
Abstract
Personal social network size exhibits considerable variation in the human population and is associated with both physical and mental health status. Much of this inter-individual variation in human sociality remains unexplained from a biological perspective. According to the brain opioid theory of social attachment, binding of the neuropeptide β-endorphin to μ-opioid receptors in the central nervous system (CNS) is a key neurochemical mechanism involved in social bonding, particularly amongst primates. We hypothesise that a positive association exists between activity of the μ-opioid system and the number of social relationships that an individual maintains. Given the powerful analgesic properties of β-endorphin, we tested this hypothesis using pain tolerance as an assay for activation of the endogenous μ-opioid system. We show that a simple measure of pain tolerance correlates with social network size in humans. Our results are in line with previous studies suggesting that μ-opioid receptor signalling has been elaborated beyond its basic function of pain modulation to play an important role in managing our social encounters. The neuroplasticity of the μ-opioid system is of future research interest, especially with respect to psychiatric disorders associated with symptoms of social withdrawal and anhedonia, both of which are strongly modulated by endogenous opioids.
Similar content being viewed by others

Introduction
The origin of societies is considered one of the major evolutionary transitions1. This has been accomplished by numerous species but arguably no society is as widespread, complex and technologically advanced as our own. The human brain has evolved to thrive in social environments, providing us with the cognitive processing power to deal with our dynamic and intricate personal relationships2. However, there is limited understanding of the neurobiological processes underpinning human sociality. A growing number of studies highlight the important role played by endogenous opioid peptides, most notably β-endorphin, in affiliation and bonding in social animals such as rodents and primates, including humans3,4. This neuropeptide is released from the CNS and has the highest binding affinity for μ-opioid receptors, which are widely distributed in the brain5. Upon binding, β-endorphin induces analgesia and a sense of well-being6,7. The brain opioid theory of social attachment8 postulates that the endogenous μ-opioid system is fundamental to the establishment and maintenance of social bonds. Indeed, μ-opioid neurotransmission has been shown to modulate social motivation4 and plays a key role in attributing positive value to social interactions9. Specifically, the close relationship between the opioid and dopamine systems is integral to the rewarding nature of social interactions10.
Until relatively recently, experimental evidence supporting the role of the endogenous opioid system in modulating social behaviour mainly derived from the administration of opioids and opioid blockers3,11. For instance, humans given the μ-opioid antagonist naltrexone experience feelings of reduced social connection12. With advances in genetics, knockout technology has revealed that mice lacking the μ-opioid receptor gene show severe deficits in numerous facets of social behaviour, including interactions with conspecifics, communication and infant attachment13,14. Furthermore, there is increasing interest in the use of positron emission tomography (PET) scanning to measure activity of the μ-opioid system in relation to differences in social behaviour, both within individuals (Manninen et al. in prep) and between individuals15.
Since β-endorphin is a potent analgesic, indeed more so than the pain-relieving opiate drug morphine16, the primary hypothesis tested here was whether pain tolerance (as a proxy for activation of the μ-opioid system) predicts social network size. We tested this hypothesis in a population of healthy young adults (n = 101). The study involved a questionnaire relating to the two innermost social network layers (approximately corresponding to those individuals contacted at least once a week and once a month respectively), as well as collecting information on personality, sociodemographics and lifestyle. Since the blood-brain barrier is impermeable to β-endorphin, CNS endorphin levels can only be accurately determined by sampling cerebrospinal fluid3 via lumbar puncture, whilst measuring the μ-opioid system directly requires the use of PET scanning17. Instead, pain tolerance was assessed by means of a non-invasive, physical pain test (see Methods).
Results
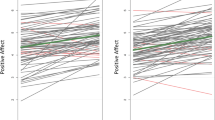
Multiple regression analysis (see Supplementary Tables S1–3) revealed pain tolerance to be a significant predictor of social network size (P = 0.010), in particular the size of an individual’s outer network layer (P = 0.002, Fig. 1). This corresponds to members of their network whom they are typically in contact with at least monthly but less frequently than once a week. The personality trait agreeableness also positively predicted network size but was negatively related to pain tolerance and thus proved not to mediate the above relationship (Supplementary Tables S4–6). Notably, there were no significant gender differences in pain test performance (t99 = −1.144, P = 0.255). Since pain tolerance is inferred from the length of time participants can endure the physical pain test, individuals with higher self-rated fitness performed significantly better, as anticipated (Supplementary Tables S4–6). However, fitter individuals also had smaller social networks, particularly the outer network layer (P = 0.021) and so fitness was not a confounding variable in the relationship between pain tolerance and network size. The analysis also revealed stress to be a significant negative predictor of outer social network size (P = 0.023), with individuals who reported higher stress levels having smaller networks.

Relationship between pain tolerance and social network size.
Pain tolerance is a significant predictor of an individual’s social network size (P = 0.010), especially the size of their outer network layer (P = 0.002) as depicted here. This represents those individuals contacted at least monthly, but less frequently than once a week. Pain tolerance is plotted as the natural log transformation of pain test time and the reduced major axis regression line is shown.
Discussion
Our results show that pain tolerance positively predicts social network size. This therefore supports our hypothesis that variation in the μ-opioid system underlies individual differences in sociality. These results are consistent with a recent PET imaging experiment demonstrating a correlation between μ-opioid receptor availability and attachment style, such that individuals showing greater avoidance of social attachment exhibit lower receptor densities15. Our findings are also in agreement with previous pain tolerance studies indirectly implicating the endogenous opioid system in human social bonding activities such as music-making18, dancing19 and laughter20. In addition, laughter has since been shown to correlate with elevated μ-opioid activity, as measured by PET scanning (Manninen et al. in prep). This suggests that tests of pain tolerance like that used in our study may indeed serve as a useful proxy for assessing activation of the μ-opioid system.
Variation in μ-opioid receptor signalling may be due to underlying differences in both endogenous opioid release and receptor density, though their relative contribution is yet to be fully determined. However, studies of oxytocin and vasopressin signalling in rodents have shown that CNS receptor densities strongly modulate the influence of these neuropeptides, irrespective of neuropeptide abundance21. In fact, analyses of post-mortem brain tissue and in vivo PET studies in humans have revealed a broad range of μ-opioid receptor densities within the population, differing by at least 30–50%22. Such variation is likely to considerably affect the potency of β-endorphin11. Genetic studies suggest these differences in receptor density are partly the result of a non-synonymous single-nucleotide polymorphism in the μ-opioid receptor gene (OPRM1), substituting aspartic acid for asparagine (A118G)23. This functional polymorphism is relatively common in the population, with the minor G allele having a frequency of 10–30%24 and is associated with reduced μ-opioid receptor expression24,25. The G allele has also been linked to increased social withdrawal26 and reactivity to social rejection27, as well as greater pain sensitivity and reduced relief from opiate drugs28. This is therefore in line with our proposition that variation in the μ-opioid system contributes to individual differences in both social behaviour and pain tolerance.
We acknowledge that use of pain tolerance as a proxy for μ-opioid receptor signalling, rather than its direct measurement, represents a limitation of our research. However, the μ-opioid system is critically involved in pain modulation6,29 and numerous PET studies implicate μ-opioidergic activation in both experimental and clinical pain settings30. Most notably, in humans undergoing a sustained muscular pain challenge, individuals exhibiting higher activity of the μ-opioid system report reduced sensory and affective pain31. A possible future direction that would benefit research in this field would be to combine PET scanning with a range of different pain tests to determine how reliably they can predict activity of the μ-opioid system. We also recognise the possible involvement of non-opioid signalling pathways, especially given the complex neurochemistry underlying pain responses32,33. In particular, oxytocin, vasopressin and endocannabinoids are all implicated in social behaviour34,35, as well as having analgesic effects36,37,38. Indeed, it is likely that they act in concert with β-endorphin39,40,41.
Further research is required to understand the causality of this relationship between pain tolerance and network size. It may be that individuals with genetic variants conferring enhanced μ-opioid neurotransmission derive greater reward from social interactions, thereby seeking more company. An alternative, though not mutually exclusive, explanation is that individuals leading lives rich in social interactions may release higher levels of endogenous opioids and/or have elevated receptor expression. However, we currently lack knowledge regarding the neuroplasticity exhibited by the μ-opioid system. This is of particular interest in relation to psychiatric disorders. Indeed, healthy females asked to sustain a sad mood for only 30 minutes show a reduction in μ-opioid receptor activation42. Thus prolonged sadness, as experienced by those suffering from depression, may over time lead to a significant fall in opioidergic signalling. We hypothesise that reduced μ-opioid activity may characterise the onset of conditions such as depression and schizophrenia, resulting in the common symptoms of anhedonia and social withdrawal. Indeed, endogenous opioids mediate hedonic experiences and are integral to our feelings of social connection8,12. In support of this, there is evidence of compromised μ-opioid receptor signalling in patients suffering from depression and schizophrenia43,44 and studies using rodent models of depression also implicate the μ-opioid system45.
With respect to the other notable results of our analysis, fitness was primarily included in the regression model to account for its influence on pain tolerance but revealed an interesting and novel negative relationship with network size. This indicates a trade-off between leading a socially active versus a physically active life. Beyond the obvious constraint of time, this relationship may reflect our underlying neurobiology such that individuals who exercise more may have greater reliance on this method of promoting β-endorphin release, rather than through social interactions. Though exercise is frequently prescribed as a treatment for depression, perhaps focus should also be placed on strengthening and expanding an individual’s social ties.
The relationship reported here between stress and network size may reflect the beneficial effects of social support in dealing with stressful situations46, since measures of social support often correlate with social network size47. Interestingly, one study found that the number of Facebook friends (a known correlate of real-world social network size48) is associated with enhanced perceptions of social support and reduced stress49. Whether online social networks play a role in relieving stress (or even intensifying it) over and above an individual’s actual social interactions remains uncertain. However, an alternative interpretation of our data is that stressed individuals find less time for social engagement and thus their network decreases in size.
Understanding the biological causes of variation in social network size is of particular interest given the robust association between an individual’s social support and their health, ranging from functioning of their immune, endocrine and cardiovascular systems46 to myelin integrity50. Interestingly, it is an individual’s perceived level of social support that may often be a more reliable indicator of their health status46,51. Compared to other lifestyle factors, we have limited understanding of the mechanisms via which sociality influences morbidity and mortality risk52, though reduced activation of the neuroendocrine stress response likely plays a significant role in both humans51,53 and animals54. Since β-endorphin is known to alleviate the stress response55 and protect against inflammation and cancer56, the activity of an individual’s endogenous μ-opioid system may have important consequences for their health. However, such a direct interaction between social and somatic health is yet to be explored.
In summary, there is substantial evidence that μ-opioid neurotransmission influences sensitivity not only to our physical environment but also our social one. This study adds to previous research implicating the μ-opioid system as a key neural substrate upon which human sociality has evolved. A better understanding of the neurobiological mechanisms underpinning our social lives is imperative, especially since our technology-driven world is rapidly changing the nature of social relationships and certainly outpacing any biological adaptations. Sociality is clearly of adaptive value to our species, yet in this digital era deficiencies in our social interactions may be one of the overlooked factors contributing to the declining health of our modern society.
Methods
Participants
The study was advertised for healthy adults aged 18–35 years, recruited predominantly from the University of Oxford. Exclusion criteria were recreational drug use or drug replacement therapy. Participants were requested not to consume alcohol (within 24 hours) or smoke (within 3 hours) prior to the study, given the analgesic properties of these substances.
The mean age of respondents was 21.7 years (range = 18–34 years). In total 107 subjects (30 males and 77 females) took part in the study. Six data points were excluded from the analysis due to either questionnaire inadequacies or failure to perform the pain test correctly. The study was approved by the University of Oxford’s Medical Sciences Inter-Divisional Research Ethics Committee and the methods were carried out in accordance with the approved guidelines. All participants gave written informed consent.
Questionnaires
The social network questionnaire was designed to collect data relating to the two innermost layers of a participant’s social network, corresponding to those individuals contacted on a weekly and monthly basis respectively57. The 50-item IPIP (International Personality Item Pool) inventory58 was used to score individuals on each of the ‘Big-Five’ personality traits (openness, conscientiousness, extraversion, agreeableness and neuroticism). Respondents also provided basic sociodemographic and health information, along with self-rated assessments of their fitness and stress levels.
Pain tolerance test
Given the invasive nature of PET imaging, pain tolerance is often used as a conventional assay in studies of the endogenous opioid system18,19,20. Participants performed an isometric quadriceps exercise (commonly known as the wall sit test) which involves squatting against the wall with knees at a 90° angle and a straight back. They were asked to hold this position and endure the discomfort for as long as possible and the time was recorded to the nearest second. The main advantages of this pain test are that it is non-invasive, does not require any specialist equipment and is quick to conduct, with an average time of 113 s (range = 26–394 s).
Statistical analyses
Analyses were performed using R 3.2.3 software59 and all tests were conducted with an α level of 0.05. The construction of general linear models was guided by the Akaike Information Criterion, incorporating pain tolerance, self-rated fitness, stress and agreeableness as predictors of network size. Where necessary the appropriate variables were transformed, including natural log transformation of the pain test times, such that model residuals were normally distributed (Shapiro-Wilk test, P > 0.05) and satisfied the assumption of homoscedasticity (non-constant variance test, P > 0.05). The relationship between pain tolerance and social network size was plotted using the reduced major axis regression line which minimises the sum of the product of residuals in both the x and y directions. Partial correlations between variables were also calculated and the absence of multicollinearity confirmed using variance inflation factors. For analysis involving comparison of means, Student’s two-sample t-test (two-tailed) was conducted.
Additional Information
How to cite this article: Johnson, K. V.-A. and Dunbar, R. I. M. Pain tolerance predicts human social network size. Sci. Rep. 6, 25267; doi: 10.1038/srep25267 (2016).
References
Maynard Smith, J. & Szathmáry, E. The major transitions in evolution. Ch. 16, 255–278 (Oxford University Press, 1997).
Dunbar, R. I. M. The social brain hypothesis. Evol. Anthropol. 6, 178–190 (1998).
Machin, A. J. & Dunbar, R. I. M. The brain opioid theory of social attachment: a review of the evidence. Behaviour 148, 985–1025 (2011).
Loseth, G. E., Ellingsen, D.-M. & Leknes, S. State-dependent μ-opioid modulation of social motivation. Front. Behav. Neurosci. 8, 430, doi: 10.3389/fnbeh.2014.00430 (2014).
Pasternak, G. W. & Pan, Y.-X. Mu opioids and their receptors: evolution of a concept. Pharmacol. Rev. 65, 1257–1317 (2013).
Rubinstein, M. et al. Absence of opioid stress-induced analgesia in mice lacking β-endorphin by site-directed mutagenesis. Proc. Natl. Acad. Sci. USA 93, 3995–4000 (1996).
Akil, H. et al. Endogenous opioids: biology and function. Annu. Rev. Neurosci. 7, 223–255 (1984).
Panksepp, J. Affective neuroscience: the foundations of human and animal emotions. Ch. 13–14, 246–279 (Oxford University Press, 1998).
Trezza, V., Damsteegt, R., Achterberg, E. J. M. & Vanderschuren, L. J. M. J. Nucleus accumbens μ-opioid receptors mediate social reward. J. Neurosci. 31, 6362–6370 (2011).
Fields, H. L. & Margolis, E. B. Understanding opioid reward. Trends Neurosci. 38, 217–225 (2015).
Depue, R. A. & Morrone-Strupinsky, J. V. A neurobehavioral model of affiliative bonding: implications for conceptualizing a human trait of affiliation. Behav. Brain Sci. 28, 313–350 (2005).
Inagaki, T. K., Irwin, M. R. & Eisenberger, N. I. Blocking opioids attenuates physical warmth-induced feelings of social connection. Emotion 15, 494–500 (2015).
Becker, J. A. J. et al. Autistic-like syndrome in mu opioid receptor null mice is relieved by facilitated mGluR4 activity. Neuropsychopharmacology 39, 2049–2060 (2014).
Moles, A., Kieffer, B. L. & D’Amato, F. R. Deficit in attachment behavior in mice lacking the μ-opioid receptor gene. Science 304, 1983–1986 (2004).
Nummenmaa, L. et al. Adult attachment style is associated with cerebral μ-opioid receptor availability in humans. Hum. Brain Mapp. 36, 3621–3628 (2015).
Loh, H. H., Tseng, L. F., Wei, E. & Li, C. H. β-endorphin is a potent analgesic agent. Proc. Natl. Acad. Sci. USA 73, 2895–2898 (1976).
Henriksen, G. & Willoch, F. Imaging of opioid receptors in the central nervous system. Brain 131, 1171–1196 (2008).
Dunbar, R. I. M., Kaskatis, K., Macdonald, I. & Barra, V. Performance of music elevates pain threshold and positive affect: implications for the evolutionary function of music. Evol. Psychol. 10, 688–702 (2012).
Tarr, B., Launay, J., Cohen, E. & Dunbar, R. I. M. Synchrony and exertion during dance independently raise pain threshold and encourage social bonding. Biol. Lett. 11, 10, doi: 10.1098/rsbl.2015.0767 (2015).
Dunbar, R. I. M. et al. Social laughter is correlated with an elevated pain threshold. Proc. R. Soc. B Biol. Sci. 279, 1161–1167 (2012).
McCall, C. & Singer, T. The animal and human neuroendocrinology of social cognition, motivation and behavior. Nat. Neurosci. 15, 681–688 (2012).
Uhl, G. R., Sora, I. & Wang, Z. The μ opiate receptor as a candidate gene for pain: polymorphisms, variations in expression, nociception and opiate responses. Proc. Natl. Acad. Sci. USA 96, 7752–7755 (1999).
Bond, C. et al. Single-nucleotide polymorphism in the human mu opioid receptor gene alters β-endorphin binding and activity: possible implications for opiate addiction. Proc. Natl. Acad. Sci. USA 95, 9608–9613 (1998).
Zhang, Y., Wang, D., Johnson, A. D., Papp, A. C. & Sadée, W. Allelic expression imbalance of human mu opioid receptor (OPRM1) caused by variant A118G. J. Biol. Chem. 280, 32618–32624 (2005).
Mague, S. D. et al. Mouse model of OPRM1 (A118G) polymorphism has sex-specific effects on drug-mediated behavior. Proc. Natl. Acad. Sci. USA 106, 10847–10852 (2009).
Bertoletti, E., Zanoni, A., Giorda, R. & Battaglia, M. Influence of the OPRM1 gene polymorphism upon children’s degree of withdrawal and brain activation in response to facial expressions. Dev. Cogn. Neurosci. 2, 103–109 (2012).
Way, B. M., Taylor, S. E. & Eisenberger, N. I. Variation in the mu-opioid receptor gene (OPRM1) is associated with dispositional and neural sensitivity to social rejection. Proc. Natl. Acad. Sci. USA 106, 15079–15084 (2009).
Peciña, M., Love, T., Stohler, C. S., Goldman, D. & Zubieta, J.-K. Effects of the mu opioid receptor polymorphism (OPRM1 A118G) on pain regulation, placebo effects and associated personality trait measures. Neuropsychopharmacology 40, 957–965 (2015).
Al-Hasani, R. & Bruchas, M. R. Molecular mechanisms of opioid receptor-dependent signaling and behavior. Anesthesiology 115, 1363–1381 (2011).
Sprenger, T., Berthele, A., Platzer, S., Boecker, H. & Tölle, T. R. What to learn from in vivo opioidergic brain imaging? Eur. J. Pain 9, 117–121 (2005).
Zubieta, J.-K. et al. Regional mu opioid receptor regulation of sensory and affective dimensions of pain. Science 293, 311–315 (2001).
Watkins, L. R. & Mayer, D. J. Organization of endogenous opiate and nonopiate pain control systems. Science 216, 1185–1192 (1982).
Denk, F., McMahon, S. B. & Tracey, I. Pain vulnerability: a neurobiological perspective. Nat. Neurosci. 17, 192–200 (2014).
Donaldson, Z. R. & Young, L. J. Oxytocin, vasopressin and the neurogenetics of sociality. Science 322, 900–904 (2008).
Wei, D. et al. Endocannabinoid signaling mediates oxytocin-driven social reward. Proc. Natl. Acad. Sci. USA 112, 14084–14089 (2015).
Rash, J. A., Aguirre-Camacho, A. & Campbell, T. S. Oxytocin and pain: a systematic review and synthesis of findings. Clin. J. Pain 30, 453–462 (2014).
Mogil, J. S. et al. Pain sensitivity and vasopressin analgesia are mediated by a gene-sex-environment interaction. Nat. Neurosci. 14, 1569–1573 (2011).
Guindon, J. & Hohmann, A. G. The endocannabinoid system and pain. CNS Neurol. Disord. Drug Targets 8, 403–421 (2009).
Gao, L. & Yu, L.-C. Involvement of opioid receptors in the oxytocin-induced antinociception in the central nervous system of rats. Regul. Pept. 120, 53–58 (2004).
van de Heijning, B. J. M., Koekkoek-van den Herik, I. & van Wimersma Greidanus, T. B. The opioid receptor subtypes μ and κ, but not δ, are involved in the control of the vasopressin and oxytocin release in the rat. Eur. J. Pharmacol. 209, 199–206 (1991).
Befort, K. Interactions of the opioid and cannabinoid systems in reward: insights from knockout studies. Front. Pharmacol. 6, 6, doi: 10.3389/fphar.2015.00006 (2015).
Zubieta, J.-K. et al. Regulation of human affective responses by anterior cingulate and limbic μ-opioid neurotransmission. Arch. Gen. Psychiatry 60, 1145–1153 (2003).
Bernstein, H. et al. Fewer beta-endorphin expressing arcuate nucleus neurons and reduced beta-endorphinergic innervation of paraventricular neurons in schizophrenics and patients with depression. Cell. Mol. Biol. 48, 259–265 (2002).
Hsu, D. T. et al. It still hurts: altered endogenous opioid activity in the brain during social rejection and acceptance in major depressive disorder. Mol. Psychiatry 20, 193–200 (2015).
Lutz, P.-E. & Kieffer, B. L. Opioid receptors: distinct roles in mood disorders. Trends Neurosci. 36, 195–206 (2013).
Uchino, B. N., Cacioppo, J. T. & Kiecolt-Glaser, J. K. The relationship between social support and physiological processes: a review with emphasis on underlying mechanisms and implications for health. Psychol. Bull. 119, 488–531 (1996).
Graham, J. E., Christian, L. M. & Kiecolt-Glaser, J. K. In Psychoneuroimmunology 4th edn, Vol. 2 (ed. Ader, R. ) Ch. 36, 781–798 (Academic Press, 2007).
Kanai, R., Bahrami, B., Roylance, R. & Rees, G. Online social network size is reflected in human brain structure. Proc. R. Soc. B Biol. Sci. 279, 1327–1334 (2012).
Nabi, R. L., Prestin, A. & So, J. Facebook friends with (health) benefits? Exploring social network site use and perceptions of social support, stress and well-being. Cyberpsychol. Behav. Soc. Netw. 16, 721–727 (2013).
Molesworth, T., Sheu, L. K., Cohen, S., Gianaros, P. J. & Verstynen, T. D. Social network diversity and white matter microstructural integrity in humans. Soc. Cogn. Affect. Neurosci. 10, 1169–1176 (2015).
Yang, Y. C. et al. Social relationships and physiological determinants of longevity across the human life span. Proc. Natl. Acad. Sci. USA 113, 578–583 (2016).
Holt-Lunstad, J., Smith, T. B. & Layton, J. B. Social relationships and mortality risk: a meta-analytic review. PLoS Med. 7, e1000316 (2010).
Eisenberger, N. I., Taylor, S. E., Gable, S. L., Hilmert, C. J. & Lieberman, M. D. Neural pathways link social support to attenuated neuroendocrine stress responses. Neuroimage 35, 1601–1612 (2007).
Silk, J. B. et al. Strong and consistent social bonds enhance the longevity of female baboons. Curr. Biol. 20, 1359–1361 (2010).
Bali, A., Randhawa, P. K. & Jaggi, A. S. Stress and opioids: role of opioids in modulating stress-related behavior and effect of stress on morphine conditioned place preference. Neurosci. Biobehav. Rev. 51, 138–150 (2015).
Sarkar, D. K., Murugan, S., Zhang, C. & Boyadjieva, N. Regulation of cancer progression by β-endorphin neuron. Cancer Res. 72, 836–840 (2012).
Roberts, S. G. B., Wilson, R., Fedurek, P. & Dunbar, R. I. M. Individual differences and personal social network size and structure. Pers. Individ. Dif. 44, 954–964 (2008).
Goldberg, L. R. International Personality Item Pool (2001). Available at: http://ipip.ori.org/. (Accessed: 13th April 2015).
R Development Core Team (2015). R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. Available at: http://www.R-project.org.
Acknowledgements
We acknowledge support from BBSRC (K.V.-A.J.) and ERC (R.I.M.D.).
Author information
Authors and Affiliations
Contributions
K.V.-A.J. designed and conducted the study, performed the analyses and wrote the manuscript. R.I.M.D. conceived and supervised the overall project.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Johnson, KA., Dunbar, R. Pain tolerance predicts human social network size. Sci Rep 6, 25267 (2016). https://doi.org/10.1038/srep25267
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep25267
This article is cited by
-
Only empathy-related traits, not being mimicked or endorphin release, influence social closeness and prosocial behavior
Scientific Reports (2023)
-
Bending and bonding: a randomized controlled trial on the socio-psychobiological effects of spiritual versus secular yoga practice on social bonding
Current Psychology (2023)
-
Mu opioid receptor gene (OPRM1) moderates the influence of perceived parental attention on social support seeking
Adaptive Human Behavior and Physiology (2022)
-
Physical, Emotional, and Social Pain During COVID-19 Pandemic-Related Social Isolation
Trends in Psychology (2022)
-
Opposing effects of antibiotics and germ-free status on neuropeptide systems involved in social behaviour and pain regulation
BMC Neuroscience (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
