
Volume 91 Issue 1, January 2022
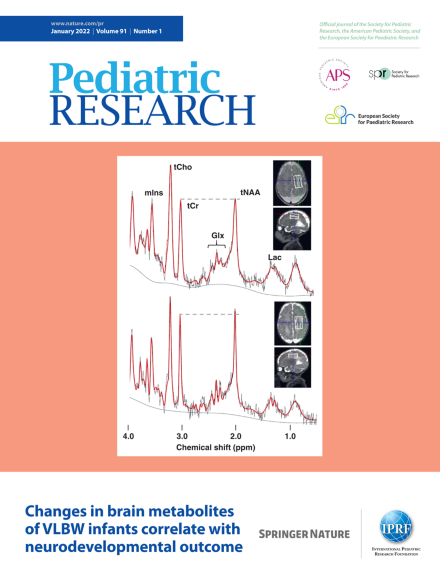
Magnetic resonance spectroscopy at term of very-low-birthweight infants with delayed (top) and normal (bottom) development. See article by Tomiyasu et al. on page 197.
Editor's Focus
-
Advertisement
