
Abstract
Glucose-6-phosphate dehydrogenase (G6PD) deficiency is an X-linked enzymopathy that affects hundreds of millions of people worldwide, conferring increased risk of neonatal jaundice and oxidant-induced hemolytic anemia. Screening and diagnosis of G6PD deficiency is currently performed using genetic or biochemical assays, the former being cost ineffective in populations with significant allelic heterogeneity and the latter being limited in ability to detect female heterozygotes. Cytochemical assays can obviate these shortcomings, but at the expense of added technical complexity and labor. We describe here a simple, novel cytofluorometric method that extends the classic methemoglobin reduction test, assessing G6PD deficiency at the level of an individual erythrocyte. In preliminary testing in Malian children, there was strong concordance between our method and established genetic and biochemical techniques. The assay is robust and economical and could serve as a screening method as well as a research tool, especially for high-throughput applications such as flow cytometry.
Similar content being viewed by others


Introduction
Glucose-6-phosphate dehydrogenase (G6PD) is a housekeeping enzyme that catalyses the rate-limiting first step in the pentose phosphate pathway, where it produces nicotinamide adenine dinucleotide phosphate (NADPH), a critical cofactor in a variety of metabolic processes. In the red blood cell (RBC), G6PD activity is especially important as the principal source of reducing power to regenerate the antioxidant glutathione. Individuals with G6PD-deficient RBCs are thus at risk for hemolysis precipitated by oxidants found in certain foods or chemotherapeutics, or generated during severe infections. One especially important example of drug-induced hemolysis is that caused by primaquine1,2,3, one of few antimalarial drugs active against both Plasmodium vivax hypnozoites and P. falciparum gametocytes. As areas of high malaria transmission overlap geographically with areas of high G6PD deficiency prevalence, this drug sensitivity reaction is an important public health concern, especially given recent interest in reducing and eliminating malaria transmission4,5.
Despite decades of research, our understanding of the molecular pathogenesis of G6PD deficiency in the RBC is incomplete. While many functional allelic variants of G6PD have been described, it is less well understood how this genetic heterogeneity translates into diversity at the level of molecular and clinical phenotypes. Since clinical phenotypes such as primaquine sensitivity and malaria protection are complex and multifactorial in etiology, it is critical that the more proximate link between genetics and molecular phenotypes be clearly elucidated. This objective will require the development of novel methodologies suitable for high-throughput work.
One fundamental molecular phenotype to consider is G6PD enzyme activity, not only at the level of a single RBC but also in a population of RBCs. While many severe, sporadic G6PD variants are defective in their ability to form active dimers and tetramers, the means by which the most common variants, such as the main African variant ‘G6PD A-’, are deficient in enzyme activity are poorly understood. As the catalytic rate of these variants is minimal, it is believed that the G6PD deficiency phenotypes they produce may result from decreased thermal stability of the protein6,7. According to this theory, nascent RBCs emerge from the bone marrow invested with near-normal G6PD activity in deficient individuals and the RBC aging process leads to a rapid decrease in the enzyme activity levels over time8. As many factors influence RBC senescence, it is also important to think of G6PD enzyme deficiency as a population characteristic, dependent on the age distribution of RBCs, where a significant proportion of reticulocytes can impact the measurement of G6PD enzyme activity in hemolysates.
In females that are heterozygous for G6PD deficiency polymorphisms, the picture of cell population variation is even more complicated due to the random X-chromosome inactivation that produces a mosaic population of G6PD-normal and G6PD-deficient RBCs. Selection processes during or shortly after hematopoiesis, or skewed patterns of X-chromosome inactivation9, which itself may be influenced by age10, each have the potential to significantly alter the G6PD deficiency status in a female heterozygote.
Various methods have been developed for assessing an individual's G6PD activity status and these can be loosely grouped into genetic, gross biochemical and cytochemical approaches.
Genetic typing of G6PD variants has a long history that began shortly after the development of gel electrophoresis, with variant G6PD enzymes first identified on the basis of differential migration rate on starch gels11. Today, this has been largely superseded by DNA-based genotyping and sequencing, which enable the identification of hundreds of nonsynonymous coding mutations associated with G6PD deficiency worldwide12, including many region-specific common variants.
Gross biochemical typing of G6PD involves either direct or indirect measures of enzyme activity in hemolysates. Direct tests are those that assess the enzyme's production of NADPH, which absorbs (340 nm) and fluoresces (450 nm) at characteristic wavelengths of light. These include the quantitative gross activity assay13, where the initial reaction velocity of the G6PD reaction is measured by examining the rate at which NADPH is produced. A qualitative analogue is the fluorescent spot test14, a popular screening test in which a drop of blood incubated with G6PD reaction substrates is placed on filter paper and illuminated with UV light, where the presence or absence of fluorescence provides a categorical measure of G6PD activity. Indirect assays of G6PD activity translate NADPH production into a colorimetric readout using chromophores like brilliant cresyl blue15, resazurin16, or formazan derivatives17,18; these assays typically involve long incubation periods of several hours (it is likely that they all rely on one or more oxidoreductases with poor kinetic profiles). One indirect test with shorter incubation times and more consistent results is the methemoglobin reduction test (MRT), once a widely used screening tool in resource-poor areas19,20. In this colorimetric assay, G6PD activity is assessed by first treating RBCs with nitrite (converting oxyhemoglobin [red] to methemoglobin [brown]) and then examining the rate of NADPH-dependent methemoglobin reduction in the presence of an appropriate redox catalyst (Nile blue or methylene blue) and substrate (glucose).
Cytochemical typing provides a categorical assessment of G6PD enzyme activity (i.e., ‘normal’ or ‘deficient’) at the level of an individual RBC and thus is the biochemical technique with greatest sensitivity for detecting mosaicism in female heterozygotes21. The methemoglobin elution test22, the earliest assay developed, is a light microscopic technique that extends the aforementioned MRT by submerging cyanide-treated thin blood smears in an ethanol-based solution of peroxide and citric acid prior to conventional staining, with individual RBCs labeled according to their relative methemoglobin content. Another more recently developed assay detects the quenching of glutaraldehyde-induced autofluorescence by formazan crystals produced in cells with normal G6PD activity23. Owing to their relative difficulty, technical complexity and often ambiguous results20, neither technique is particularly well suited to high-throughput applications.
Neither genetic nor gross biochemical approaches capture the full picture of G6PD activity. While genetic typing offers generally unequivocal interpretation of results, it is imperfectly predictive of both molecular and clinical phenotypes. In addition, typing multiple polymorphisms may not be cost-effective in resource-poor areas of allelic heterogeneity such as West Africa, Southeast Asia, or Oceania. Conversely, while gross biochemical approaches offer a functional assessment of G6PD deficiency, they are often difficult to interpret, especially for mosaic female heterozygotes and insufficiently scalable. Cytochemical methods can thus fill a void and, beyond their utility as a screening technique, can serve as a research tool to understand how genetic polymorphisms manifest at the level of G6PD activity in individual RBCs.
A straightforward cytochemical typing assay is presented here, termed the ‘cytofluorometric method’, which provides a fluorometric readout of the classic MRT at the level of an individual RBC. Upon testing this method on a cohort of Malian children, it was found to exhibit strong agreement with established methods of genetic and gross biochemical typing. This assay represents a useful addition to the screening and research toolkit for G6PD deficiency, especially in malaria-endemic areas.
Results
Development of the cytofluorometric method
The cytofluorometric method described here can be considered most simply as a fluorometric readout of a classic test for G6PD deficiency, the methemoglobin reduction test (MRT), at the level of an individual RBC (Figure 1). The MRT is a standard colorimetric test for G6PD deficiency19,20. In the first step, RBCs were treated with nitrite to oxidize all oxyhemoglobin (oxy-Hb, Fe2+) to methemoglobin (met-Hb, Fe3+). After washing away excess nitrite, glucose (substrate) and Nile blue sulfate (redox catalyst) were added, driving reduction of met-Hb back to oxy-Hb via an NADPH-dependent methemoglobin reductase (NADPH-hemoprotein reductase). The activity of this enzyme is dependent on NADPH, which is produced in the RBC solely by G6PD. The rate of the reductase reaction generally proceeds slowly, but is enhanced by Nile blue, which acts as an intermediate electron carrier between NADPH and the reductase. Thus, it is an indirect assay for G6PD deficiency, as normal RBCs (G6PD+) are able to quickly reduce met-Hb, while deficient RBCs (G6PD-) are not. At the end of the incubation period, G6PD+ samples (containing oxy-Hb) are red, G6PD- samples (containing met-Hb) are brown, with heterozygous (G6PD+/−) samples exhibiting an intermediate color. The MRT is sensitive to detection of both mild (class III, e.g., ‘G6PD A-’) and more severe (class II, e.g., ‘G6PD Mediterranean’) forms of G6PD deficiency24,25, presumably because of a threshold effect where a given level of G6PD activity is necessary for methemoglobin reduction to proceed at a visually observable rate within the reaction time allotted.

Principle of the cytofluorometric method.
The cytofluorometric method is a fluorometric extension of the methemoglobin reduction test (left). Fluorescence intensity distributions (FL1, right) show that the sequential reaction of cyanide followed by peroxide in RBCs containing predominantly oxyhemoglobin yields a fluorescent product (grey), while in nitrite-treated RBCs containing predominantly methemoglobin, little or no fluorescence is generated (white).
The cytofluorometric method follows on from the MRT by sequential reaction of cyanide followed by peroxide to generate a fluorescent product inside RBCs containing oxy-Hb, but little or no fluorescence from those containing met-Hb. In the first step, only met-Hb reacts with cyanide to generate cyanmethemoglobin (cyanmet-Hb), while oxy-Hb remains unreactive26. In the second step, only oxy-Hb reacts with peroxide27,28 to generate a fluorescent product (ferryl-Hb), while cyanmet-Hb remains largely nonreactive and nonfluorescent (Figure 1). After these two reactions, G6PD+ cells contain brightly fluorescent ferryl-Hb, while G6PD- cells contain very dimly fluorescent cyanmet-Hb (Figure 2), with fluorescent signal uniformly distributed throughout cells (Figure 3). One cannot say with absolute certainty what the fluorescent adduct(s) generated from these reactions are, but the major component is likely derived from conversion of ferrous heme to fluorescent iron-free porphyrin29,30,31,32, with an additional contribution from lipid peroxidation products such as malonyldialdehyde33,34.

Demonstration of the cytofluorometric method on artificial mixtures of A+ and A− RBCs.
Fluorescence intensity distributions (FL1) from artificial mixtures of A+ and A− RBCs containing either: (a) 0%, (b) 50%, (c) 75%, or (d) 100% A+ cells. Genotype is defined as follows: ‘A+’ = 202C (wild-type), ‘A−’ = 202T (deficient).

Demonstration of the cytofluorometric method on RBCs from A+, A+/− and A− individuals.
Shown here are representative fluorescence intensity distributions (FL1) and fluorescence micrographs from A+ (top), A+/− (middle) and A− (bottom) individuals. Genotype is defined as follows: ‘A+’ = 202C (wild-type), ‘A+/−’ = 202CT (heterozygous), ‘A−’ = 202T (deficient). The estimated proportion of high (blue) and low (red) intensity cells for each individual is indicated. NB: The micrographs show two populations of RBCs, one that is bright (G6PD+) and another that is dim (G6PD-).
Correlation of cytofluorometric data with genotype and gross activity data
The cytofluorometric method was applied to peripheral blood samples obtained from 42 healthy Malian children who were enrolled into a longitudinal cohort study. In addition, gross measures of G6PD enzyme activity were obtained using hemolysates derived from the same samples, as was genotype data for the G6PD 202 (‘A-’, rs1050828, C>T, Val68Met) variant, the most common G6PD deficiency polymorphism in Africa35. These latter two ‘gold-standard’ techniques provide a benchmark against which to evaluate the cytofluorometric method.
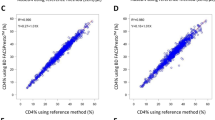
As expected, there was a strong relationship between data obtained using the two established techniques, the genetic and gross biochemical activity assays, with variation in genotype explaining 78% of variation in gross activity (Figure 4A, P = 5.5×10−14, 1-way ANOVA). Interestingly, the correlation between genotype and cytofluorometry data was even stronger, with genotype explaining 89% of variance in the proportion of G6PD+ cells found by cytofluorometry (Figure 4B, P = 1.0×10−21, 1-way ANOVA). Finally, it was found that the proportion of G6PD+ cells observed by cytofluorometry was well modeled by gross activity (Figure 4C, Spearman's rho = +0.88, P < 2.2×10−16) with the relationship remaining significant when considering only heterozygotes, in whom variance in both measures is greatest (Spearman's rho = +0.65, P = 0.01).

Correlations between genotype, gross activity and cytofluorometric data.
Concordance between (a) genotype and gross activity, (b) genotype and cytofluorometry and (c) gross activity and cytofluorometry. Genotype is defined as follows: ‘A+’ = 202C (wild-type), ‘A+/−’ = 202CT (heterozygous), ‘A−’ = 202T (deficient). Each point represents the mean of duplicate experiments, with gender indicated by blue (male) and magenta (female) dots. Horizontal line indicates median. G6PD activity units are arbitrary.
A few outliers were observed in the data, including two individuals who had homozygous A+ genotypes at G6PD 202 but exhibited mosaicism by cytofluorometry (Figure 4B), which may be the result of other, untyped G6PD deficiency mutations that are present at lower frequency in West Africa (e.g., G6PD 542, 680, or 968). The lone heterozygous outlier (Figure 4B) illustrates the difficulty of detecting certain mosaic females who seem to have normal enzyme activity, a well-documented limitation of the MRT22. Interestingly, A- males still exhibited a significant population of G6PD+ RBCs, which likely reflects the younger population of RBCs (likely reticulocytes) in which G6PD enzyme activity has not yet declined significantly.
Discussion
The cytofluorometric method described here is a new approach for typing G6PD deficiency at the level of individual RBCs. It provides a fluorescent readout of an established screening method (i.e., the methemoglobin reduction test, MRT) for G6PD deficiency, utilizing the unique redox chemistry and abundance of hemoglobin in the RBC to generate a differential auto-fluorescent signal that adequately distinguishes G6PD-normal from G6PD-deficient RBCs. In preliminary testing in Malian children, this assay showed strong agreement with other established methods of typing G6PD deficiency, including genotyping and gross biochemical activity. Additionally, it has performance characteristics that make it useful for clinicians and researchers alike, especially in resource-poor settings.
The literature suggests different possibilities for the origin of the fluorescent signal created when hydrogen peroxide reacts with oxyhemoglobin. Since this peroxide reaction does not occur with cyanmethemoglobin, it seems likely that the major fluorescent adduct created is a protoporphyrin derivative29,30,31,32 generated from ferryl heme (Fe4+) created as a result of the reaction of peroxide with ferrous heme (Fe2+). Another possible component of the fluorescent signal may derive from lipid peroxidation33,34, involving fatty acid derivatives such as malonyldialdehyde (MDA). Since MDA generation has been shown to be precipitated by unstable hemoglobins, it is possible that there is a complicated and co-dependent relationship between porphyrin generation and any downstream adducts such as those from lipid peroxidation32,36.
Several questions emerging from this work concern the methemoglobin reduction test, upon which the cytofluorometric method is dependent. One issue involves the potential for heritable variation in the activity of the NADPH-dependent methemoglobin reductase enzyme itself to confound assay results. Another known complication in interpreting the results of the MRT concerns cell-cell interaction20,22, specifically the finding that soluble factors can traffic from G6PD+ to G6PD- cells, possibly confounding results in mosaic females, such as the one A+/− outlier in our data who appeared as a G6PD-normal homozygote by cytofluorometry.
Overall, in spite of the aforementioned concerns, assay performance was found to be robust and reliable, giving consistent results across repeated measurements. Although the focus here was on a high-throughput application of the method using flow cytometry, the technique may be adaptable to additional applications. One direct use for investigators interested in methemoglobinemia would be to detect methemoglobin in an individual RBC by simply using the assay independently of the G6PD activity-dependent MRT step. As a screening tool for G6PD deficiency, one need only have a microscope outfitted with a UV lamp to detect G6PD+ and G6PD- cells in a blood sample, with no special fixation or staining procedures required and at a low cost per assay. This may be especially well-suited to areas such as Southeast Asia and Oceania where there is considerable allelic heterogeneity35 that makes genotyping cost ineffective. Finally, if the ultimate goal is to understand how genetic variation at G6PD influences an individual's complex, multifactorial response to primaquine administration or to Plasmodium infection, methods like that described here will be critical in further elucidating the proximate relationship between genotype and molecular phenotypes.
Methods
Samples
Peripheral blood samples from 42 children aged 1–15 years (mean = 5.8 years) were collected at a rural health center in Kenieroba, Mali. Of these children, 22 were male and 20 were female and most (79%) children were of Malinke ethnicity. Sample collection was nonrandom, as children were previously genotyped at G6PD 202. Blood was obtained by venipuncture, anticoagulated using acid-citrate-dextrose, washed three times in RPMI 1640 prior to storage at 4°C and processed within 4 days. All samples were obtained with parental informed consent and under protocols approved by the Ethics Committee of the Faculty of Medicine, Pharmacy and Odontostomatology at the University of Bamako and the Institutional Review Board of the National Institute of Allergy and Infectious Diseases.
Genotyping
Genotyping of the G6PD 202 polymorphism was performed by restriction fragment length polymorphism (RFLP) analysis using a nested PCR protocol, as described previously37.
Gross G6PD activity assay
Gross G6PD activity was measured in duplicate with the G6PDH kit (PD-410, Randox Laboratories, Kearneysville, WV), using a modified protocol adapted for high-throughput screening. First, a hemolysate was prepared by combining 10 µl of RBC suspension (50% hematocrit) with 20 µl of digitonin. Next, 2 µl of this hemolysate was combined with 4 µl NADP (0.34 mM), 2 µl glucose-6-phosphate (0.58 mM) and 120 µl reaction buffer (triethanolamine 31.7 mM, EDTA 3.2 mM, pH 7.6). Reaction rate was assessed using a UV/VIS plate spectrophotometer by observing the rate of production of NAPDH, which absorbs light at 340 nm, over a 30 min time course. Reaction rate was normalized to total protein content by measuring absorbance of hemoglobin at 540 nm, as follows:

Methemoglobin reduction test
The methemoglobin reduction test was performed in duplicate by modification of previously published protocols19,20. One hundred µl of RBC suspension (5% hematocrit) was combined with 100 µl of sodium nitrite (0.125 M, Sigma) and incubated at room temperature for 20 min. Samples were then washed three times with phosphate-buffered saline (PBS), with centrifugation at 1800 rpm for 1 min and resuspended to 100 µl with PBS. Finally, the washed, nitrite-treated RBCs were combined with 18 µl of glucose (0.28 M in PBS, Sigma) and 6 µl of Nile blue sulfate (0.01%, Sigma) and incubated at 37°C for 90 min in an aerobic environment (i.e., in open microcentrifuge tubes).
Cytofluorometric method
At the completion of the methemoglobin reduction test, 2.5 µl of potassium cyanide (0.4 M, Sigma) was added to each sample and incubated at room temperature for 5 min. Five µl of each sample was then added to 100 µl of hydrogen peroxide (3% in PBS, Sigma), agitated vigorously by hand and then washed two times in PBS, with centrifugation at 3000 rpm for 3 min.
Flow cytometry
Samples were analysed in duplicate using an Accuri C6 flow cytometer, using default factory settings, with 10,000 total events meeting size threshold of FSC-H > 80,000 collected. Samples were excited using an Ar ion laser (488 nm) and fluorescence emission was measured in the FL1 channel (533 ± 30 nm).
Fluorescence microscopy
Wet mounts of RBC samples were prepared and imaged on an Olympus BX53 fluorescence microscope using the 40x oil immersion objective, a 100 W Hg arc lamp and a FITC filter cube. All images were taken using a 10-second exposure time and processed identically using ImageJ (NIH, Bethesda, MD).
Data analysis
Custom scripts (available upon request) were written in R to automate data analysis. Gross activity was calculated using the formula above, with coefficients derived from linear modeling functions. Flow cytometry data were first converted from FCS format to raw data using the ‘flowCore’ package38 and then subject to morphological gating, with events retained only if they lay in the central 95% of the empirical distribution for both forward scatter (FSC) and side scatter (SSC) parameters. Next, the FL1 fluorescence intensity distribution was analysed to identify and quantify high and low intensity subpopulations. First, maxima in the kernel density estimation function were identified and then the midpoint between the two maxima was used as an ad hoc gate between high and low intensity subpopulations (Figure 1, right panel). When only one maximum was found (i.e., for G6PD-deficient homozygotes), the ad hoc gate was placed 0.5 log units away (about half the average distance between high and low intensity subpopulations in our dataset).
References
Dern, R. J., Beutler, E. & Alving, A. The hemolytic effect of primaquine. II. The natural course of the hemolytic anemia and the mechanism of its self-limited character. J Lab Clin Med 44, 171–176 (1954).
Carson, P. E., Flanagan, C., Ickes, C. & Alving, A. Enzymatic deficiency in primaquine-sensitive erythrocytes. Science 124, 484–485 (1956).
Shekalaghe, S. A. et al. In Tanzania, hemolysis after a single dose of primaquine coadministered with an artemisinin is not restricted to glucose-6-phosphate dehydrogenase-deficient (G6PD A-) individuals. Antimicrob Agents Chemother 54, 1762–1768 (2010).
Greenwood, B. Can malaria be eliminated? .Trans R Soc Trop Med Hyg 103 Suppl 1, S2–5 (2009).
White, N. J. The role of anti-malarial drugs in eliminating malaria. Malar J 7 Suppl 1, S8 (2008).
Yoshida, A., Stamatoyannopoulos, G. & Motulsky, A. G. Negro variant of glucose-6-phosphate dehydrogenase deficiency (A-) in man. Science 155, 97–99 (1967).
Babalola, O., Cancedda, R. & Luzzatto, L. Genetic variants of glucose 6-phosphate dehydrogenase from human erythrocytes: unique properties of the A - variant isolated from “deficient” cells. Proc Natl Acad Sci USA 69, 946–950 (1972).
Piomelli, S., Corash, L. M., Davenport, D. D., Miraglia, J. & Amorosi, E. L. In vivo lability of glucose-6-phosphate dehydrogenase in GdA- and GdMediterranean deficiency. J Clin Invest 47, 940–948 (1968).
Plenge, R. M. et al. A promoter mutation in the XIST gene in two unrelated families with skewed X-chromosome inactivation. Nat Genet 17, 353–356 (1997).
Au, W.-Y. et al. Glucose-6-phosphate dehydrogenase deficiency in female octogenarians, nanogenarians and centenarians. J Gerontol A Biol Sci Med Sci 61, 1086–1089 (2006).
Boyer, S., Porter, I. & Weilbacher, R. Electrophoretic heterogeneity of glucose-6-phosphate dehydrogenase and its relationship to enzyme deficiency in man. Proc Natl Acad Sci USA 48, 1868–1876 (1962).
Beutler, E. & Vulliamy, T. J. Hematologically important mutations: glucose-6-phosphate dehydrogenase. Blood Cells Mol Dis 28, 93–103 (2002).
Glock, G. & McLean, P. Glucose-6-phosphate dehydrogenase activity of rat liver. Nature 170, 119–120 (1952).
Beutler, E. A series of new screening procedures for pyruvate kinase deficiency, glucose-6-phosphate dehydrogenase deficiency and glutathione reductase deficiency. Blood 28, 553–562 (1966).
Dickens, F. & Glock, G. Direct oxidation of glucose-6-phosphate, 6-phosphogluconate and pentose-5-phosphates by enzymes of animal origin. Biochem J 50, 81–95 (1951).
Guilbault, G. G. Fluorometric determination of dehydrogenase activity using resorufin. Meth Enzymol 41, 53–56 (1975).
Hess, R., Scarpelli, D. & Pearse, A. Cytochemical localization of pyridine nucleotide-linked dehydrogenases. Nature 181, 1531–1532 (1958).
Jalloh, A. et al. Rapid epidemiologic assessment of glucose-6-phosphate dehydrogenase deficiency in malaria-endemic areas in Southeast Asia using a novel diagnostic kit. Trop Med Int Health 9, 615–623 (2004).
Brewer, G. J., Tarlov, A. & Alving, A. Methaemoglobin reduction test: a new, simple, in vitro test for identifying primaquine-sensitivity. Bull World Health Organ 22, 633–640 (1960).
Beutler, E. & Baluda, M. C. Methemoglobin reduction: Studies of the interaction between cell populations and of the role of methylene blue. Blood 22, 323–333 (1963).
Beutler, E., Yeh, M. & Fairbanks, V. The normal human female as a mosaic of X-chromosome activity: studies using the gene for C-6-PD-deficiency as a marker. Proc Natl Acad Sci USA 48, 9–16 (1962).
Gall, J. C., Brewer, G. J. & Dern, R. J. Studies of Glucose-6-Phosphate Dehydrogenase Activity of Individual Erythrocytes: The Methemoglobin-Elution Test for Identification of Females Heterozygous for G6PD Deficiency. Am J Hum Genet 17, 359–368 (1965).
van Noorden, C. J., Dolbeare, F. & Aten, J. Flow cytofluorometric analysis of enzyme reactions based on quenching of fluorescence by the final reaction product: detection of glucose-6-phosphate dehydrogenase deficiency in human erythrocytes. J Histochem Cytochem 37, 1313–1318 (1989).
Luzzatto, L., Usanga, F. A. & Reddy, S. Glucose-6-phosphate dehydrogenase deficient red cells: resistance to infection by malarial parasites. Science 164, 839–842 (1969).
Rinaldi, A., Filippi, G. & Siniscalco, M. Variability of red cell phenotypes between and within individuals in an unbiased sample of 77 heterozygotes for G6PD deficiency in Sardinia. Am J Hum Genet 28, 496–505 (1976).
Evelyn, K. A. & Malloy, H. T. Microdetermination of oxyhemoglobin, methemoglobin and sulfhemoglobin in a single sample of blood. Journal of Biological Chemistry (1938).
Betke, K. Peroxidase activity of the hemoglobin. Biochem Z 321, 271–291 (1951).
Kleihauer, E. & Betke, K. Elution procedure for the demonstration of methaemoglobin in red cells of human blood smears. Nature 199, 1196–1197 (1963).
Grinstein, M. & Watson, C. J. Studies of protoporphyrin; a simple and improved method for the preparation of pure protoporphyrin from hemoglobin. J Biol Chem 167, 515–519 (1947).
Granick, S. & Levere, R. D. The intracellular localization of heme by a fluorescence technique. J Cell Biol 26, 167–176 (1965).
Schwartz, S., Dahl, J., Ellefson, M. & Ahlquist, D. The “HemoQuant” test: a specific and quantitative determination of heme (hemoglobin) in feces and other materials. Clin Chem 29, 2061–2067 (1983).
Nagababu, E., Chrest, F. J. & Rifkind, J. M. The origin of red cell fluorescence caused by hydrogen peroxide treatment. Free Radic Biol Med 29, 659–663 (2000).
Flynn, T. P., Allen, D. W., Johnson, G. J. & White, J. G. Oxidant damage of the lipids and proteins of the erythrocyte membranes in unstable hemoglobin disease. Evidence for the role of lipid peroxidation. J Clin Invest 71, 1215–1223 (1983).
Kikugawa, K., Kosugi, H. & Asakura, T. Effect of malondialdehyde, a product of lipid peroxidation, on the function and stability of hemoglobin. Arch Biochem Biophys 229, 7–14 (1984).
Beutler, E. G6PD: population genetics and clinical manifestations. Blood Rev 10, 45–52 (1996).
Nagababu, E. & Rifkind, J. M. Reaction of hydrogen peroxide with ferrylhemoglobin: superoxide production and heme degradation. Biochemistry 39, 12503–12511 (2000).
Guindo, A., Fairhurst, R. M., Doumbo, O. K., Wellems, T. E. & Diallo, D. A. X-linked G6PD deficiency protects hemizygous males but not heterozygous females against severe malaria. PLoS Med 4, e66 (2007).
Hahne, F. et al. flowCore: a Bioconductor package for high throughput flow cytometry. BMC Bioinformatics 10, 106 (2009).
Acknowledgements
We thank all the children and their families who participated in this study and Saibou Doumbia, Drissa Konate, Mory Doumbia and Dick Sakai for their efforts in support of this work. This study was supported by the Intramural Research Program of the NIAID, NIH.
Author information
Authors and Affiliations
Contributions
SS designed the study in collaboration with RMF, TEW, MD, KAR and DPK. SD and KT performed the genotyping work. SS designed, validated and performed all enzyme activity and cytofluorometric assays. SS conducted all statistical analyses. SS and RF wrote the paper and all authors reviewed the manuscript.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareALike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Shah, S., Diakite, S., Traore, K. et al. A novel cytofluorometric assay for the detection and quantification of glucose-6-phosphate dehydrogenase deficiency. Sci Rep 2, 299 (2012). https://doi.org/10.1038/srep00299
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep00299
This article is cited by
-
A fluorometric assay to determine the protective effect of glucose-6-phosphate dehydrogenase (G6PD) against a Plasmodium spp. infection in females heterozygous for the G6PD gene: proof of concept in Plasmodium falciparum
BMC Research Notes (2022)
-
Cut-off values for diagnosis of G6PD deficiency by flow cytometry in Thai population
Annals of Hematology (2022)
-
Determining a critical threshold for G6PD activity below which red blood cell response to oxidative stress is poor
Malaria Journal (2020)
-
Molecular phenotyping of oxidative stress in diabetes mellitus with point-of-care NMR system
npj Aging and Mechanisms of Disease (2020)
-
Bead-based assays to simultaneously detect multiple human inherited blood disorders associated with malaria
Malaria Journal (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
