
Abstract
Cisplatin (CDDP) combined with radiotherapy (RT) is employed in head and neck squamous cell carcinoma (HNSCC) with variable toxicities and clinical response. Glutathione S-transferases (GSTs) participate in CDDP excretion from cells, and genes encoding GSTs, GSTM1, GSTT1and GSTP1, are polymorphic in humans. This prospective study aimed to evaluate the roles of GSTM1, GSTT1, and GSTP1 Ile105Val polymorphisms in outcomes of HNSCC patients treated with CDDP chemoradiation. Ninety patients were genotyped by multiplex PCR. Urinary CDDP measurements were performed by HPLC. Treatment side effects and response were analysed by conventional criteria. Patients with GSTT1 genes showed 7.23- and 5.37-fold higher likelihood of presenting vomiting and ototoxicity, lower glomerular filtration rate (GFR), and lower elimination of CDDP in urine relative to patients with deleted genes. Patients harbouring the GSTP1 IleVal or ValVal genotypes showed 4.28-fold higher likelihood of presenting grade 2 or 3 vomiting and lower GFR with treatment than those harbouring the IleIle genotype. In multivariate Cox analysis, patients with the GSTP1 105ValVal genotype had 3.87 more chance of presenting disease progression than those with the IleIle or IleVal genotype (p < 0.01). Our findings provide preliminary evidence that inherited abnormalities in CDDP metabolism, related to GSTT1 and GSTP1 Ile105Val polymorphisms, alter outcomes of HNSCC patients treated with CDDP and RT.
Similar content being viewed by others


Introduction
Head and neck squamous cell carcinoma (HNSCC) is a common cancer affecting humans and is responsible for around 600,000 cases and 350,000 tumour-related deaths worldwide each year1.
Cisplatin (CDDP) is one of the first-line drugs against HNSCC and is usually administered with radiotherapy (RT)2. CDDP treatment leads to adducts with cellular DNA and triggers the release of free radicals, which induces cell death by apoptotic pathways3. RT induces lesions in cellular DNA via activation of photons and free radical generation, consequently leading to apoptosis of damaged cells. Therefore, the effects of RT are potentiated by CDDP4. Although the beneficial effects of CDDP are unequivocal, it is associated with numerous side effects involving the hematologic, gastrointestinal, renal, and auditory systems in HNSCC5,6. HNSCC patients treated with CDDP may also experience resistance and/or tumour recurrence within five years of follow-up7.
HNSCC patients with similar clinicopathological aspects are expected to present variable toxicity, tumour regression, and survival following treatment with CDDP-based chemoradiation8. Variability in patient responses can be caused by differences in genetic regulation of metabolic pathways.
Glutathione S-transferases (GSTs) participate in the excretion of CDDP from the cells9, and the genes encoding GSTs, namely, Mu 1 (GSTM1), Theta 1 (GSTT1), and Pi 1 (GSTP1), are polymorphic in humans. Null genotypes of GSTM1 and GSTT1 result in absence of encoded enzymes10, and the GSTP1 Ile105Val polymorphism confers reduced enzymatic activity11. A few previous publications associated GSTM1, GSTT1, and/or GSTP1 Ile105Val polymorphisms with variable toxicities in HNSCC patients treated with CDDP and RT12,13,14. In a previous study, tumour response to CDDP chemoradiation was observed in a HNSCC patient with distinct genotypes of GSTT1 and GSTP1 Ile105Val polymorphisms12; however, another study indicated that the GSTM1, GSTT1, and GSTP1 genes did not alter response to CDDP9. Furthermore, the GSTM1, GSTT1, and/or GSTP1 Ile105Val polymorphisms were associated with variable survival in HNSCC patients treated with CDDP chemoradiation15 or RT16. However, these genes showed no association with survival in radiation-treated HNSCC patients17.
Considering the limited number of studies that investigated these genes, we conducted this prospective study to determine whether the GSTM1, GSTT1, and GSTP1 Ile105Val polymorphisms alter toxicity, response rate, and survival in HNSCC patients treated with CDDP and RT.
Results
Patients and laboratory characteristics
A total of 90 HNSCC patients with a median age of 56 years were enrolled in this study. The majority of the enrolled subjects were males, drinkers and smokers, and presented moderately differentiated and advanced tumours. Nearly two-thirds of the cases had tumours in the pharynx. All analysed cases tested negative for human papillomavirus (HPV) type 16. Most patients showed medium or high adherence to anti-emetics (Table 1).
All patients were homogenously treated with RT at a total dose of 75 Gy and 80–100 mg/m2 of CDDP as initial dose as previously described (100 mg/m2 of CDDP was administered to patients with Karnofsky Performance Scale (KPS) 80–100% and without comorbidities, and patients with KPS 60–70% without comorbidities or KPS higher than 70% with comorbidities received CDDP at dose of 80 mg/m2). As recommended by the institutional protocol, 13 patients who presented adverse side effects of grades 3 or 4 received CDDP at lower dose (50–75 mg/m2) in further administrations or had suspension of CDDP. A total of 68 patients (75.5%) received three infusions of CDDP, while 22 patients (24.5%) received only two CDDP infusions because of hematologic or renal toxicities.
CDDP was measured in the urine samples of 43 patients after three CDDP infusions, and cumulative CCDP was found to be higher in urine samples collected in the first 12 h than in samples collected between 12 to 24 h (p = 0.001) and between 24 to 48 h (p = 0.001) (Table 1) (Fig. 1A). Similar urinary CDDP levels were observed in urine samples collected between 0 to 12 h (76.91 ± 50.26, 81.97 ± 68.74, and 56.39 ± 40.10 µg CDDP/mg creatinine; p = 0.06), 12 to 24 h (8.34 ± 7.02, 9.90 ± 7.82, and 7.59 ± 3.38 µg CDDP/mg creatinine, p = 0.10), and 24 to 48 h (5.35 ± 4.11, 7.83 ± 8.85, and 6.96 ± 4.10 µg CDDP/mg creatinine; p = 0.10) after the first, second, and third CDDP infusions, respectively.

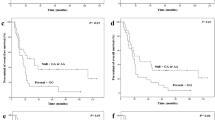
Urinary cisplatin (CDDP) and probability of event-free survival (EFS) of patients with head and neck squamous cell carcinoma treated with CDDP-chemoradiation. Average levels of CDDP after three CDDP infusion in 43 patients who collected urine in all three periods proposed in study, where *shows difference between CDDP excretion in 0–12 and 12–24 hours (p < 0.001), and **shows difference between CDDP excretion in 0–12 and 24–48 hours (p < 0.001) (A). Total CDDP urinary concentration in the same stratified by GSTM1, GSTT1 and GSTP1 Ile105Val genotypes, where *shows difference between patients with GSTT1 null genotype and patients with GSTT1 wild-type genotype (p = 0.04, power test: 83.4%) (B). Probabilities of EFS by Kaplan-Meier estimates in 90 patients stratified by genotypes of the GSTP1 Ile105 Val polymorphism (C).
Nearly four fifths and two thirds of available cases presented nausea and vomiting, respectively. The majority of patients showed hematologic toxicities; a quarter of the cases presented nephrotoxicity, and half of the patients showed ototoxicity (Table 2). Among the patients with available data on response rate (RR), 15 (20.5%) patients achieved complete response, 53 (72.6%) showed partial response (PR), and 5 (6.9%) showed stable disease (SD) status. Similar gastrointestinal and haematological toxicity (Table S1 Supplement), nephrotoxicity, ototoxicity, and response to therapy (Table S2 Supplement) were observed in patients stratified based on clinicopathological aspects and cumulative dose of intravenous CDDP.
All cases were followed-up for a median period of 21 months (range: 3.0–74). The cumulative probabilities of event-free survival (EFS) and overall survival (OS) at 24 months follow-up were 35.0% and 40.0%, respectively. On the date of analysis (December 2017), 23 patients were alive, of which 6 had HNSCC and 17 did not have HNSCC. A total of 67 patients died, of which 59 mortalities were associated with tumour effects and eight were attributed to unrelated causes.
Polymorphisms, toxicity, response, and CDDP excretion
The polymorphisms at the GSTP1 Ile105Val locus in the analyzed participants were in Hardy-Weinberg equilibrium (HWE) (χ2 = 2.80, p = 0.09).
Patients harbouring the GSTT1 genes were 7.23- and 5.37-fold more likely to present vomiting and ototoxicity of any grade (G1 to G3), respectively, relative to patients with the GSTT1 null genotype. Patients with the GSTP1 IleVal or ValVal genotype were 4.28-fold more likely to present vomiting (G2 or G3) than those carrying the IleIle genotype. Patients stratified based on nausea and nephrotoxicity symptoms showed similar frequencies of the GSTM1, GSTT1, and GSTP1 Ile105Val polymorphisms (Table 3). In addition, patients harbouring different genotypes of the analysed polymorphisms showed no significant differences in haematological toxicity and response to therapy (Table S3 Supplement).
Reduction in glomerular filtration rate (GFR) after chemoradiation was found to be more pronounced in patients harbouring the GSTT1 genes and in patients with GSTP1 IleVal or ValVal genotype relative to patients with the GSTT1 null genotype and IleIle genotype, respectively (Table 4). The mean cumulative urinary CDDP level (in the three cycles) was higher in patients with the GSTT1 null genotype than in those carrying the GSTT1 gene (429.58 ± 116.24 vs. 253.42 ± 95.20 g CDDP/mg creatinine, p = 0.04; power test = 83.4%) (Fig. 1B). A unique patient with combined GSTM1 null, GSTT1 null, and GSTP1 IleIle genotypes showed the highest reported total CDDP elimination rate (545.42 µg CDDP/mg creatinine).
Polymorphisms and survival analysis
At 24 months of follow-up, patients with advanced tumours (26.3% vs. 83.3%, p = 0.02) and patients with the GSTP1 ValVal genotype (0.0% vs. 31.7%, p = 0.047) had shorter event-free survival (EFS) than those with localised tumours and those harbouring the GSTP1 IleVal or ValVal genotype (Fig. 1C). Only patients with advanced tumours showed shorter OS (83.3% vs. 21.7%, p = 0.009) (Kaplan-Meier estimates). In univariate Cox analysis, patients with advanced tumours showed 7.50- and 8.88-fold higher likelihood of disease progression and mortality than those with localised tumours, respectively. Results of multivariate Cox analysis showed that patients with advanced tumours and patients harbouring the GSTP1 105ValVal genotype had 8.90- and 3.87-fold higher likelihood of presenting disease progression than those with localised tumours and harbouring the GSTP1 IleIle or Ile Val genotype, respectively. The significance of survival differences were confirmed by the bootstrapping method (Table 5).
Discussion
Our findings on the clinicopathological aspects of HNSSC patients, toxicity and RR to chemoradiation, and survival were similar to those described in previous studies18,19. A history of tobacco and alcohol consumption but the low prevalence of HPV infection indicate that history of tobacco and alcohol consumption were in fact the most important factors influencing tumour development in the analysed patients.
The presence of GSTT1 and the GSTP1 IleVal or ValVal genotype were found to be associated with a higher likelihood of presenting vomiting with chemoradiation, as previously suggested20. In a previous publication, we analysed almost the same patients enrolled in the current study (n = 88) and focused on the roles of GSTM1, GSTT1, GSTP1, and other genetic polymorphisms in genes involved in the repair of DNA damage induced by CDDP and apoptosis of cells with CDDP-induced lesions, only in severity of vomiting presented by HNSCC patients treated with CDDP chemoradiation14. Our previous findings indicated that the GSTP1 IleVal or ValVal genotype, but not the presence of GSTT1, was associated with vomiting; in the current study, vomiting was strongly associated with the presence of both GSTT1 and the GSTP1 IleVal or ValVal genotype. The contrasting results between the two studies can be attributed to the differences in patient stratification based on the severity of vomiting grade. In the previous publication, patients were stratified based on grade 0 or 1 vs. grade 2 or 3, whereas patients in the present study (n = 90) were stratified based on grade 0 vs. grades 1 to 3.
GSTT1 null patients were expected to show more severe vomiting than patients harbouring GSTT1; however, opposite results were obtained in the present study. Nutrient deficiency in patients with malignancies was postulated to lead to a lack of GSH, thereby causing impaired detoxification of free radicals of CDDP by GSTT1 and more severe toxicity13. In fact, reduction in body mass was found to be more predominantly observed in HNSCC patients receiving CDDP and RT treatment21, which could have modified the effects of the GSTT1 gene.
CDDP is well known to cause vomiting by inducing DNA damage in epithelial enterocromaffin cells of the intestine, thereby leading to serotonin release and stimulation of the chemoreceptor trigger zone and vomiting centre22. On the other hand, in addition to its role in CDDP detoxification, GSTP1 regulates JNK signalling pathways by forming a complex with c‐Jun‐JNK, which inactivates JNK signalling and inhibits apoptosis23. Thus, increased apoptosis of CDDP-damaged enterochromaffin cells of the intestines, which is associated with the less active “Val” allele of the GSTP1 Ile105Val polymorphism, may have influenced the severity of vomiting in the HNSCC patients.
In addition, the presence of GSTT1 was associated with ototoxicity in the patients. Oldenburg et al.24 demonstrated that the GSTM1 null genotype conferred protection against hearing impairment in testicular cancer patients treated with CDDP. Talach et al.13 reported that early treatment with CDDP induced ototoxicity in adults with various tumours types, including HNSCC, and two copies of the GSTT1 gene. The GSTP1 “Val” allele was associated with ototoxicity in patients with medulloblastoma who were treated with CDDP-based therapy25.
CDDP induces ototoxicity through the generation of free radicals and subsequently activates cell death pathways, such as the c-Jun N terminal kinase (JNK) and p38 mitogen activated protein kinase (MAPK) pathways, which in turn induce hair cell apoptosis and hearing loss26. GSTs represent the major enzyme family involved in the excretion of CDDP, which protects cells from the deleterious effects of free radicals9. Again, we expected more severe ototoxicity in GSTT1 null patients than in patients harbouring GSTT1; however, contrasting results were obtained in the present study. Talach et al.13 observed that patients with testicular tumours tended to have increased ototoxicity and presence of GSTT1. They postulated that nutrient deficiency with lack of GSH production and impaired detoxification of free radicals of CDDP in the sensory inner ear cells consequently increased ototoxicity. The same mechanisms are likely to occur in HNSCC patients in the present study.
Our current findings indicated that the GSTM1, GSTT1, and GSTP1 Ile105Val polymorphisms did not alter myelotoxicity and RR to CDDP and RT. Cabelguenne et al.9 found no associations of the GSTM1, GSTT1, and GSTP1 Ile105Val polymorphisms with RR in HNSCC patients treated with low doses of CDDP (25 mg/m²) and 5-FU. We observed pronounced myelotoxicity and a durable complete response in one HNSCC patient treated with both CDDP (100 mg/m²) and RT, which was attributed to inherited deficiency in CDDP detoxification (GSTT1 null genotype), deficiency in repair of CDDP cellular damage (MSH3 1045ThrThr), and increased apoptosis induction during CDDP cellular damage (GSTP1 105IleIle)12.
Patients harbouring the GSTT1 and GSTP1 IleVal or ValVal genotype showed more pronounced reduction in 51Cr-EDTA GFR after chemoradiation than those with the remaining genotypes. Khrunin et al.27 observed that patients with epithelial ovarian cancer and harbouring the GSTT1 null genotype who were treated with CDDP (100 mg/m2) plus cyclophosphamide were 3.31-fold more likely to develop nephrotoxicity.
Given its low molecular weight, CDDP is conjugated with reduced glutathione (GSH) in the liver. CDDP-GSH is freely filtered in the glomerulus and is completely recovered in the urine. CDDP-GSH reaches high concentrations in the proximal tubular cells of the internal renal cortex and the outer medullary layer. The mechanism of CDDP-induced tubular damage is complex and involves several mechanisms, such as CDDP accumulation-mediated membrane transport, conversion to nephrotoxin, DNA damage, mitochondrial dysfunction, oxidative stress, inflammatory response, activation of transducers and intracellular messengers, and activation of apoptotic pathways28.
To our knowledge, the roles of GSTT1 and GSTP1 in renal damage by CDDP remain unknown. Thus, the high CDDP-GSH concentrations in proximal tubule cells, associated with the GSTT1 genes, are likely to influence the severity of renal dysfunction in our patients. Furthermore, patients harbouring the GSTP1 IleVal or ValVal genotype showed more pronounced renal dysfunction. These results are unexpected because the protein encoded by the “Val” allele is known to be less efficient in CDDP-GSH production than that encoded by the “Ile” allele11. Again, this association could be attributed to effects of the protein encoded by the “Val” allele, which induces apoptosis in proximal tubule cells23.
Nearly 90% of CDDP excretion in our patients was measured within the first 24 h after infusion. Patients with the different GSTT1 genotypes showed variable CDDP levels, suggesting that gene polymorphisms influence the kinetics of CDDP elimination. Notably, pharmacokinetic studies usually analyse plasma samples obtained from patients receiving therapy. However, in the present study, sequential blood plasma collection cannot be obtained from outpatients. Therefore, we determined CDDP levels in urine for this pharmacokinetic analysis. The HPLC method used was well established29 and considered essential to pharmacokinetics and pharmacodynamics studies30. Lanjwani et al.29 postulated a correlation between urine and plasma CCDP levels and that both parameters could be used to pharmacokinetics studies of the drug. To the best of our knowledge, our study is the first to analyse the effects of GST polymorphisms on CDDP pharmacokinetics in HNSCC patients. Results of a unique study conducted by Joerger et al.31 showed no associations between GSTM1 and GSTP1 A313G (Ile105Val) genotypes with CDDP pharmacokinetics in advanced non-small-cell lung cancer patients.
Surprisingly, patients with the GSTT1 null genotype showed higher cumulative urinary CDDP levels compared to patients with the GSTT1 genotype. In this case, the deficiency in an individual GST isoenzyme could be compensated for by other isoforms32. Consistent with the above hypothesis, the only patient with GSTM1 null, GSTT1 null, and GSTP1 IleIle genotypes showed the highest total CDDP elimination rate.
Finally, our findings indicated that patients carrying the GSTP1 Ile105Val polymorphism had altered EFS. There were no associations between the GSTM1 and GSTT1 genotypes and survival in early-stage radiation-treated HNSCC patients17. In addition, disease-specific survival was observed in patients with SCC of oral cavity and harbouring GSTM1 who were treated with radiotherapy16. Shorter survival rates were observed in GSTM1 null patients with SCC of oral cavity who were treated with CDDP-based chemotherapy15. To the best of our knowledge, no published studies have focused on the role of the GSTP1 Ile105Val polymorphism in survival of HNSCC patients treated with CDDP and RT. The GSTP1 105IleIle genotype was previously associated with higher PFS in epithelial ovarian cancer patients treated with CDDP (100 mg/m²) and cyclophosphamide27 and oesophageal cancer patients treated with CDDP and 5-FU/paclitaxel33. The observed association between GSTP1 ValVal genotype and shorter EFS in the current study was based on a small sample size and cannot be explained by direct drug detoxification by GSTP1, which will lead to higher survival. Free radicals produced by CDDP that are not detoxified due to the lack of GSTP1 are likely to induce new mutations in residual tumour cells, thereby facilitating survival and proliferation of the tumour cells34.
In summary, our study is the first to provide preliminary evidence that inherited GSTT1 and GSTP1 Ile105Val polymorphisms can alter gastrointestinal status, nephrotoxicity, ototoxicity, pharmacokinetics, and survival in HNSCC patients treated with CDDP chemoradiation. In this context, GST genotypes can be used as instruments for assessing toxicity of CDDP-based therapies by selecting HNSCC patients for the use of specific anti-emetics and protective renal and auditory system agents, thereby saving patients from the side effects of chemotherapy14,35,36 and reducing treatment costs37. However, we are aware that the number of patients enrolled in study was not large, and that further larger studies and functional analyses of relevant polymorphisms are required to confirm the roles of these GSTs in disease.
Material and Methods
Subjects and clinical variables
In this prospective study, HNSCC patients diagnosed at the Clinical Oncology Service of the General Hospital of University of Campinas between June 2011 and February 2014 were selected to undergo CCDP chemoradiation as definitive treatment due to locoregional unresectable tumour, refusal of surgery related to expected functional, or anatomic sequels or an organ preservation protocol. The following exclusion criteria were considered: (1) refusal to participate in the study; (2) low KPS score; (3) renal dysfunction; (4) previous hearing dysfunction; and/or (5) other therapeutic protocol. The present study was conducted according to the Declaration of Helsinki and was approved by the Ethics Committees of the University of Campinas (n° 274/2011; CAAE: 0218.0.146.000-11). All patients provided written informed consent after they were informed about the study and any associated risks.
Data relating to age, gender, tobacco and alcohol consumption, hematologic and biochemistry exams, tumour location, histological grade, and stage were obtained using specific questionnaires or patient charts. Subjects were classified according to smoking38 and drinking habits39 as previously reported. Tumours were diagnosed based on standard criteria40 and staged based on criteria specified by the American Joint Committee on Cancer41. HPV type 16 was investigated in tumour fragments by immunohistochemistry and in situ hybridization as previously reported42.
Toxicities (nausea, vomiting, hematologic, nephrotoxicity, and ototoxicity) were assessed using data on adverse effects, hematologic exams, GFR measured with EDTA labelled with chrome37 (51Cr-EDTA GFR), and audiometric tests performed before and after chemoradiotherapy. Toxicities were evaluated according to the National Cancer Institute based on common terminology criteria for adverse events version 4.0 (CTCAE)43. For each patient, the worst grade for each toxicity was included in analysis.
Patients were homogeneously treated with CDDP chemoradiation according to the institutional protocol42. RR to treatment was assessed using the Response Evaluation Criteria in Solid Tumors (RECIST) guidelines version 1.144. Surgical tumour resection was indicated to patients with good clinical condition and partial response or tumour relapse.
On each day of CDDP infusion, patients received hydration (3 L of 0.9% saline solution), 125 mL of 20% mannitol as diuretic, 20 mL of 19.1% potassium chloride and 10 mL of magnesium sulphate as electrolytes, and 20 mg of dexamethasone plus 24 mg of ondansetron as prophylaxis to acute emesis. Patients were orally administered with 8 mg of dexamethasone (every 12 h) and 10 mg of metoclopramide (every 6 h) for three additional days42. Anti-emetic adherence was classified as previously described42.
Patient follow-up was performed in three-month intervals. The end of the follow-up period was September 2018.
DNA extraction and genotyping
Genomic DNA of all subjects was isolated from 5 mL of peripheral blood sample following the proteinase K and lithium chloride method45.
GSTM1 and GSTT1 genotypes were amplified from genomic DNA by the multiplex-polymerase chain reaction (multiplex-PCR)46. GSTP1 Ile105Val genotypes were identified by PCR and enzymatic digestion47. Positive and negative controls were used in all genotyping reactions. The amount of 15% of genotype determinations was carried out twice in independent experiments and showed 100% of concordance.
Urinary CCDP excretion kinetics
Urine was collected from patients by voluntary urination during three different collection periods: 0–12 h, 12–24 h, and 24–48 h after each CDDP infusion. Samples were stored at −80 °C until analysis48.
CDDP derivatization and extraction from patient urine and a sample of standard urine (without CDDP) were conducted as previously described49. Nickel chloride and chloroform were obtained from Merck, Darmstadt, Germany, and diethyldithiocarbamate was obtained from Sigma-Aldrich, India. Samples were analysed using a high-performance liquid chromatography (HPLC) Separation Module system with dual absorbance detector (UV-visible detector, wavelength 254 nm) (Waters 2487, Milford, MA, USA) and a Hypersil ODS C18 column (150 mm × 4 mm with a particle size of 4 μm (Thermo, Waltham, MA, USA). The HPLC conditions and the mobile phase were set as described by Lopez-Flores et al.50. Sample measurement and standard curves were performed in duplicate. Urinary CDDP was normalized with urinary creatinine and measured using akinetic kit (Creatinine Laborclin kit, Parana, Brazil). The final concentration of urinary CDDP was calculated as the sum of all measurements obtained after each CDDP administration.
Statistical analysis
The HWE was tested with chi-square (χ2) statistic for the goodness-to-fit. Differences between groups were analysed by χ2 or Fisher’s exact test. A logistic regression model was generated to obtain odds ratios (OR) values to verify associations between genotypes, nausea, vomiting, nephrotoxicity, ototoxicity, haematological toxicity, and RR. Comparisons between GFR before and after CCDP treatment were evaluated by two-way ANOVA. Student’s t-test was performed to determine associations between average CDDP urinary elimination rate in each collection period (0–12, 12–24, and 24–48 h) and to determine significant associations of the total CDDP elimination rates with genotypes. The statistical power of a test was calculated using the Researcher’s Toolkit51.
EFS and OS were calculated for each participant from the date of diagnosis until the date of tumour progression, tumour relapse, death attributed to tumour effects, or last follow-up and from the date of diagnosis until the date of death by any cause or last follow-up contact, respectively. Kaplan-Meier method was used to plot EFS and OS curves, and log-rank test was conducted to determine significant differences between curves. Multivariate Cox regression was used to estimate hazard ratios (HRs) adjusted for potential possible discrepancies in clinical aspects (p ≤ 0.10 in univariate Cox regression). Bootstrapping (n = 1,000) based on repeatedly random sampling was applied to ensure the stability of the model by applying the bias-corrected and accelerated method.
P-values were two-sided and considered statistically significant at p < 0.05. Statistical analyses were conducted using SPSS 21.0 software (IBM Corporation, Armonk, NY, USA).
Data Availability
The authors declare that all data of this study are available from the corresponding author upon reasonable request.
References
Siegel, R. L., Miller, K. D. & Jemal, A. Cancer statistics 2017. CA Cancer J. Clin. 67, 7–30 (2017).
Kimura, S., Imagawa, Y., Satake, K. & Tsukuda, M. The relationship of the human glutathione S-transferase P1 polymorphism and chemotherapeutic sensitivity in head and neck squamous carcinoma. Int. J. Mol. Med. 14, 185–189 (2004).
Dasari, S. & Tchounwou, P. B. Cisplatin in cancer therapy: molecular mechanisms of action. Eur. J. Pharmacol. 740, 364–378 (2014).
Lomax, M. E., Folkes, L. K. & O’Neill, P. Biological consequences of radiation-induced DNA damage: relevance to radiotherapy. Clin. Oncol. 25, 578–585 (2013).
Paken, J., Govender, C. D., Pillay, M. & Sewram, V. Cisplatin-associated ototoxicity: a review for the health professional. J. Toxicol. 2016, 1809394 (2016).
Visacri, M. B. et al. Adverse drug reactions and kinetics of cisplatin excretion in urine of patients undergoing cisplatin chemotherapy and radiotherapy for head and neck cancer: a prospective study. DARU 25, 1–9 (2017).
Jimenez, L., Jayakar, S. K., Ow, T. J. & Segall, J. E. Mechanisms of invasion in head and neck cancer. Arch. Pathol. Lab. Med. 139, 1334–1348 (2015).
Forastiere, A. A. et al. Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal cancer. N. Engl. J. Med. 349, 2091–2098 (2003).
Cabelguenne, A. et al. Glutathione-associated enzymes in head and neck squamous cell carcinoma and response to cisplatin-based neoadjuvant chemotherapy. Int. J. Cancer 93, 725–730 (2001).
McIlwain, C. C., Townsend, D. M. & Tew, K. D. Glutathione S-transferase polymorphisms: cancer incidence and therapy. Oncogene 25, 1639–1648 (2006).
Strange, R. C., Spiteri, M. A., Ramachandran, S. & Fryer, A. A. Glutathione-S-transferase family of enzymes. Mutat. Res. 482, 21–26 (2001).
Lopes-Aguiar, L. et al. Do genetic polymorphisms modulate response rate and toxicity of cisplatin associated with radiotherapy in laryngeal squamous cell carcinoma?: a case report. Medicine (Baltimore) 94, e578 (2015).
Talach, T. et al. Genetic risk factors of cisplatin induced ototoxicity in adult patients. Neoplasma 63, 263–268 (2016).
Carron, J. et al. GSTP1 c.313A > G, XPD c.934G > A, XPF c.2505T > C and CASP9 c.-1339A > G Polymorphisms and severity of vomiting in head and neck cancer patients treated with cisplatin chemoradiation. Basic Clin. Pharmacol. Toxicol. 121, 520–525 (2017).
Shukla, D. et al. Association between GSTM1 and CYP1A1 polymorphisms and survival in oral cancer patients. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech. Repub. 157, 304–310 (2013).
Mahimkar, M. B. et al. Polymorphisms in GSTM1 and XPD genes predict clinical outcome in advanced oral cancer patients treated with postoperative radiotherapy. Mol. Carcin. 51, E94–E103 (2015).
Azad, A. K. et al. Validation of genetic sequence variants as prognostic factors in early-stage head and neck squamous cell cancer survival. Clin. Cancer Res. 18, 196–206 (2012).
Adelstein, D. J. et al. An intergroup phase III comparison of standard radiation therapy and two schedules of concurrent chemoradiotherapy in patients with unresectable squamous cell head and neck cancer. J. Clin. Oncol. 21, 92–98 (2003).
De Castro, G. Jr. et al. High-dose cisplatin concurrent to conventionally delivered radiotherapy is associated with unacceptable toxicity in unresectable, non-metastatic stage IV head and neck squamous cell carcinoma. Eur. Arch. Otorhinolaryngol. 264, 1475–1482 (2007).
Sugino, S. & Janicki, P. K. Pharmacogenetics of chemotherapy-induced nausea and vomiting. Pharmacogenomics 16, 149–160 (2015).
Carvalho, T. M. R. et al. Evaluation of patients with head and neck cancer performing standard treatment in relation to body composition, resting metabolic rate, and inflammatory cytokines. Head Neck 37, 97–102 (2015).
Minami, M. et al. Pharmacological aspects of anticancer drug-induced emesis with emphasis on serotonin release and vagal nerve activity. Pharmacol. Ther. 99, 149–165 (2003).
Singh, S. Cytoprotective and regulatory functions of glutathione S-transferases in cancer cell proliferation and cell death. Cancer Chemother. Pharmacol. 75, 1–15 (2015).
Oldenburg, J. et al. Association between long-term neuro-toxicities in testicular cancer survivors and polymorphisms in glutathione-s-transferase-P1 and -M1, a retrospective cross sectional study. J. Transl. Med. 5, 1–8 (2007).
Rednam, S., Scheurer, M. E., Adesina, A., Lau, C. C. & Okcu, M. F. Glutathione S-transferase P1 single nucleotide polymorphism predicts permanent ototoxicity in children with meduloblastoma. Pediatr.Blood Cancer 60, 593–598 (2013).
Tabuchi, K. et al. Ototoxicity: mechanisms of cochlear impairment and its prevention. Curr. Med. Chem. 18, 4866–4871 (2011).
Khrunin, A. V., Moisseev, A., Gorbunova, V. & Limborska, S. Genetic polymorphisms and the efficacy and toxicity of cisplatin-based chemotherapy in ovarian cancer patients. Pharmacogenomics J. 10, 54–61 (2010).
Herrera-Pérez, Z., Gretz, N. & Dweep, H. A Comprehensive review on the genetic regulation of cisplatin-induced nephrotoxicity. Curr. Genomics 17, 279–293 (2016).
Lanjwani, S. N., Zhu, R., Khuhawar, M. Y. & Ding, Z. High performance liquid chromatographic determination of platinum in blood and urine samples of cancer patients after administration of cisplatin drug using solvent extraction and N,N′-bis(salicylidene)-1,2-propanediamine as complexation reagent. J. Pharm. Biomed. Anal. 40, 833–839 (2006).
Hanada, K., Nishijima, K., Ogata, H., Atagi, S. & Kawahara, M. Population pharmacokinetic analysis of cisplatin and its metabolites in cancer patients: possible misinterpretation of covariates for pharmacokinetic parameters calculated from the concentrations of unchanged cisplatin, ultrafiltered platinum and total platinum. Jap. J. Clin. Oncol. 1, 179–184 (2001).
Joerger, M. et al. Germline polymorphisms in patients with advanced nonsmall cell lung cancer receiving first-line platinum-gemcitabine chemotherapy: a prospective clinical study. Cancer 118, 2466–2475 (2012).
Parl, F. F. Glutathione S-transferase genotypes and cancer risk. Cancer Lett. 221, 123–9 (2005).
Lee, J. M. et al. Association of GSTP1 polymorphism and survival for esophageal cancer. Clin. Cancer Res. 11, 4749–4753 (2005).
Singh, A. K. et al. Free radicals hasten head and neck cancer risk: A study of total oxidant, total antioxidant, DNA damage, and histological grade. J. Postgrad. Med. 62, 96–101 (2016).
Bulacio, R. P., Anzai, N., Ouchi, M. & Torres, A. M. Organic anion transporter 5 (Oat5) urinary excretion is a specific biomarker of kidney injury: evaluation of urinary excretion of exosomal Oat5 after N-acetylcysteine prevention of cisplatin induced nephrotoxicity. Chem. Res. Toxicol. 28, 1595–1602 (2015).
Doğan, M. et al. Protective role of misoprostol against cisplatin-induced ototoxicity. Eur. Arch. Otorhinolaryngol. 273, 3685–3692 (2016).
Macedo, L. T. et al. Cost-minimization analysis of GSTP1 c.313A > G genotyping for the prevention of cisplatin-induced nausea and vomiting: a Bayesian inference approach. PLoS One 14, e0213929 (2019).
Jindal, S. K. et al. Bronchogenic carcinoma in Northern India. Thorax 37, 343–347 (1982).
Whitcomb, D. C. et al. Multicenter approach to recurrent acute and chronic pancreatitis in the United States: the North American Pancreatitis Study 2 (NAPS2). Pancreatology 8, 520–531 (2008).
Mori, S. et al. A novel evaluation system of metastatic potential of oral squamous cell carcinoma according to the histopathological and histochemical grading. Oral Oncol. 34, 549–557 (1998).
Edge, S. B. et al. American Joint Committee on Cancer: Cancer Staging Manual. 21–97 (Springer, 2010).
Lopes-Aguiar, L. et al. XPD c.934G > A polymorphism of nucleotide excision repair pathway in outcome of head and neck squamous cell carcinoma patients treated with cisplatin chemoradiation. Oncotarget 8, 16190–16201 (2017).
National Cancer Institute. Cancer therapy evolution program. Common terminology criteria for adverse events (CTCAE) v 4.0, 2009. Available at, http://ctep.cancer.gov. Accessed September (2017).
Eisenhauer, E. A. et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur. J. Cancer 45, 228–247 (2009).
Woodhead, J. L., Fallon, R., Figuered, H., Longdale, J. & Malcom, A. D. B. Alternative methodology of gene diagnosis. In: K. E. Davies (org). Human Genetic Diseases: A Practical Approach. 51–64 (IRL Press, 1986).
Arruda, V. R. et al. Prevalence of homozygosity for the deleted alleles of glutathione S-transferase mu (GSTM1) and theta (GSTT1) among distinct ethnic groups from Brazil: relevance to environmental carcinogenesis? Clin. Genet. 54, 210–214 (1998).
Hohaus, S. et al. Glutathione S-transferase P1 genotype and prognosis in Hodgkin’s lymphoma. Clin. Cancer Res. 11, 2175–2179 (2005).
Vouillamoz-Lorenz, S., Bauer, J., Lejeune, F. & Decosterd, L. A. Validation of an AAS method for the determination of platinum in biological fluids from patients receiving the oral platinum derivative JM216. J. Pharm. Biomed. Anal. 25, 465–475 (2001).
Bannister, S. J., Sternson, L. A. & Repta, A. J. Urine analysis of platinum species derived from cis-dichlorodiammineplatinum(II) by high-performance liquid chromatography following derivatization with sodium diethyldithiocarbamate. J. Chromatogr. 173, 333–342 (1979).
Lopez-Flores, A., Jurado, R. & Garcia-Lopez, P. A high-performance liquid chromatographic assay for determination of cisplatin in plasma, cancer, cell and tumour samples. J. Pharmacol. Toxicol. Methods 52, 366–372 (2005).
Park, H. M. Hypothesis testing and statistical power of a test. Working Paper. The University Information Technology Services (UITS), Indiana University. In, http://www.indiana.edu/~statmath/stat/all/power/index.html. Acessed in (17/04/2015).
Acknowledgements
We thank Miss Cleide Aparecida Moreira Silva and Miss Juliana Luz Passos Argenton from the Faculty of Medical Sciences for the statistical analysis guidance. This work was supported by “Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP) (grant number 2012/1807-2).
Author information
Authors and Affiliations
Contributions
E.C.P. was responsible for the study design, acquisition, analysis, and interpretation of data, and drafting of the manuscript. E.F.D.C., L.L.A., G.A.S.N., T.R.P.L., M.B.V. and G.J.L. made relevant contributions to the conception of work, genotyping, and data interpretation. M.B.V., A.P.L.C. and P.M. made relevant contributions to conception of the work, performed identification and control of side effects and conducted the urinary C.D.D.P. measurements. L.C. performed and analysed audiometric tests. C.T.C. provided surgical support to the patients. F.V.M., A.M.A.M.A. and C.C.C. analysed histological grade and human papillomavirus type 16 status. J.M.C.A. analysed computed tomography images of the necks of patients. C.D.R. analysed glomerular filtration rate measured by 51Cr-EDTA. C.S.P.L. was responsible for the concept and study design, clinical treatment of patients, acquisition, and interpretation of data, and critical revision of the manuscript. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pincinato, E.C., Costa, E.F.D., Lopes-Aguiar, L. et al. GSTM1, GSTT1 and GSTP1 Ile105Val polymorphisms in outcomes of head and neck squamous cell carcinoma patients treated with cisplatin chemoradiation. Sci Rep 9, 9312 (2019). https://doi.org/10.1038/s41598-019-45808-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-45808-6
This article is cited by
-
Genetic variability in cisplatin metabolic pathways and outcome of locally advanced head and neck squamous cell carcinoma patients
Scientific Reports (2023)
-
GSTM1 null and GSTT1 null: predictors of cisplatin-caused acute ototoxicity measured by DPOAEs
Journal of Molecular Medicine (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
