


 Figure 1
Figure 1















« Prev Next »
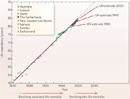
Within the United States, the twentieth century was marked by an overall increase in life expectancy of about six years in both men and women, raising the average life span to 74 years in men and almost 80 years in women. Recently, however, mortality seems to be increasing, and it appears to be doing so at different rates in different areas of the country. For example, counties along the Mississippi River and in Appalachia have shown the most significant decrease in life expectancy. Increased incidence of cancer, diabetes, chronic obstructive pulmonary disease, and cardiovascular disease (all of which are multifactorial diseases) seems to be responsible for this decline, particularly among women (Ezzati et al., 2008).
Both the marked increase in human life span that occurred in the twentieth century (Figure 1) and the recent decline in life expectancy coincided with great advances in the field of genetics. Despite these advances, scientists have yet to unravel the complex genetic mechanisms underlying the majority of common disorders, especially those that claim the lives of seemingly healthy adults. Researchers do know that genetic diseases fall into three main causative categories: defects in a single gene, mutations in multiple genes, and chromosomal abnormalities. While many genetic diseases manifest at birth, others do not show symptoms until later in life, some 30 to 70 years later. In the framework of late-onset disease, researchers know that polygenic disorders outnumber other types by orders of magnitude (Wright et al., 2003). Nonetheless, the causes of onset and progression of such disorders are poorly understood due to the complexity of the genetic mechanisms involved, as well as the interplay between these mechanisms and the environment. Some factors that trigger incurable diseases after decades of healthy life have been proposed, however. These factors, as described in the sections that follow, help explain the reasons for the marked prevalence of polygenetic disorders among the older population.
Accumulation of Harmful Mutations
A diverse and deadly list of afflictions can be categorized as late-onset disorders, including numerous cancers, Alzheimer's disease (AD), and schizophrenia, to name but a few. While some mutations that contribute to these disorders are present at birth, many more of these mutations arise from intrinsic failures of the genomic replication mechanisms within cells. Some of these failures can be traced to mutagens in the environment. In addition to causing mutations, mutagens can also trigger the expression of genes already present in the genome that are otherwise dormant. Together, this combination of accumulated harmful mutations and inappropriately activated genes can eventually manifest in pathology.
To explore this idea further, consider the example of cancer. While many people are born with genes that increase their chances of developing certain cancers, these people never manifest the disease unless specific mutations occur during the course of their lifetime. For instance, mutations in the HPC1 gene on chromosome 1 have been linked to the development of prostate cancer. Although an individual with this mutation can develop a nonmalignant polyp at a fairly young age, prostate cancer will not metastasize to the man's other organs unless a number of other tumor suppressor genes are also partially or completely disabled. Dozens of such genes have been identified to date, and researchers know that the expression of some of these genes is environmentally induced. Moreover, researchers have also noted that mutation events continue to occur after the disease phenotype has manifested, and these events are often responsible for the development of treatment resistance.
In contrast, due to the involvement of multiple genes and large variation in the severity of disease phenotype, very little is known about many of the more complex late-onset diseases, such as Alzheimer's disease and schizophrenia. AD is the most common cause of dementia in the elderly, and it is characterized physically by the presence of amyloid plaques in the patient's brain and neurofibrillary tangles in his or her nervous tissue. Surprisingly, these plaques and tangles have also been found (to a lesser extent) in the healthy aging population, so it remains unclear whether they cause the neurological symptoms of AD or are merely side effects. Recently, variation in the APOE gene, which is involved in fat metabolism, has been implicated in the formation of amyloid plaques. In healthy individuals, APOE signals the production of apolipoprotein E, which breaks down excess lipids throughout the body. This is not the case in individuals with Alzheimer's, although the exact mechanisms behind disease progression—including the role of APOE variation—are still a mystery. To further complicate matters, additional gene mutations may also have a major effect in AD. For example, approximately 5% of all AD cases are caused by autosomal dominant mutations in APP, PS1, or PS2 genes, and these cases tend to manifest before 60 years of age. In contrast, cases of AD that manifest after 60 years of age have been associated with a number of chromosomal regions, clearly suggesting the condition is a polygenic trait.
Similarly elusive are the genes involved in the onset of schizophrenia. In a commonly used method, researchers are trying to map these genes by considering their functional products. Several theories exist as to the biochemical causes of schizophrenia; the two main hypotheses involve glutamate and dopamine neurotransmitter systems (Stefansson et al., 2002), but they are unfortunately exclusive of one another. Nonetheless, most scientists agree that there is a significant genetic component in schizophrenia. Indeed, genome-wide scans employed in the search for gene variants contributing to the disease have identified multiple loci, adding schizophrenia to the growing list of major late-onset disorders whose patterns are complex and poorly understood.
Accumulated Gene Products (or Lack Thereof)
Beyond accumulated mutations, yet another mode of late-onset disease manifestation is through the accumulation of disease-causing agents that are produced from birth (or alternatively, a lack of vital substances in the body due to genetic malfunctions). This accumulation can be a gradual process, producing an imbalance that goes unnoticed for decades.
An example of this mode of affliction is Huntington's disease (HD), an autosomal dominant neurodegenerative disorder that first shows symptoms in middle adulthood. HD is characterized physiologically by a severe loss of neuronal tissue in the striatum, a structure in the brain that regulates movement and the cognitive aspects of behavior. At the molecular level, Huntington's is caused by a mutation in the HTT gene, which encodes a protein called huntingtin. Normally, each huntingtin molecule includes between six and 35 glutamine amino-acid residues as a result of CAG trinucleotide repeats in the HTT gene, but in people with HD, the number of CAG repeats is increased to between 36 and 180 (Palfi & Jarraya, 2008).
So, if this mutation is present from birth, why are the symptoms of HD not evident until adulthood? To answer this question, briefly consider the other molecular players involved in Huntington's—particularly the BDNF gene, which codes for the production of brain-derived neurotrophic factor (BDNF), a protein that has a number of important functions in the adult central nervous system. The mutated HTT gene in HD patients represses the transcriptional activity of BDNF promoters, thus impairing expression of BDNF gene. The reduction of BDNF levels over the first few decades of a person's life is asymptomatic: symptoms appear slowly and can go unnoticed for years, presenting as depression and subtle cognitive impairment while the striatal neurons progressively degenerate and die without BDNF (Zuccato & Cattaneo, 2007). The age of HD onset is also controlled by a number of modifier genes that influence BDNF levels, but their influence is not currently understood beyond association. Interestingly, physical exercise and diet significantly increase BDNF levels in the brain, and such factors are therefore being investigated for their therapeutic value.
Genetic Modifiers
As previously described, Huntington's disease is a highly penetrant single-gene disorder that manifests late in life. Although HD is caused by a mutation in a single gene, recent research indicates that the timing of its onset, however inevitable, might be regulated by a number of modifier genes. This sort of pattern of gene modification is even more complex in multifactorial genetic disorders, such as cancer and heart disease. In fact, these and other late-onset disorders show high levels of genetic variation—which is one of the reasons it is often challenging to forecast the onset and development of these conditions. This phenomenon has been attributed to the fact that the majority of late-onset disorders, by definition, manifest after people's reproductive years, thus avoiding the stringent selective constraints associated with sexual reproduction (Wright et. al., 2003). The genetic variation of late-onset disorders is also a result of the natural increase in mutation that occurs during the lifetime of any individual. Mutations arise and accumulate throughout a person's life, resulting in more potential loci that can interact to cause disease.
Recently, large studies examining genetic variation in thousands of individuals have identified the genes responsible for the most significant impacts on complex disease—in other words, the genes associated with the clearest phenotypes. However, these genome-wide association studies often overlook genetic modifiers of phenotype that have subtle or less penetrant effects due to the difficulties associated with identifying statistically significant variation in large populations. Thus, one of the central challenges in the study of common adult diseases is the need to better delineate disease mechanisms to provide new insight for preventive approaches and therapeutic targets.
References and Recommended Reading
Ezzati, M., et al. The reversal of fortunes: Trends in county mortality and cross-county morality disparities in the United States. PLoS Medicine 5, 557–568 (2008) doi:10.1371/journal.pmed.0050066
Kirkwood, T. A systematic look at an old problem. Nature 451, 644–647 (2008) doi:10.1038/451644a (link to article)
Palfi, S., & Jarraya, B. Huntington's disease lends a hand. Nature 453, 863 (2008) doi:10.1038/nature06365 (link to article)
Stefansson, H., et al. Neuregulin 1 and susceptibility to schizophrenia. American Journal of Human Genetics 71, 877–892 (2002)
Wright, A., et al. A polygenic basis for late-onset disease. Trends in Genetics 19, 97–105 (2003)
Zuccato, C., & Cattaneo, E. Role of brain-derived neurotrophic factor in Huntington's. Progress in Neurobiology 81, 294–330 (2007)










