
Abstract
There is still a lot of ambiguity about the link between physical activity (PA), sedentary behaviors (SBs) and osteoarthritis (OA). This study aimed to investigate the causal relationship of PA/SBs on the risk of OA. A univariate and multivariate Mendelian randomization (MR) analysis was conducted to investigate the causal effect of five PA phenotypes and three SB phenotypes on overall OA, knee OA, hip OA, total hip arthroplasty, and total knee arthroplasty (TKA). MR methods used were inverse-variance weighting, MR-Egger regressions, and weighted median. Sensitivity analysis examined horizontal pleiotropy and heterogeneity, and confirmed the reliability of the results. After false discovery rate, light do-it-yourself (DIY) activities decreased the risk for overall OA (OR: 0.32, 95% CI 0.16–0.65), and knee OA (OR: 0.26, 95% CI 0.12–0.51). Resulting in a decreased risk of walking for pleasure on overall OA (OR: 0.87, 95% CI 0.70–1.04) and knee OA (OR: 0.14, 95% CI 0.06–0.32) was also observed. Television viewing, however, significantly increased the risk of OA, knee OA, hip OA, and TKA. MVMR findings revealed independent causal impacts of walking for pleasure and watching television on overall and knee OA, taking into account BMI, smoking, and education. This study suggested that light DIY and walking for pleasure were beneficial for preventing OA, and the risk of OA and TKA increased with prolonged television watching.
Similar content being viewed by others


Introduction
The most common degenerative joint disease for the aging population, osteoarthritis (OA), ranks fifth in global disability causes1. The number of people suffering from OA worldwide exceeds 300 million, especially knee and hip OA2. In spite of the fact that OA risk factors, including female sex, obesity, joint injuries, and high bone mineral density, it remains a priority to study modifiable variables that can prevent OA's pain and impairment3.
As a public health intervention, many major diseases can be treated through physical activity (PA), including cardiovascular disease, diabetes, and obesity4,5. However, there is still a lot of ambiguity about the link between PA and OA. Although evidence suggests that PA such as strengthening exercises and aerobic walking, is beneficial for reducing pain and improving the physical function of OA patients6,7, studies have shown that high levels of PA can lead to knee structural damage and increase the risk for knee arthroplasty8,9. Moreover, a Danish trial revealed that the improvement of exercise after 9 weeks was also similar, with no essential difference in comparison with the placebo10. The contextual effects seem to explain essentially all the improvement after an exercise intervention11. On the other hand, sedentary behaviors (SBs), such as sitting for prolonged periods, could increase the risk of OA12. Nevertheless, it is likely that observational studies were confounded by inverse causality or confounding variables, which potentially results in biased associations and conclusions. Therefore, it is unclear how PA and SBs link to OA and whether or not there are separate causal associations.
In order to discover single nucleotide polymorphisms (SNPs) associated with common complex diseases, genome-wide association studies (GWAS) have been greatly helpful13. It can comprehend the genetic underpinnings of several complicated features in widespread human illnesses. Genetic variants are used as instrumental variables (IV) in Mendelian randomization (MR) to examine risk variables and disease outcomes14. It is possible to exclude confounding factors and identify causal factors of a specific outcome by MR analysis since genetic variants are assigned randomly before disease onset15.
In this study, a particular focus was placed on exploring the potential causal effects of five phenotypes of PA and three phenotypes of SBs on different OA subtypes and relevant arthroplasty using large-scale GWAS data. As a result, this study assessed the impact of physical activity on OA, identified a potentially susceptible sedentary population, and provided recommendations for OA prevention.
Methods
Study design overview
This MR study was designed as shown in Fig. 1. To examine the causal effects, a univariable MR analysis (UVMR) was performed between PA/SBs and OA/TJA using GWAS summary statistics first, then potential mediators correlated with PA/SBs were evaluated in the risk factors analysis, and validated by multivariable MR analysis (MVMR). The random distribution of SNPs in offspring is mimicked by this instrumental-variable analysis similar to RCT. Only genetic variants that meet the following three requirements can be considered IVs16. As noted above, genetic variants have a strong correlation with exposure. As well as this, genetic variants don't correlate with confounders. Lastly, genetic variants cannot directly influence outcomes. STROBE-MR guidelines were followed for the analysis17.

Study design overview. OA, osteoarthritis; TKA, total knee arthroplasty; THA, total hip arthroplasty; SNP, single nucleotide polymorphism; MR, Mendelian randomization; MR-PRESSO, Mendelian Randomization Pleiotropy RESidual Sum and Outlier.
Data sources and instrumental variable selection
The UK Biobank is a large prospective cohort study including half a million volunteer participants in the United Kingdom aged between 40 and 69 years. The UK Biobank has genotyped the DNA from participants' blood samples. This genetic data provides information about participants' genetic variations, which can be linked to various health outcomes. Summary-level GWAS from the UK Biobank of 460,376 participants was used to construct instrumental variables for PA18,19, which included five phenotypes: light do-it-yourself (DIY) (eg., pruning, watering the lawn), heavy DIY (eg., weeding, lawn mowing, carpentry, digging), walking for pleasure, strenuous sports, and other exercises. At the time of enrollment, data on PA were gathered using items modified from the well-validated International Physical Activity Questionnaire (IPAQ). Participants, where appropriate, indicated their participation (yes or no), frequency (days/week), and/or length (minutes/day) for each specified physical activity. Full details of instrumental variable selection are given in Appendix 1. Finally, 12, 18, 20, 6, and 15 SNPs were used as IVs for light DIY, heavy DIY, walking for pleasure, strenuous sports, and other exercises in our study, respectively.
From the UK Biobank's latest summary-level GWAS of 422,218 participants, we identified candidate genetic instruments associated with SBs20. Answers to the questions “How many hours do you spend watching TV/driving/using the computer (Do not include using a computer at work) in a typical day?” were used to calculate the amount of time participants spent on each behavior. GWAS meta-analyses included three categories of IVs for SBs: television watching, computer use, and driving. After adjusting covariates, 151, 47, and 5 SNPs were used as IVs for television watching, computer use, and driving.
From the latest publicly available GWAS with up to 826,690 participants from the Genetics of Osteoarthritis (GO) Consortium, we compiled summary statistics for overall OA, knee OA, hip OA, total knee arthroplasty (TKA), and total hip arthroplasty (THA)21. Based on the TREAT-OA consortium's definition, OA cases were defined based on self-reported, hospital diagnoses, ICD10 codes, or radiographic findings. Variants were grouped according to which OA site they were associated with. A detailed list of SNPs for PA/SBs on OA and TJA is presented in Supplementary file 1, Tables S1–S5.
Univariable MR analysis
In this study, Two-sample MR (version 0.5.6) and MRPRESSO (version 1.0) packages with R software (version 4.2.2) were used for UVMR. We estimated the causal effects of genetically predicted exposure on the outcome using the inverse-variance-weighted (IVW) method as our primary MR analysis method22. Additionally, MR-Egger regression and weighted median method were implemented in addition to the IVW, since these methods can provide more comprehensive estimates23,24. IVW analyses were conducted using a false discovery rate (FDR) adjusted P-value (also known as q-value) for testing multiple hypotheses. A significance level of less than 0.05 was set for causal inference. Additionally, binary outcomes were used to calculate the post-hoc power using an online power calculation (https://shiny.cnsgenomics.com/mRnd/).
Sensitivity analysis
When genetic variations linked to exposure of interest have a direct impact on the result via multiple pathways other than the expected exposure, this is known as horizontal pleiotropy25. To assess whether the results were robust and pleiotropic, we performed Cochran's Q statistics, MR-Egger intercept tests, funnel pot analyses, and leave-one-out analyses25. In particular, Cochran Q tests were used to detect heterogeneity if the P value is less than 0.05. Additionally, we evaluated horizontal pleiotropy using the intercept term derived from MR-PRESSO26. Moreover, the Steiger test was utilized to validate whether the observed causalities were biased owing to reversed causation.
Multivariable MR analysis
MVMR extends UVMR by including all factors in the same model and estimating their causal effects jointly on OA risk27. Three potential mediators (BMI28, smoking29, and education30) that had strong genetic correlations with PA/SBs were chosen. In the MVMR analysis, the mediation effect of these exposures was validated simultaneously, and the mediation effect of single exposures was estimated separately. To infer causal effects in MVMR, weighted linear regression-based IVW and MR-Egger approaches were used. MVMR was carried out by Mendelian Randomization (version 0.7.0) and MVMR (version 0.3.0) packages.
Ethics approval and consent to participate
This manuscript does not include clinical studies or patient data. All data is exchanged from public open databases thus avoiding ethical disputes.
Results
Univariable MR analysis
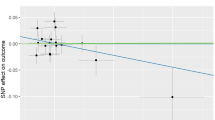
As shown in Table 1, eight out of forty exposure-outcome associations retained significant and determined to be causal effects connected with overall OA, knee OA, hip OA, and TKA, after FDR adjustment. A causal association was found between light DIY and overall OA (OR: 0.319, 95% CI 0.158–0.646, q = 0.011), and knee OA (OR: 0.258, 95% CI 0.116–0.570, q = 0.008). In addition, walking for pleasure was associated with a decreasing risk of overall OA (OR: 0.869, 95% CI 0.702–1.042, q = 0.016), and knee OA (OR: 0.136, 95% CI 0.059–0.318, q = 5.65 × 10–5). In contrast, a significant association was found between genetically proxied television watching and overall OA (OR: 1.988, 95% CI 1.637–2.413, q = 1.44 × 10–10), knee OA (OR: 1.637, 95% CI 1.396–1.920, q = 2.66 × 10–8), hip OA (OR: 1.318, 95% CI 1.110–1.565, q = 0.011), and TKA (OR: 1.104, 95% CI 1.001–1.207, q = 0.021). Additionally, genetic liability was not associated with heavy DIY, strenuous sports, other exercises, computer use, or driving on the risk of OA and TJA. The scatter plots (Fig. 2A-H) showed a significant causal relationship between PA/SBs and OA/TJA risk.

Scatterplots showing the effect of SNPs on the outcome (y-axis) and exposure (x-axis) with significant effect sizes with 95% confidence intervals. Slopes represent estimates for three different MR modes. Radiation SNP effects are plotted as standard deviation (SD) per unit and outcomes (total OA, knee OA, hip OA, and TKA) are plotted as log probability per unit of expression. (A, B) the association between light DIY and the risk of overall OA and knee OA; (C, D) the association between walking for pleasure and the risk of overall OA and knee OA; (E, H) the association between television watching and risk of overall OA, knee OA, hip OA, and TKA. SNPs, single nucleotide polymorphisms; MR, Mendelian randomization; OA, osteoarthritis; TKA, total knee arthroplasty.
Sensitivity analysis
As shown in Table 2, according to the MR-Egger intercept test, all P values were greater than 0.05, thus indicating no horizontal pleiotropy. Analyzing the Q test, heterogeneity was observed between walking for pleasure and overall OA, and television watching and overall OA, Hip OA, and TKA (P < 0.05). The global test of MR-PRESSO eliminated horizontal pleiotropy, indicating that MR estimates were not biased in the context of heterogeneity. All the Steiger P values were less than 0.05, suggesting that no reverse causality bias was found in the identified causalities. Moreover, the estimation was unaffected by any SNP with a substantial impact size, according to the leave-one-out test (Supplemental Figs. 1–2). Forest plots (Supplementary Figs. 3–4) were observed in the MR-SingleSNP test for causal effects of causal PA/SBs associated with single SNPs. Funnel plots were symmetrical, indicating that the estimates were not violated (Supplemental Fig. 5).
A summary of all the causal effects can be seen in Fig. 3. and Supplementary file 2, Table S6. Summary data of sensitivity analysis of all the MR assumptions were indicated in Supplementary file 2, Table S7. Except for television watching to TKA, all statistical powers of significance were greater than 60% (Supplementary file 2, Table S8), and the F statistic for each exposure exceeded the empirical threshold of 10 (Supplementary file 1, Tables S1–S5). Additionally, each SNP was checked in Phenoscanner's genetic instrument to assess whether prospective risk factors violated it (Supplementary file 2, Table S9). We did not detect any potential risk factors that compromised the robustness of our causality estimations.

A panorama of all PA/SB causality estimates for osteoarthritis and total joint arthroplasty, determined according to the nominal significance of P values and q-values (FDR-adjusted). PA, physical activity; SBs, sedentary behaviors; OA, osteoarthritis; TKA, total knee arthroplasty; THA, total hip arthroplasty; FDR, false discovery rate. * and *** represent the significance of the P value and q value, respectively.
Multivariable MR analysis
In MVMR analysis, BMI, smoking, and education were taken into consideration to determine whether PA/SBs were associated with OA in an independent causal manner. Walking for pleasure had an independent causal effect on overall OA (OR: 0.235, 95% CI 0.076–0.723), and knee OA (OR: 0.284, 95% CI 0.123–0.657). Moreover, television watching was strongly associated with a directed causal effect on OA risk (OR: 1.858, 95% CI 1.157–2.986), knee OA (OR: 1.936, 95% CI 1.367–2.742), and TKA (OR: 1.109, 95% CI 1.002–1.216) (Fig. 4). No causal association was found between light DIY and OA, and watching TV and hip OA. The estimated effects between IVW and Egger analysis were similar, and MVMR model estimates were not distorted by directional pleiotropy since all P values for MVMR-Egger intercept tests exceeded thresholds of 0.05 (Supplementary file 2, Table S10).

Forest plots of multivariate Mendelian randomization analyses examined causal associations between PA/SB and OA and arthroplasty, adjusted for BMI, smoking status, and education. Estimates of causality were expressed as odds ratios (ORs) and 95% confidence intervals (CIs). PA, physical activity; SBs, sedentary behaviors; OA, osteoarthritis; TKA, total knee arthroplasty.
Discussion
The present study is the first to comprehensively and deeply examine the causal effects of PA/SBs on OA and TJA using GWAS summary-level data. To identify causal effects, multivariate and univariate MR analyses were conducted on 40 potential associations and found that light DIY, walking for pleasure, and television watching were associated with the risk of OA and TJA.
Previous studies indicated that controversy still existed on the relationship between PA and OA7,8,9,31,32. According to the current study, increased levels of light DIY and walking for pleasure were associated with an increased risk of OA in both the knee and overall. Although the results from other patterns like heavy DIY, strenuous sports, and other exercises showed a consistent trend, nonsignificant causal associations were detected. Several studies have linked PA with OA, consistent with our findings. Chang et al.31 followed 1194 participants for over 10 years in a cohort study and reported no association between long-term strenuous PA and knee OA. The study also indicated that a low-to-moderate level of PA displayed a protective effect on knee OA. Bell et al.33 conducted a systematic review of 28 RCTs with 2,789 participants and indicated that people with knee OA may benefit from walking and mixed exercise, but not from resistance training. A systematic review and population modeling study found that even relatively modest intensity bouts of PA could help maintain or improve the life quality of OA patients compared with typical levels of sedentariness34,35. In cohort studies of healthy adults, PA at low or moderate intensities improved cartilage, thereby possibly preventing OA degeneration36,37. Although it has been suggested that high levels of PA in patients with OA may damage articular joint cartilage and increase the risk for TJA, it is unclear whether such structural damage actually causes OA38. We hypothesize that the potential damage of high levels of PA dampens its beneficial effects on OA, which weakened the causal relationship of heavy DIY and strenuous sports with OA in this literature. The underlying mechanism linking different types of PA to hip/knee OA remains inclusive, which is therefore necessary to further examine.
Television watching was shown to be a risk factor for OA, knee OA, hip OA, and TKA in this study by robust genetic evidence. Notably, we think that OA was induced by the sedentary behavior caused by TV viewing, not the TV watching itself. SBs and OA have been associated in previous observational studies12,39,40. These studies specifically demonstrated that sedentary behavior could increase the risk of developing knee and hip OA, and reducing sedentary time helped OA patients feel less pain and exhaustion, which in turn enhanced their quality of life. In comparison to other sedentary behaviors, there is evidence that watching leisure television leads to an increase in food intake and energy intake as well as a decrease in physical activity41,42. It is possible that watching television contributes to a surplus of energy by decreasing rest time, lowering energy expenditure, and consuming too much energy41. Additionally, watching television is a less cognitive and conversational form of leisure and entertainment than using the computer or driving42. Further, television watching specifically impacts the mental and physical health of individuals (such as anxiety and sadness)43. Hence, television watching, as a unique sedentary behavior, affects the development of OA in a specific way.
Prior MR analysis indicated that several risk factors might affect these causal inferences. Smoking status plays a significant role in the development of OA, and has been indicated as an independent deleterious causal effect upon OA by MR analysis44. Substantial evidence suggested that OA burden and TKA costs were likely to increase significantly with obesity45. Higher education was also substantiated as a protective factor for OA30. However, these potential mediators need to be further validated in multivariate MR analysis. Taking the effects of these potential mediators into consideration, MVMR results showed that the independent causal effects of walking for pleasure and television watching suggested the direct genetic associations with overall OA and knee OA, which had been overlooked in the previous studies. After adjustment for potential mediators, light DIY displayed no causal association with overall OA and knee OA, which implies that the causality between light DIY and OA may be mediated by smoking and education. Even though MVMR can assess PA/SBs' unconfounded effect on OA risk, the degree to which BMI, smoking, and education affect this effect cannot be determined. Consequently, the precise degree of crucial intermediate elements in PA/SBs for OA and TJA needs to be explored in further studies.
In comparison with observational studies, the primary advantage of this study is the use of an MR design, which is less susceptible to confounding and does not suffer from time-related bias. STROBE-MR guidelines were strictly followed in this MR study. Our study examined genetically predicted exposures to OA with data from the largest summary-level dataset available for this disease. Demographic stratification was eliminated by restricting the included participants to the European population. A variety of methods were also applied in our study, including sensitivity analyses and MVMR analyses, to improve the reliability of causal conclusions.
The MR approach has several limitations. First, age and gender are known to be significant risk factors for OA. It is difficult, however, to establish any nonlinear relationships or stratification effects using summary-level data. Second, the summary GWAS data only included European individuals, making it difficult to explain our findings across the entire population. Third, we were not able to measure PA/SBs by metabolic equivalent (MET) because there were no relevant databases. The causality link between PA/SBs and OA/TJA needs to be further confirmed, and potential mechanisms need to be explored to develop relevant clinical recommendations.
Conclusion
Overall, the research suggests that light DIY and walking for pleasure are important factors in the prevention of OA, while sedentary behavior caused by television watching may increase the risk of OA and TKA. People who are at risk for osteoarthritis should aim to engage in a regularly low-to-moderate level of PA, and try to reduce television watching time. This research examines the potential causal relationship between PA/SBs and OA/TJA, and may help identify new treatment and rehabilitation strategies to address this condition.
Data availability
The information utilized to produce the study's findings of osteoarthritis was gathered from the publicly available Genetic Consortium genome association from the website https://msk.hugeamp.org/downloads.html. The data on physical activity and sedentary behaviors were downloaded from the UK biobank from the website https://www.ukbiobank.ac.uk/. The data upon which this paper is based can be found in this paper and its online supplement.
Abbreviations
- GWAS:
-
Genome-wide association studies
- SNP:
-
Single nucleotide polymorphism
- IV:
-
Instrumental variable
- MR:
-
Mendelian randomization
- IVW:
-
Inverse variance weighted
- MR-PRESSO:
-
Mendelian Randomization Pleiotropy RESidual Sum and Outlier
- PA:
-
Physical activity
- SBs:
-
Sedentary behaviors
- OA:
-
Osteoarthritis
- DIY:
-
Do-it-yourself
- TKA:
-
Total knee arthroplasty
- THA:
-
Total hip arthroplasty
- TJA:
-
Total joint arthroplasty
- FDR:
-
False discovery rate
- BMI:
-
Body mass index
- BMD:
-
Bone mineral density
References
Katz, J. N., Arant, K. R. & Loeser, R. F. Diagnosis and treatment of hip and knee osteoarthritis: A review. JAMA 325, 568–578. https://doi.org/10.1001/jama.2020.22171 (2021).
Quicke, J. G., Conaghan, P. G., Corp, N. & Peat, G. Osteoarthritis year in review 2021: Epidemiology & therapy. Osteoarthr. Cartil. 30, 196–206. https://doi.org/10.1016/j.joca.2021.10.003 (2022).
Latourte, A., Kloppenburg, M. & Richette, P. Emerging pharmaceutical therapies for osteoarthritis. Nat. Rev. Rheumatol. 16, 673–688. https://doi.org/10.1038/s41584-020-00518-6 (2020).
Patnode, C. D., Redmond, N., Iacocca, M. O. & Henninger, M. Behavioral counseling interventions to promote a healthy diet and physical activity for cardiovascular disease prevention in adults without known cardiovascular disease risk factors: Updated evidence report and systematic review for the us preventive services task force. JAMA 328, 375–388. https://doi.org/10.1001/jama.2022.7408 (2022).
Bichsel, D., Liechti, F. D., Schlapbach, J. M. & Wertli, M. M. Cross-sectional analysis of recommendations for the treatment of hip and knee osteoarthritis in clinical guidelines. Arch. Phys. Med. Rehabil. 103, 559-569.e555. https://doi.org/10.1016/j.apmr.2021.07.801 (2022).
Nelligan, R. K., Hinman, R. S., Kasza, J., Crofts, S. J. C. & Bennell, K. L. Effects of a self-directed web-based strengthening exercise and physical activity program supported by automated text messages for people with knee osteoarthritis: A randomized clinical trial. JAMA Intern. Med. 181, 776–785. https://doi.org/10.1001/jamainternmed.2021.0991 (2021).
Daste, C. et al. Physical activity for osteoarthritis: Efficiency and review of recommandations. Joint Bone Spine 88, 105207. https://doi.org/10.1016/j.jbspin.2021.105207 (2021).
Hu, B., Han, D., Nevitt, M. C., Wise, B. L. & Segal, N. A. Longitudinal relationship between physical activity and joint space narrowing: Forty-eight-month follow-up data from the osteoarthritis initiative. Arthritis Care Res (Hoboken) 74, 1163–1171. https://doi.org/10.1002/acr.24554 (2022).
Voinier, D. & White, D. K. Walking, running, and recreational sports for knee osteoarthritis: An overview of the evidence. Eur. J. Rheumatol. https://doi.org/10.5152/eurjrheum.2022.21046 (2022).
Henriksen, M. et al. Exercise and education vs intra-articular saline for knee osteoarthritis: A 1-year follow-up of a randomized trial. Osteoarthr. Cartil. 31, 627–635. https://doi.org/10.1016/j.joca.2022.12.011 (2023).
Englund, M. & Turkiewicz, A. The emperor’s new clothes?. Osteoarthr. Cartil. 31, 549–551. https://doi.org/10.1016/j.joca.2023.02.001 (2023).
Zhaoyang, R., Martire, L. M. & Darnall, B. D. Daily pain catastrophizing predicts less physical activity and more sedentary behavior in older adults with osteoarthritis. Pain 161, 2603–2610. https://doi.org/10.1097/j.pain.0000000000001959 (2020).
Mallard, T. T., Grotzinger, A. D. & Smoller, J. W. Examining the shared etiology of psychopathology with genome-wide association studies. Physiol. Rev. 103, 1645–1665. https://doi.org/10.1152/physrev.00016.2022 (2023).
Weith, M. & Beyer, A. The next step in Mendelian randomization. Elife https://doi.org/10.7554/eLife.86416 (2023).
Liu, Y., Huang, Y., Liu, C. & Liu, Q. Longer leukocyte telomere length increases the risk of atrial fibrillation: A mendelian randomization study. Aging Dis 13, 1311–1313. https://doi.org/10.14336/ad.2022.02251 (2022).
Hartwig, F. P., Davies, N. M., Hemani, G. & Davey Smith, G. Two-sample Mendelian randomization: Avoiding the downsides of a powerful, widely applicable but potentially fallible technique. Int. J. Epidemiol. 45, 1717–1726. https://doi.org/10.1093/ije/dyx028 (2016).
Skrivankova, V. W. et al. Strengthening the reporting of observational studies in epidemiology using mendelian randomization: The STROBE-MR statement. JAMA 326, 1614–1621. https://doi.org/10.1001/jama.2021.18236 (2021).
Wijndaele, K., Sharp, S. J., Wareham, N. J. & Brage, S. Mortality risk reductions from substituting screen time by discretionary activities. Med. Sci. Sports Exerc. 49, 1111–1119. https://doi.org/10.1249/mss.0000000000001206 (2017).
Zhu, J. et al. Physical activity patterns, genetic susceptibility, and risk of hip/knee osteoarthritis: A prospective cohort study based on the UK Biobank. Osteoarthr. Cartil. 30, 1079–1090. https://doi.org/10.1016/j.joca.2022.04.004 (2022).
van de Vegte, Y. J., Said, M. A., Rienstra, M., van der Harst, P. & Verweij, N. Genome-wide association studies and Mendelian randomization analyses for leisure sedentary behaviours. Nat. Commun. 11, 1770. https://doi.org/10.1038/s41467-020-15553-w (2020).
Boer, C. G. et al. Deciphering osteoarthritis genetics across 826,690 individuals from 9 populations. Cell 184, 4784-4818.e4717. https://doi.org/10.1016/j.cell.2021.07.038 (2021).
Spiga, F. et al. Tools for assessing quality and risk of bias in Mendelian randomization studies: A systematic review. Int. J. Epidemiol. 52, 227–249. https://doi.org/10.1093/ije/dyac149 (2023).
Bowden, J., Davey Smith, G. & Burgess, S. Mendelian randomization with invalid instruments: Effect estimation and bias detection through Egger regression. Int. J. Epidemiol. 44, 512–525. https://doi.org/10.1093/ije/dyv080 (2015).
Bowden, J., Davey Smith, G., Haycock, P. C. & Burgess, S. Consistent estimation in mendelian randomization with some invalid instruments using a weighted median estimator. Genet. Epidemiol. 40, 304–314. https://doi.org/10.1002/gepi.21965 (2016).
Burgess, S., Bowden, J., Fall, T., Ingelsson, E. & Thompson, S. G. Sensitivity analyses for robust causal inference from mendelian randomization analyses with multiple genetic variants. Epidemiology 28, 30–42. https://doi.org/10.1097/ede.0000000000000559 (2017).
Verbanck, M., Chen, C. Y., Neale, B. & Do, R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat. Genet. 50, 693–698. https://doi.org/10.1038/s41588-018-0099-7 (2018).
Burgess, S. & Thompson, S. G. Multivariable Mendelian randomization: The use of pleiotropic genetic variants to estimate causal effects. Am. J. Epidemiol. 181, 251–260. https://doi.org/10.1093/aje/kwu283 (2015).
Hartley, A. et al. Using multivariable Mendelian randomization to estimate the causal effect of bone mineral density on osteoarthritis risk, independently of body mass index. Int J Epidemiol 51, 1254–1267. https://doi.org/10.1093/ije/dyab251 (2022).
Larsson, S. C. & Burgess, S. Appraising the causal role of smoking in multiple diseases: A systematic review and meta-analysis of Mendelian randomization studies. EBioMedicine 82, 104154. https://doi.org/10.1016/j.ebiom.2022.104154 (2022).
Gill, D., Karhunen, V., Malik, R., Dichgans, M. & Sofat, N. Cardiometabolic traits mediating the effect of education on osteoarthritis risk: A Mendelian randomization study. Osteoarthr. Cartil. 29, 365–371. https://doi.org/10.1016/j.joca.2020.12.015 (2021).
Chang, A. H. et al. Association of long-term strenuous physical activity and extensive sitting with incident radiographic knee osteoarthritis. JAMA Netw. Open 3, e204049. https://doi.org/10.1001/jamanetworkopen.2020.4049 (2020).
Gates, L. S. et al. Recreational physical activity and risk of incident knee osteoarthritis: An international meta-analysis of individual participant-level data. Arthritis Rheumatol. 74, 612–622. https://doi.org/10.1002/art.42001 (2022).
Bell, E. C. et al. Does land-based exercise-therapy improve physical activity in people with knee osteoarthritis? A systematic review with meta-analyses. Osteoarthr. Cartil. 30, 1420–1433. https://doi.org/10.1016/j.joca.2022.07.008 (2022).
Ouellet, P. et al. Region-specific exercises vs general exercises in the management of spinal and peripheral musculoskeletal disorders: A systematic review with meta-analyses of randomized controlled trials. Arch. Phys. Med. Rehabil. 102, 2201–2218. https://doi.org/10.1016/j.apmr.2021.01.093 (2021).
Master, H. et al. Daily walking and the risk of knee replacement over 5 years among adults with advanced knee osteoarthritis in the United States. Arch. Phys. Med. Rehabil. 102, 1888–1894. https://doi.org/10.1016/j.apmr.2021.05.014 (2021).
Master, H. et al. Joint association of moderate-to-vigorous intensity physical activity and sedentary behavior with incident functional limitation: Data from the osteoarthritis initiative. J. Rheumatol. 48, 1458–1464. https://doi.org/10.3899/jrheum.201250 (2021).
Foucher, K. C., Aydemir, B. & Huang, C. H. Walking energetics and fatigue are associated with physical activity in people with knee osteoarthritis. Clin. Biomech. (Bristol, Avon) 88, 105427. https://doi.org/10.1016/j.clinbiomech.2021.105427 (2021).
White, D. K., Jakiela, J., Bye, T., Aily, J. & Voinier, D. Stepping forward: A scoping review of physical activity in osteoarthritis. J. Rheumatol. https://doi.org/10.3899/jrheum.220728 (2022).
Holden, M. A. et al. Guidance for implementing best practice therapeutic exercise for patients with knee and hip osteoarthritis: What does the current evidence base tell Us?. Arthritis Care Res. (Hoboken) 73, 1746–1753. https://doi.org/10.1002/acr.24434 (2021).
Kang, S. H., Joo, J. H., Park, E. C. & Jang, S. I. Effect of sedentary time on the risk of orthopaedic problems in people aged 50 years and older. J. Nutr. Health Aging 24, 839–845. https://doi.org/10.1007/s12603-020-1391-7 (2020).
Huang, G. et al. A Mendelian randomization study on causal effects of leisure sedentary behaviour on the risk of rheumatoid arthritis. Eur. J. Clin. Invest. 53, e13894. https://doi.org/10.1111/eci.13894 (2023).
Chen, X. et al. Causal relationship between physical activity, leisure sedentary behaviors and COVID-19 risk: A Mendelian randomization study. J. Transl. Med. 20, 216. https://doi.org/10.1186/s12967-022-03407-6 (2022).
Benatti, F. B. & Ried-Larsen, M. The effects of breaking up prolonged sitting time: A review of experimental studies. Med. Sci. Sports Exerc. 47, 2053–2061. https://doi.org/10.1249/mss.0000000000000654 (2015).
Ni, J. et al. Does smoking protect against developing osteoarthritis? Evidence from a genetically informed perspective. Semin. Arthritis Rheum 55, 152013. https://doi.org/10.1016/j.semarthrit.2022.152013 (2022).
Matsuse, H., Segal, N. A., Rabe, K. G. & Shiba, N. Effect of neuromuscular electrical stimulation during walking on pain sensitivity in women with obesity with knee pain: A randomized controlled trial. Arch. Phys. Med. Rehabil. 103, 1707–1714. https://doi.org/10.1016/j.apmr.2022.01.157 (2022).
Acknowledgements
We appreciate the consortium studies for providing detailed association information for public consumption, and all study participants and researchers for their contributions and commitment to this study.
Funding
No specific funding was obtained from any public sector, commercial, or non-profit organization to carry out the work described here.
Author information
Authors and Affiliations
Contributions
Y.H.Z. was responsible for the conception and design of this study. X.Z.L. and S.B.W. had full access to all research data and were responsible for data integrity and accuracy of data analysis. H.W. and W.G.L. performed the statistical analysis and wrote the manuscript. All authors contributed to the writing of the article or critical review of important intellectual content, and all approved the final version for publication.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Li, X., Wang, S., Liu, W. et al. Causal effect of physical activity and sedentary behaviors on the risk of osteoarthritis: a univariate and multivariate Mendelian randomization study. Sci Rep 13, 19410 (2023). https://doi.org/10.1038/s41598-023-46984-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-46984-2
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
