
Abstract
Intrinsic capacity (IC), a function-centered construct, is defined as the composite of all physical and mental capacities of an individual. IC and surrounding environmental factors determine an individual’s functional ability to do what they want or feel valued. Current literature lacks evidence on how IC varies throughout adulthood. In this study, we demonstrated a method to establish age-specific and sex-specific reference centiles for IC using the Human Translational Research Cohort of the INSPIRE Platform (975 adults, aged 20–102 years, living in the southwest France, Toulouse area). IC was operationalized as the mean score of the five key domains (cognition, locomotion, psychology, sensory and vitality) and the factor score from a bifactor model, respectively. Both IC operationalizations showed higher IC levels in young and middle age and markedly lower levels after age 65 years, with greater inter-individual variation in old age than in youth. Individuals with IC ≤10th percentile tended to have high comorbidity, prefrailty/frailty, difficulties in basic and instrumental activities of daily living and falls than individuals with IC >90th percentile. These findings suggest that IC reference centiles can help monitor the functional capacity of individuals during aging, similar to tracking children’s development with growth charts.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$29.99 / 30 days
cancel any time
Subscribe to this journal
Receive 12 digital issues and online access to articles
$119.00 per year
only $9.92 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others
Data availability
The data underlying the results reported in this manuscript (that is, text, tables, figures and the supplementary information) will be shared in de-identified form owing to privacy protections. Request for de-identified data and a data dictionary will be evaluated by the INSPIRE data access committee, which can be contacted at the following addresses: guyonnet.s@chu-toulouse.fr and nicola.coley@inserm.fr. Data will be made available for other researchers upon reasonable request for a specified scientific purpose outlined in a methodologically sound research proposal, subject to the approval of the appropriate INSPIRE committee and after signing a data use agreement.
Given the ongoing nature of the INSPIRE-T study, the authors are unable to make the dataset publicly accessible at this time. In addition, according to the INSPIRE policy, all analyses using INSPIRE-T data (including the present study) should be first evaluated and approved by the committee after submission of a comprehensive analysis proposal. Therefore, for researchers interested in accessing the data used for the current study, the same evaluation procedure should be followed.
Code availability
The code that supports the results of the present study is available from the corresponding authors upon reasonable request. All models were built using publicly available packages and functions in the R and SAS programming languages.
References
Beard, J. R. et al. The World report on ageing and health: a policy framework for healthy ageing. Lancet 387, 2145–2154 (2016).
Cesari, M. et al. Evidence for the domains supporting the construct of intrinsic capacity. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 73, 1653–1660 (2018).
Tay, L. et al. Association of intrinsic capacity with frailty, physical fitness and adverse health outcomes in community-dwelling older adults. J. Frailty Aging. 12, 7–15 (2023).
González-Bautista, E., de Souto Barreto, P., Andrieu, S., Rolland, Y. & Vellas, B. Screening for intrinsic capacity impairments as markers of increased risk of frailty and disability in the context of integrated care for older people: secondary analysis of MAPT. Maturitas 150, 1–6 (2021).
Ma, L. et al. Cross-sectional study examining the status of intrinsic capacity decline in community-dwelling older adults in China: prevalence, associated factors and implications for clinical care. BMJ Open 11, e043062 (2022).
Stolz, E., Mayerl, H., Freidl, W., Roller-Wirnsberger, R. & Gill, T. M. Intrinsic capacity predicts negative health outcomes in older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 77, 101–105 (2022).
Meng, L.-C., Huang, S.-T., Peng, L.-N., Chen, L.-K. & Hsiao, F.-Y. Biological features of the outcome-based intrinsic capacity composite scores from a population-based cohort study: pas de deux of biological and functional aging. Front. Med. (Lausanne) 9, 851882 (2022).
World Health Organization. Integrated care for older people (ICOPE): guidance for person-centred assessment and pathways in primary care. https://www.who.int/publications/i/item/WHO-FWC-ALC-19.1 (2019).
López-Ortiz, S. et al. Defining and assessing intrinsic capacity in older people: a systematic review and a proposed scoring system. Ageing Res. Rev. 79, 101640 (2022).
Beard, J. R., Jotheeswaran, A. T., Cesari, M. & Araujo de Carvalho, I. The structure and predictive value of intrinsic capacity in a longitudinal study of ageing. BMJ Open 9, e026119 (2019).
Beard, J. R., Si, Y., Liu, Z., Chenoweth, L. & Hanewald, K. Intrinsic capacity: validation of a new WHO concept for healthy aging in a longitudinal Chinese study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 77, 94–100 (2022).
World Health Organization. WHO Clinical Consortium on Healthy Ageing: topic focus—frailty and intrinsic capacity. https://www.who.int/publications/i/item/WHO-FWC-ALC-17.2 (2017).
Cesari, M., Vanacore, N. & Agostoni, C. The two extremes meet: pediatricians, geriatricians and the life-course approach. Pediatr. Res. 86, 432–435 (2019).
Beard, J. R. & Chen, M. Intrinsic capacity as a composite outcome measure: opportunities and challenges. J. Nutr. Health Aging 27, 398–400 (2023).
Ghosh, A., Millett, C., Subramanian, S. V. & Pramanik, S. Neighborhood heterogeneity in health and well-being among the elderly in India—evidence from Study on global AGEing and adult health (SAGE). Health Place 47, 100–107 (2017).
Belloni, G. & Cesari, M. Frailty and intrinsic capacity: two distinct but related constructs. Front. Med. (Lausanne) 6, 133 (2019).
Liu, S. et al. Trajectory and correlation of intrinsic capacity and frailty in a Beijing elderly community. Front. Med. (Lausanne) 8, 751586 (2021).
Tay, L., Tay, E. L., Mah, S. M., Latib, A. & Ng, Y. S. Intrinsic capacity rather than intervention exposure influences reversal to robustness among prefrail community-dwelling older adults: a non-randomized controlled study of a multidomain exercise and nutrition intervention. Front. Med. (Lausanne) 9, 971497 (2022).
Cole, T. J. Sample size and sample composition for constructing growth reference centiles. Stat. Methods Med. Res. 30, 488–507 (2021).
de Souto Barreto P. et al. The INSPIRE research initiative: a program for GeroScience and healthy aging research going from animal models to humans and the healthcare system. J. Frailty Aging 10, 86–93 (2021).
Guyonnet, S. et al. The INSPIRE bio-resource research platform for healthy aging and geroscience: focus on the human translational research cohort (the INSPIRE-T cohort). J. Frailty Aging 10, 110–120 (2021).
Folstein, M. F., Folstein, S. E. & McHugh, P. R. ‘Mini-mental state’: a practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 12, 189–198 (1975).
Guralnik, J. M. et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J. Gerontol. 49, M85–M94 (1994).
Kroenke, K., Spitzer, R. L. & Williams, J. B. W. The PHQ-9: validity of a brief depression severity measure. J. Gen. Intern. Med. 16, 606–613 (2001).
Bautmans, I. et al. WHO working definition of vitality capacity for healthy longevity monitoring. Lancet Health Longev. 3, e789–e796 (2022).
Granic, A. et al. Initial level and rate of change in grip strength predict all-cause mortality in very old adults. Age Ageing 46, 970–976 (2017).
Sasaki, H., Kasagi, F., Yamada, M. & Fujita, S. Grip strength predicts cause-specific mortality in middle-aged and elderly persons. Am. J. Med. 120, 337–342 (2007).
Lu, W.-H. et al. Plasma inflammation‐related biomarkers are associated with intrinsic capacity in community‐dwelling older adults. J. Cachexia Sarcopenia Muscle 14, 930–939 (2023).
Charlson, M. E., Pompei, P., Ales, K. L. & MacKenzie, C. R. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J. Chronic Dis. 40, 373–383 (1987).
Liu, H. et al. Effect of comorbidity assessed by the Charlson comorbidity index on the length of stay and mortality among immobile hemorrhagic stroke patients younger than 50 years. Front. Neurol. 11, 487 (2020).
Fried, L. P. et al. Frailty in older adults: evidence for a phenotype. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 56, M146–M157 (2001).
Katz, S., Downs, T. D., Cash, H. R. & Grotz, R. C. Progress in development of the index of ADL. Gerontologist 10, 20–30 (1970).
Lawton, M. P. & Brody, E. M. Assessment of older people: self-maintaining and instrumental activities of daily living. Gerontologist 9, 179–186 (1969).
Ferrucci, L. et al. Subsystems contributing to the decline in ability to walk: bridging the gap between epidemiology and geriatric practice in the InCHIANTI study. J. Am. Geriatr. Soc. 48, 1618–1625 (2000).
Box, G. E. P. & Cox, D. R. An analysis of transformations. J. R. Stat. Soc. Ser. B 26, 211–252. (1964).
Cole, T. J. The LMS method for constructing normalized growth standards. Eur. J. Clin. Nutr. 44, 45–60 (1990).
Rigby, R. A. & Stasinopoulos, D. M. Smooth centile curves for skew and kurtotic data modelled using the Box-Cox power exponential distribution. Stat. Med. 23, 3053–3076 (2004).
Rigby, R. A. & Stasinopoulos, D. M. Using the Box-Cox t distribution in GAMLSS to model skewness and kurtosis. Stat. Modelling 6, 209–229 (2006).
Cole, T. J. & Green, P. J. Smoothing reference centile curves: the LMS method and penalized likelihood. Stat. Med. 11, 1305–1319 (1992).
Van Buuren, S. & Fredriks, M. Worm plot: a simple diagnostic device for modelling growth reference curves. Stat. Med. 20, 1259–1277 (2001).
Aliberti, M. J. R. et al. Validating intrinsic capacity to measure healthy aging in an upper middle-income country: findings from the ELSI-Brazil. Lancet Reg. Health Am. 12, 100284 (2022).
Andrieu, S. et al. Effect of long-term omega 3 polyunsaturated fatty acid supplementation with or without multidomain intervention on cognitive function in elderly adults with memory complaints (MAPT): a randomised, placebo-controlled trial. Lancet Neurol. 16, 377–389 (2017).
Acknowledgements
The INSPIRE platform was supported by grants from the Region Occitanie/Pyrénées-Méditerranée (reference no.: 1901175) and the European Regional Development Fund (ERDF) (project no.: MP0022856) and the Inspire Chairs of Excellence funded by: Alzheimer Prevention in Occitania and Catalonia (APOC), EDENIS, KORIAN, Pfizer and Pierre-Fabre.
W.-H.L. has been partially supported through the grant EUR CARe N°ANR-18-EURE-0003 in the framework of the Programme des Investissements d’Avenir.
The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Members of the INSPIRE platform group:
INSPIRE-T human cohort group: coordinators: S. Guyonnet and B. Vellas; project managers: L. Brigitte and A. Milhet; clinical research assistants: E. Paez, E. Muller and S. Le Floch; investigators: C. Takeda, C. Faisant, F. Lala, G. Abellan Van Kan, Z. Steinmeyer, A. Piau, T. Macaron, D. Angioni and P.-J. Ousset; nurses: M. Comté, N. Daniaud and F. Boissou-Parachaud; methodology, statistical analysis and data management subgroup: S. Andrieu and C. Cantet; body composition, VO2 max and isocinetism subgroup: Y. Rolland, P. de Souto Barreto and F. Pillard; technician DXA: B. Teysseyre; MRI subgroup: M. Faruch and P. Payoux; ICOPE subgroup: C. Takeda and N. Tavassoli; and biological sample collection subgroup: M. Dorard, B. Razat, C. Champigny and S. Guyonnet.
INSPIRE animal cohort groups: C. Dray and J.-P. Pradère (fish colony) and A. Parini and Y. Santin (murine cohort).
Associated research teams: D. Langin, P. Gourdy, L. Martinez, A. Bouloumié and A. Parini (I2MC lab); N. Fazilleau, R. Liblau, J.-C. Guéry, M. Simon, N. Gaudenzio, L. Bostan, H. El Costa and N. J. Ferrat (Infinity lab); P. Valet, C. Dray, I. Ader and V. Planat (Restore); P. Payoux and P. Peran (Tonic lab); C. Delpierre and S. Andrieu (CERPOP lab); C. Rampon, N. Davezac and B. Guiard (CRCA/CBI lab); N. Vergnolles, J.-P. Motta, S. Djelabi and P. Floch (IRSD lab); and J.-E. Sarry (CRCT lab).
Author information
Authors and Affiliations
Contributions
W.-H.L. designed and conceptualized the research, performed the analyses, interpreted the data and drafted the manuscript. Y.R. and S.G. revised the draft critically for important intellectual content. P.S.d.B. designed and conceptualized the research, interpreted the data and revised the draft critically for important intellectual content. B.V. conceived the INSPIRE platform, interpreted the data and revised the draft critically for important intellectual content. All authors have read and agreed with the final version to be submitted.
Corresponding author
Ethics declarations
Competing interests
B.V. is the founder president of IHU HealthAge at Toulouse University Hospital and is an investigator in clinical trials sponsored by several industry partners (IHU and the INSPIRE geroscience platform). Other authors report no competing interests.
Peer review
Peer review information
Nature Aging thanks Jean Woo and the other, anonymous, reviewer(s) for their contribution to the peer review of this work.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 Sensitivity analysis on the IC factor score extracted from the CFA bifactor model showed a similar distribution across age as the IC mean score.
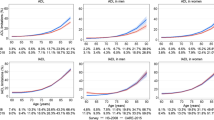
a. Scatterplot of the IC factor score among the 948 INSPIRE-T participants aged 20 to 102 (588 women and 360 men). Red represents women, and blue represents men. Like the distribution of the IC mean score, the IC factor score showed a negative, non-linear association with age. b,c. Smoothed reference centile curves for the IC factor score based on the INSPIRE-T cohort, derived using the LMS method (b for female and c for male). Seven percentile curves are shown: 3rd, 10th, 25th, 50th, 75th, 90th, and 97th. Numerical results of IC reference values for each percentile curve are provided in Supplementary Table 1.
Extended Data Fig. 2 Sensitivity analysis on the subgroup younger than 70 using four cognitive tests to assess the cognitive domain.
A composite measure of four cognitive tests – the Free and Cued Selective Reminding Test (FCSRT), the Digit Symbol Substitution Test (DSST), the Category Naming Test (CNT), and ten MMSE orientation items – was used to assess the cognitive domain of IC. a. Scatterplot of IC across age among 575 participants younger than 70, stratified by sex (379 women and 196 men). b,c. Smoothed reference centile curves for IC based on the INSPIRE-T cohort, derived using the LMS method (b for female and c for male). Seven percentile curves are shown: 3rd, 10th, 25th, 50th, 75th, 90th, and 97th. Numerical results of IC reference values for each percentile curve are provided in Supplementary Table 2.
Extended Data Fig. 3 All participants with IC ≤ P10 had at least one abnormal IC domain identified by the ICOPE Step 1 tools.
We examined the number of IC domains with potential abnormality according to the WHO ICOPE Step 1 screening tools among subjects with available data (n = 960). The details of the ICOPE Step 1 screening tools are summarized in Extended Data Table 3. This figure illustrates how individuals are distributed within each IC centile category based on the number of abnormal IC domains ranging from 0 to 6. Values in the bars indicate the participant numbers and percentages. All participants with IC ≤ P10 had at least one abnormal IC domain identified by the ICOPE Step 1 tools. Participants with IC > P90 tended to have fewer abnormal domains.
Supplementary information
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Lu, WH., Rolland, Y., Guyonnet, S. et al. Reference centiles for intrinsic capacity throughout adulthood and their association with clinical outcomes: a cross-sectional analysis from the INSPIRE-T cohort. Nat Aging 3, 1521–1528 (2023). https://doi.org/10.1038/s43587-023-00522-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s43587-023-00522-x
