
Abstract
Physical activity (PA) is linked to a decreased risk of type 2 diabetes mellitus (T2DM). However, the influence of circadian PA trajectories remains uncertain. This study aims to explore the optimal circadian PA trajectory pattern for reducing the risk of T2DM. Methods: A total of 502,400 participants were recruited from the UK Biobank between 2006 and 2010, and 102,323 participants provided valid accelerometer-captured acceleration data. After excluding individuals with prior T2DM, 99,532 participants were included in the final analysis. We initially investigated the association between PA intensity at 24 hourly time points and T2DM. Subsequently, PA trajectories were identified using K-means cluster analysis. Cox proportional hazard models were employed to estimate hazard ratios (HR). Four distinct PA trajectories were identified: consistently low, single peak, double peak, and intense trajectories. Compared to consistently low, single peak, double peak and intense PA trajectory reduced the risk of T2DM progressively. Sensitivity analyses, further excluding individuals with glycated hemoglobin (HbA1c) ≥ 6.5% or random glucose ≥ 11.1 mmol/L and adjusted for daily average acceleration, yielded consistent results. This confirms that the ideal circadian PA trajectory serves as a protective factor, independently of PA intensity. Subgroup analyses indicated that these effects were more pronounced in men and individuals with eGFR < 60 mL/(min*1.73 m2). In conclusion, ideal circadian PA trajectory patterns (especially intense and then double peak) reduced risk of T2DM.
Similar content being viewed by others


Introduction
Physical activity (PA) is a preventive factor for type 2 diabetes mellitus (T2DM)1,2,3, yet the role of circadian PA trajectory patterns remains relatively unexplored. Most studies, such as those by Duncan4 and Castetbon5, rely on questionnaires to gauge PA metrics. These questionnaires are often crude and subjective, overlooking many nuances of PA. Additionally, an increasing of research has delved into the relationship between circadian rhythm and health outcomes6,7,8,9,10. Disruptions in circadian rhythm have been associated with a range of diseases, including obesity11, cardiovascular events7, and mortality12. Growing evidence also suggests that the pattern of PA is an independent determinant of T2DM risk11. However, recommendations regarding the optimal PA patterns remain under discussion. Given the challenges of real-time activity data collection, it remains unclear which PA pattern offers the greatest health benefits, especially in the absence of evidence from large-scale cohorts. Few studies have addressed the relationship between PA trajectories and type 2 diabetes. The advent of wrist-worn triaxial accelerometers13 has bridged this gap, capturing continuous activity data in a precise manner, facilitating research into the optimal 24-h PA trajectory patterns. Furthermore, cluster trajectory models offer a more intuitive, granular approach to identify potential subgroups based on temporal measures, while trajectory models are traditionally suited for cohort data14,15,16, the repeated measures of PA acceleration captured by accelerometer bear similarities. Previous studies often singularly focused on either the intensity or the variation of PA, which was somewhat one-sided. In this study, through K-means clustering trajectory analysis, we identified the PA trajectories in the population that encompass both aspects. This provides a more comprehensive and precise depiction, capturing the actual PA behaviours and patterns of individuals. Thus, trajectories of circadian PA patterns might offer fresh insights.
Therefore, our study, based on a large population cohort from the UK Biobank, identifies circadian PA trajectories. We aimed to evaluate the optimal PA trajectories by examining their association with type 2 diabetes incidence. We further sought to reinforce the robustness of our findings through sensitivity analyses and to uncover variations in specific populations via subgroup analyses.
Results
Identification of circadian PA trajectories
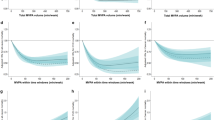
Based on continuous monitoring acceleration data and circadian rhythm temporal distribution from accelerometer over a span of 24 h of participants in this study, the K-means clustering algorithm discerned four potential trajectory groups, as depicted in Fig. 1. The first group, termed the “consistently low Group”, comprised 13.8% of the participants. This group demonstrated consistently lower daily PA acceleration levels throughout the day, below 23.37 mg (milligravity). The second group, encompassing 47.7% of the participants, was termed “single peak”. This group was characterized by relatively higher PA acceleration levels in the morning, reaching 45.54 mg. In contrast, the third group, termed “double peak”, consisted of 18.8% of participants. This group displayed two distinct PA level peaks: one in the morning at 57.09 mg and another later in the afternoon at 50.65 mg. The fourth group, termed “intense”, accounted for 19.7% of participants, characterized by high PA acceleration levels during the day, peaking at a 74.26 mg.

Trajectory groups of PA patterns in this study. Trajectory Cluster were based on continuous monitoring acceleration data and circadian rhythm temporal distribution from accelerometer over a span of 24 h.
Participant characteristics across different trajectory groups
Our analysis encompassed 99,532 participants, with 42,902 men and 56,630 women. The mean age at baseline was 56 years, standard deviation (SD) 7.8 years. 13.8% of participants (Group 1) displayed a relatively steady low level of PA during the day, without evident PA intensity peaks.
Typically, these participants were older men with a higher BMI and smoking history. In contrast, 19.7% of participants (Group 4) exhibited higher activity intensities. This group predominantly consisted of younger women with higher education and income levels. Detailed demographic and feature breakdowns are provided in Table 1; Table S1.
Hourly PA and incident type 2 diabetes
During the follow-up period, 2,692 incident diabetes cases were identified according to ICD-10 codes: E11. Association between PA over 24 h and T2DM were evaluated, higher relative PA during nighttime hours (00:00–6:00am) was associated with increased risk, while morning (8:00–11:00am) and late afternoon (18:00–20:00pm) physical activities were linked to lower risk (Fig. 2A, in mod3 fully adjusted for gender, age, ethnicity, education level, income, BMI, smoking status, eGFR, CRP, and medical history of cardiovascular disease and cancer). The highest HR (95% CI) for T2DM with Hourly PA occurred at 4:00 am, with a value of 1.12 (1.04–1.21), while the two lowest HR (95% CI) values for T2DM were observed at 20:00 pm, with a value of 0.90 (0.88–0.93), and at 11:00 am, with a value of 0.91 (0.90–0.93).

Hourly PA and T2DM risk distribution in 24 h. (A) shows the risk on incident T2DM risk in mod3; (B) also shows association of T2DM risk with 24-hourly acceleration in mod1 and mod2. Model 1 adjusted for gender, age, and ethnicity. Model 2 further adjusted for education level, income, BMI, and smoking based on Model 1. Model 3 further adjusted for eGFR, CRP, and medical history of cardiovascular disease and cancer based on Model 2.
Figure 2B shows HR (95% CI) for T2DM with hourly PA in different models. And the HR (95% CI%) corresponding to specific 24-hourly PA are presented in Table S2, as well as the outcomes for the population further excluded individuals with HbA1c levels ≥ 48 mmol/mol (6.5%) or random glucose levels ≥ 11.1 mmol/L at baseline according to ADA standards presented in Figure S1, Table S3. This preliminary analysis suggests an association between the time distribution of PA throughout the day and T2DM risk.
Association between PA trajectory groups and T2DM incidence
Based on PA trajectories identified by continuous PA trends, Fig. 3 provided a visual representation for the associations between circadian PA trajectories and T2DM. Compared to the consistently low group, the single peak, double peak, and intense groups displayed progressively reduced risks associated with overall T2DM incidence. Specifically, in comparison to the consistently low pattern, the HR (95% CI) of T2DM risk with PA trajectories in single peak, double peak, and intense trajectories were 0.78 (0.71–0.85), 0.60 (0.52–0.69), and 0.48 (0.41–0.56) respectively in mod3, fully adjusted for gender, age, ethnicity, education level, income, BMI, smoking status, eGFR, CRP, and medical history. In mod1 and mod2, ideal circadian exercise trajectory patterns similarly displayed an inverse association with T2DM risk, the HR (95% CI) in single peak, double peak, and intense trajectories were respectively 0.58(0.53–0.64), 0.37(0.32–0.42), 0.27 (0.24–0.32) and 0.77 (0.71–0.85), 0.60 (0.52–0.69), 0.48 (0.41–0.56). Association of incident T2DM with 24-hourly PA acceleration using the single peak, double peak, and intense group as a reference, yielded consistent results (Figure S2).

Association of incident T2DM with PA trajectories in mod1, mod2 and mod3. Model 1 adjusted for gender, age, and ethnicity. Model 2 further adjusted for education level, income, BMI, and smoking based on Model 1. Model 3 further adjusted for eGFR, CRP, and medical history of cardiovascular disease and cancer based on Model 2.
Sensitivity analysis
To ensure test result stability, further exclusions were made from those diagnosed with T2DM, and individuals with random glucose levels ≥ 11.1 mmol/L or HbA1c levels ≥ 48 mmol/mol (6.5%). The associations between PA trajectory groups and T2DM incidence remained consistent (Figure S3). Compared to the consistently low group, the HR (95% CI) of T2DM risk with PA trajectories for single peak, double peak, and intense trajectories were 0.60 (0.54–0.66), 0.36 (0.31–0.42) and 0.28 (0.24–0.33) in mod1, 0.79 (0.71–0.87) 0.59 (0.50–0.69) and 0.49 (0.42–0.58) in mod2, 0.80 (0.72–0.89),0.61 (0.52–0.73) and 0.50 (0.42–0.60) in mod3.
Additionally, we further adjusted for all-day average acceleration on top of all confounders in mod3. The ideal PA trajectory groups remained a significant protective factor for T2DM, compared to the consistently low group, the HR (95% CI) for single peak, double peak, and intense trajectories were 0.90 (0.80–1.02), 0.79 (0.64–0.96) and 0.68 (0.54–0.86) (Figure S4). Besides, considering some relevant occupational factors, we adjusted for jobs involving night shifts, PA work and unemployment, and yielded consistent results (Figure S5).
Subgroup analysis
We conducted subgroup analyses based on gender, age, BMI, eGFR, CRP, and medical history of cardiovascular disease and cancer. As showed in Table 2, the protective trend of ideal exercise trajectories remained consistent across all subgroups. However, the strength of the protective effect varied, especially for men and those with eGFR < 60mL/(min*1.73 m2). HR (95% CI) of T2DM risk with PA trajectories for single peak, double peak, and intense trajectories were 0.76 (0.65–0.88), 0.70 (0.56–0.88) and 0.54 (0.43–0.69) in women; 0.80 (0.71–0.89), 0.54 (0.45–0.65) and 0.44 (0.37–0.54) in men; 0.78 (0.71–0.86), 0.61 (0.53–0.71) and 0.49 (0.42–0.57) in population with eGFR ≥ 60 mL/(min*1.73 m2); 0.71 (0.44–1.14), 0.33 (0.10–1.13) and 0.26 (0.08–0.86) in population with eGFR < 60 mL/(min*1.73 m2). Double peak and intense PA trajectories offered more pronounced protection subgroups of men and eGFR < 60mL/(min*1.73 m2). Specifically, compared to the consistently low pattern, the T2DM risk reduction for double peak, and intense groups were 30% and 46% for women; 46% and 56% for men; 39% and 51% for eGFR ≥ 60 mL/(min*1.73 m2); 67% and 74% for eGFR < 60 mL/(min*1.73 m2).
Discussion
In this large-scale prospective cohort study based on the UK Biobank, we identified four distinct PA trajectory patterns according to intensity and circadian rhythm distribution. We discovered that the optimal PA trajectory offers protective effects against the onset of T2DM. PA remains one of the most evident cornerstones in the prevention of T2DM. Our study adds fresh insights to previous evidence, suggesting that the PA trajectory is another independent influencer of T2DM risk, introducing a new dimension to T2DM risk prevention.
To our knowledge, this is the first study to prospectively analyse the relationship between 24-h PA trajectory patterns and T2DM incidence in a large population. By continuously monitoring the activity of nearly 100,000 individuals over seven days using accelerometer, this study allowed for the exploration of circadian rhythm distribution and the cumulative effects of PA. We discerned four PA trajectories: consistently low, single peak, double peak, and intense group. These results further elucidate the relationship between PA trajectories patterns and health outcomes.
In our analysis, older men exhibited relatively lower PA levels. In contrast, younger, highly-educated women showed a propensity for more intense PA or increased activity in the late afternoon. Numerous studies indicate that PA patterns are influenced by various factors, including physiological, physical environment, social background, and occupational status5,13. For older participants, their daytime PA pattern peaks tend to be lower, consistent with previous findings17. On the other hand, younger individuals have higher daily activity levels and tend to engage in PA later in the day, likely due to indoor occupations commonly held by younger cohorts18,19. Clearly, various PA patterns exist within populations. Analysing these patterns using accelerometer can further identify target populations in need of exercise interventions, offering insights potentially beneficial to public health policy strategies.
Importantly, our study observed variations in T2DM incidence across the four identified PA trajectory groups. After adjusting for all confounders, optimal PA trajectory patterns progressively revealed protective effects against T2DM onset, especially evident in the intense and then double peak trajectory patterns. While consistently low group had the highest T2DM incidence, with PA levels below the World Health Organization's recommendations20, in line with previous findings linking physical inactivity to increased T2DM risk21. Conversely, the "intense group" had the lowest risk. While past studies have shown that any PA offers some benefits over sedentary behaviors21,22,23, our findings underscore the need for exercise to attain specific intensities to maximize health benefits against T2DM onset.
Crucially, even when reaching similar PA intensity peaks, the protective effects of different circadian rhythms differ. We observed that the double peak and single peak groups had comparable peak intensities. However, double peak group, engaging in some activity later in the afternoon, seems to correlate with stronger protective effects, consistent with past studies suggesting that afternoon physical activities have a more positive impact on health24. Although some studies have shown associations between morning PA and better metabolic health25,26,27, others have found that afternoon exercises more effectively improved blood sugar levels than morning exercises28,29. Furthermore, afternoon exercises were more effective in elevating blood lipid levels than morning exercises24,30,31, consistent with the significant circadian rhythm characteristics of cholesterol synthesis, with its lowest during the day and peaking at night32,33. In combination with our study's findings, this underscores the significance of the double peak exercise pattern in preventing T2DM. These findings emphasize that even if some patients face difficulties in maintaining continuous intense exercises, engaging in intermittent moderate-intensity activities throughout the morning and afternoon still provides health benefits.
Sensitivity analyses, further excluding populations according to ADA standards and further adjusting for all-day average acceleration, yielded consistent results, proving that ideal PA trajectory are protective factors against type 2 diabetes, independent from the overall daily average PA intensity. These insights are immensely valuable for clinical practice, highlighting the comprehensive effects of an ideal PA trajectory of all-day exercise regimen on health.
In subgroup analyses based on gender, age, BMI, eGFR, CRP, and medical history of cardiovascular disease and cancer, we observed that the ideal circadian exercise trajectory pattern consistently showcased a protective trend against T2DM risk. Especially in men, the double peak and intense patterns offered stronger protection, possibly due to men generally having more adverse lifestyle habits like higher BMI, smoking, etc34, while the PA trajectory pattern may play a role in improving some of these factors, such as BMI, and they are yet to be further studied as potential mediators affecting the occurrence of T2DM. Simultaneously, the ideal circadian exercise trajectory pattern provided stronger protection for eGFR < 60mL/(min*1.73 m2), possibly because individuals with impaired kidney function have reduced metabolic capabilities35,36,37. The ideal circadian exercise trajectory pattern might regulate the state of circadian metabolic disorder, subsequently reducing diabetes risk. This further emphasizes that in specific populations, the individualized and rational design of exercise patterns, considering exercise intensity and rhythmicity, can help achieve greater health benefits and investigation is needed to explore the underlying mechanisms in greater depth.
This study has several strengths, including its vast sample size and a well-characterized cohort from the UK Biobank. Moreover, PA in the UK Biobank was objectively collected by e wrist-worn accelerometers which can be used to estimate population levels of AEE and TEE in free-living conditions with high precision38 and explain about 44–47% of the variation in PA energy expenditure39. We further employed a data-driven clustering method to identify subgroups of the circadian PA trajectory pattern, more likely representing our participants' natural behavioural pattern than previously used predefined time periods. Lastly, we had the capability to examine the association between circadian PA trajectory patterns and T2DM incidence due to our extensive medical records and baseline data.
We recognize certain limitations in our study. Although we made rigorous efforts to adjust for confounders, the possibility of other unconsidered confounding factors remains. Secondly, given our study's primary focus on a European population cohort, the generalizability of our findings may require validation on a global scale. In this study, through K-means cluster analysis of accelerometer-related data provided by the UK Biobank dataset, four trajectory groups were identified. However, due to variations in economic status, regional culture, and climatic conditions, we acknowledge the potential existence of different PA patterns in other populations, such as an "Evening Only" pattern. While the result of association of hourly PA with T2DM showed that those with higher PA during nighttime hours had a higher risk of T2DM. However, the current study data suggested that, in this British cohort, the proportion of individuals with such a pattern was too small to be identified as a separate cluster. Therefore, future research could consider exploring other potential PA patterns in different regional populations and further investigate their impact on health outcomes, particularly focusing on nighttime PA.
Despite these limitations, this study, with ts strengths, offers fresh content to an unexplored research area, discussing the ideal circadian PA trajectory pattern for preventing T2DM. This lays the groundwork for devising rational physical exercise strategies. If replicated and validated in broader populations in the future, it stands to benefit public health immensely.
Conclusion
Optimal PA trajectories reduced T2DM incidence. The protective effect was not just linked to intensity but also with circadian rhythm distribution. This might suggest that an ideal circadian PA intensity distribution could be an additional beneficial behavioural factor to maximize health benefits and reduce T2DM risk.
Methods
Study design and population
This study utilized data collected from the UK Biobank, a large-scale prospective study that recruited 502,400 adult participants between 2006 and 2010. The study amassed a wealth of demographic data and laboratory measurements while continually monitoring various health-related outcomes. Researchers can access de-identified data after signing a material transfer agreement, committing to use it solely for approved research and not attempting to identify any participants. After the exclusion of participants without accelerometer data, a total of 102,323 individuals were considered. Further excluding those with a prior history of T2DM, individuals (n = 99,532) without T2DM at baseline were incorporated into the final T2DM incidence risk analysis (Figure S6).
The present study protocol adhered to the ethical guidelines of the 1975 Declaration of Helsinki and approved by the ethics committee of Tianjin Chu Hsien-l Memorial Hospital. The study granted access to the UK Biobank database, which received ethical approval from the North West Multi-Centre Research Ethics Committee (21/NW/0157). All participants provided informed consent.
Accelerometer data and PA trajectories
To objectively measure PA, participants wore the Axivity AX3 wrist-worn triaxial accelerometer, capturing acceleration data continuously over 7 days at a frequency of 100Hz with a dynamic range of ± 8g. Participants wore the device uninterrupted, engaging in their typical activities. During a period of seven days, 24-h acceleration measurements provided real-time monitoring data that helped assess PA. Data processing was carried out by the UK Biobank (UKB) expert working group. The details of data processing were elaborately described in a previously published article40. The preliminary processed acceleration data, which was a movement metric (Euclidean norm minus one, ENMO) measured in milligravity (mg), served as a summary indicator of the body's acceleration (Figure S7). This metric reflected the instantaneous intensity of PA and was directly provided by the official UK Biobank, which constituted the raw data accessible for analysis in this study.
Evaluation of Type 2 diabetes
Type 2 diabetes was classified based on International Statistical Classification of Diseases, Tenth Revision (ICD-10) codes: E11. Also, according to the American Diabetes Association (ADA) criteria41, those with baseline glycated hemoglobin (HbA1c) levels ≥ 48 mmol/mol (6.5%) or random glucose levels ≥ 11.1 mmol/L were further excluded for sensitivity analysis. Follow-up for T2DM incidence continued until February 1, 2022.
Covariates
Factors such as age, gender, ethnicity, household income, smoking status, BMI, eGFR, CRP, and medical history were collected. Additional details regarding covariate measurements can be found in the UK Biobank online protocol (https://www.ukbiobank.ac.uk).
Statistical analysis
In order to identify potential PA trajectories, we employed the K-means algorithm by “sklearn.cluster” package in Python to perform cluster analysis using the average acceleration values for each of the 24-h periods across all measurement days, provided officially by the UK Biobank. Before conducting the cluster analysis, a Within-Cluster Sum of Squares (WSS) plot was created to determine the number of clusters to be considered in the K-means analysis (Figure S8).
All other analyses were conducted in R 4.2.2. Given the valuable nature of the continuous 24-h exercise data, multivariate imputation of the random forest method by “mice” package was used and only a small percentage of missing values for some covariates were imputed, maximizing data retention The distribution before and after imputation remained consistent, ensuring result reliability (see Table S4). Baseline demographic differences between the four trajectory groups (Table 1) were analysed. For normally distributed continuous variables, ANOVA was applied, for inappropriate distributions and categorical variable, the Kruskal–Wallis test and chi–square test were employed. Cox Proportional Hazards model was conducted by “survival” package. Proportional hazard assumptions were checked using Schoenfeld residuals and visually (Figure S9). Based on the identified trajectories from cluster analysis, we evaluate the association between PA patterns and T2DM risk. Three models were fitted to assess the effect of covariates. Model 1 adjusted for gender, age, and ethnicity. Model 2 further adjusted for education level, income, BMI, and smoking based on Model 1. Model 3 further adjusted for eGFR, CRP, and medical history of cardiovascular disease and cancer based on Model 2.
To ascertain result stability, sensitivity analyses were conducted: (1) further excluding individuals with HbA1c levels ≥ 48 mmol/mol (6.5%) or random glucose levels ≥ 11.1 mmol/L at baseline; (2) adopting Model 4, which adjusted for all-day average acceleration on top of all confounders adjusted in Model 3. Additionally, subgroup analyses were conducted based on gender, age, BMI, eGFR, CRP, and medical history of cardiovascular disease and cancer. Adequate analysis was performed to ensure the stability of the results. However, to address the issue of multiple testing, the Benjamini and Hochberg method was used to adjust the p-values and p-values after adjustment < 0.05 were considered significant.
Ethics approval and consent to participate
The study protocol adhered to the ethical guidelines of the 1975 Declaration of Helsinki and the UK Biobank obtained ethics approval from the North West Multi-Centre Research Ethics Committee (21/NW/0157). Informed consent was obtained from all individual participants included in the study.
Data availability
The data are available from the UK Biobank, but there are restrictions on their availability. These data were used under a license for the current study and are not publicly accessible. Researchers who wish to access the UK Biobank database will need to apply for access through the following link: https://www.ukbiobank.ac.uk/enable‑your‑research/.
References
Kolb, H. & Martin, S. Environmental/lifestyle factors in the pathogenesis and prevention of type 2 diabetes. BMC Med. 15, 131. https://doi.org/10.1186/s12916-017-0901-x (2017).
Boonpor, J., Ho, F. K., Gray, S. R. & Celis-Morales, C. A. Association of self-reported walking pace with type 2 diabetes incidence in the UK biobank prospective cohort study. Mayo Clin. Proc. 97, 1631–1640. https://doi.org/10.1016/j.mayocp.2022.02.028 (2022).
Ribeiro, A., Carvalho, J. P. R. & Bento-Torres, N. V. O. Physical exercise as treatment for adults with type 2 diabetes: A rapid review. Front. Endocrinol. 14, 1233906. https://doi.org/10.3389/fendo.2023.1233906 (2023).
Duncan, M. J., Arbour-Nicitopoulos, K., Subramaniapillai, M., Remington, G. & Faulkner, G. Revisiting the international physical activity questionnaire (IPAQ): Assessing sitting time among individuals with schizophrenia. Psychiatry Res. 271, 311–318. https://doi.org/10.1016/j.psychres.2018.11.063 (2019).
Castetbon, K. et al. Dietary intake, physical activity and nutritional status in adults: The French nutrition and health survey (ENNS, 2006–2007). Br. J. Nutr. 102, 733–743. https://doi.org/10.1017/s0007114509274745 (2009).
Blacher, E. et al. Aging disrupts circadian gene regulation and function in macrophages. Nat. Immunol. 23, 229–236. https://doi.org/10.1038/s41590-021-01083-0 (2022).
Costello, H. M. & Gumz, M. L. Circadian rhythm, clock genes, and hypertension: Recent advances in hypertension. Hypertension 78, 1185–1196. https://doi.org/10.1161/hypertensionaha.121.14519 (2021).
Shafi, A. A. & Knudsen, K. E. Cancer and the circadian clock. Cancer Res. 79, 3806–3814. https://doi.org/10.1158/0008-5472.Can-19-0566 (2019).
van der Velde, J. et al. Timing of physical activity in relation to liver fat content and insulin resistance. Diabetologia 66, 461–471. https://doi.org/10.1007/s00125-022-05813-3 (2023).
Rowlands, A. V. et al. Association of timing and balance of physical activity and rest/sleep with risk of COVID-19: A UK biobank study. Mayo Clin. Proc. 96, 156–164. https://doi.org/10.1016/j.mayocp.2020.10.032 (2021).
Rea, M. S., Bierman, A., Figueiro, M. G. & Bullough, J. D. A new approach to understanding the impact of circadian disruption on human health. J. Circadian Rhyth. 6, 7. https://doi.org/10.1186/1740-3391-6-7 (2008).
Feng, H. et al. Associations of timing of physical activity with all-cause and cause-specific mortality in a prospective cohort study. Nat. Commun. 14, 930. https://doi.org/10.1038/s41467-023-36546-5 (2023).
Althoff, T. et al. Large-scale physical activity data reveal worldwide activity inequality. Nature 547, 336–339. https://doi.org/10.1038/nature23018 (2017).
Kelly, S. P. et al. Prediagnostic body mass index trajectories in relation to prostate cancer incidence and mortality in the PLCO cancer screening trial. J. Natl. Cancer Inst. https://doi.org/10.1093/jnci/djw225 (2017).
Oluwagbemigun, K. et al. Developmental trajectories of body mass index from childhood into late adolescence and subsequent late adolescence-young adulthood cardiometabolic risk markers. Cardiovascul. Diabetol. 18, 9. https://doi.org/10.1186/s12933-019-0813-5 (2019).
Petrick, J. L. et al. Body weight trajectories and risk of oesophageal and gastric cardia adenocarcinomas: A pooled analysis of NIH-AARP and PLCO Studies. Br. J. Cancer 116, 951–959. https://doi.org/10.1038/bjc.2017.29 (2017).
Watts, E. L. et al. Association of leisure time physical activity types and risks of all-cause, cardiovascular, and cancer mortality among older adults. JAMA Netw. Open 5, e2228510. https://doi.org/10.1001/jamanetworkopen.2022.28510 (2022).
Gilson, N. et al. Postpandemic hybrid work: Opportunities and challenges for physical activity and public health. Br. J. Sports Med. 56, 1203–1204. https://doi.org/10.1136/bjsports-2022-105664 (2022).
Trenell, M. I. Sedentary behaviour, physical activity, and NAFLD: Curse of the chair. J. Hepatol. 63, 1064–1065. https://doi.org/10.1016/j.jhep.2015.08.009 (2015).
Guthold, R., Stevens, G. A., Riley, L. M. & Bull, F. C. Worldwide trends in insufficient physical activity from 2001 to 2016: A pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Global Health 6, e1077–e1086. https://doi.org/10.1016/s2214-109x(18)30357-7 (2018).
Balducci, S. et al. Relationships of changes in physical activity and sedentary behavior with changes in physical fitness and cardiometabolic risk profile in individuals with type 2 diabetes: The Italian Diabetes and Exercise Study 2 (IDES_2). Diabetes Care 45, 213–221. https://doi.org/10.2337/dc21-1505 (2022).
Patterson, R. et al. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: A systematic review and dose response meta-analysis. Eur. J. Epidemiol. 33, 811–829. https://doi.org/10.1007/s10654-018-0380-1 (2018).
Zheng, Y., Ley, S. H. & Hu, F. B. Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Nat. Rev. Endocrinol. 14, 88–98. https://doi.org/10.1038/nrendo.2017.151 (2018).
Kim, H. K. et al. Late-afternoon endurance exercise is more effective than morning endurance exercise at improving 24-h glucose and blood lipid levels. Front. Endocrinol. 13, 957239. https://doi.org/10.3389/fendo.2022.957239 (2022).
Galan-Lopez, P. & Casuso, R. A. Metabolic adaptations to morning versus afternoon training: A systematic review and meta-analysis. Sports Med. 53, 1951–1961. https://doi.org/10.1007/s40279-023-01879-0 (2023).
Albalak, G. et al. Timing of objectively-collected physical activity in relation to body weight and metabolic health in sedentary older people: A cross-sectional and prospective analysis. Int. J. Obesity 2005(46), 515–522. https://doi.org/10.1038/s41366-021-01018-7 (2022).
Sudlow, C. et al. UK biobank: An open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 12, e1001779. https://doi.org/10.1371/journal.pmed.1001779 (2015).
Savikj, M. et al. Afternoon exercise is more efficacious than morning exercise at improving blood glucose levels in individuals with type 2 diabetes: A randomised crossover trial. Diabetologia 62, 233–237. https://doi.org/10.1007/s00125-018-4767-z (2019).
Brito, L. C. et al. Comparison of morning versus evening aerobic-exercise training on heart rate recovery in treated hypertensive men: A randomized controlled trial. Blood Press. Monit. 26, 388–392. https://doi.org/10.1097/mbp.0000000000000545 (2021).
Homer, A. R. et al. Regular activity breaks combined with physical activity improve postprandial plasma triglyceride, nonesterified fatty acid, and insulin responses in healthy, normal weight adults: A randomized crossover trial. J. Clin. Lipidol. 11, 1268-1279.e1261. https://doi.org/10.1016/j.jacl.2017.06.007 (2017).
Muralidharan, J. et al. Effect on gut microbiota of a 1-y lifestyle intervention with Mediterranean diet compared with energy-reduced Mediterranean diet and physical activity promotion: PREDIMED-Plus Study. Am. J. Clin. Nutrit. 114, 1148–1158. https://doi.org/10.1093/ajcn/nqab150 (2021).
Jones, P. J. & Schoeller, D. A. Evidence for diurnal periodicity in human cholesterol synthesis. J. Lipid Res. 31, 667–673 (1990).
Saito, Y., Yoshida, S., Nakaya, N., Hata, Y. & Goto, Y. Comparison between morning and evening doses of simvastatin in hyperlipidemic subjects A double-blind comparative study. Arterioscler. Thromb. A J. Vascul. Biol. 11, 816–826. https://doi.org/10.1161/01.atv.11.4.816 (1991).
Stea, T. H., Wandel, M., Mansoor, M. A., Uglem, S. & Frølich, W. BMI, lipid profile, physical fitness and smoking habits of young male adults and the association with parental education. Eur. J. Public Health 19, 46–51. https://doi.org/10.1093/eurpub/ckn122 (2009).
Spoto, B., Pisano, A. & Zoccali, C. Insulin resistance in chronic kidney disease: A systematic review. Am. J. Physiol. Renal Physiol. 311, F1087-f1108. https://doi.org/10.1152/ajprenal.00340.2016 (2016).
Yan, M. T., Chao, C. T. & Lin, S. H. Chronic kidney disease: Strategies to retard progression. Int. J. Mole. Sci. https://doi.org/10.3390/ijms221810084 (2021).
Lai, S. et al. Vitamin D deficiency, insulin resistance, and ventricular hypertrophy in the early stages of chronic kidney disease. Renal Failure 36, 58–64. https://doi.org/10.3109/0886022x.2013.832308 (2014).
White, T. et al. Estimating energy expenditure from wrist and thigh accelerometry in free-living adults: A doubly labelled water study. Int. J. Obes. 2005(43), 2333–2342. https://doi.org/10.1038/s41366-019-0352-x (2019).
Ramakrishnan, R. et al. Accelerometer measured physical activity and the incidence of cardiovascular disease: Evidence from the UK Biobank cohort study. PLoS Med. 18, e1003487. https://doi.org/10.1371/journal.pmed.1003487 (2021).
van Hees, V. T. et al. Separating movement and gravity components in an acceleration signal and implications for the assessment of human daily physical activity. PloS One 8, e61691. https://doi.org/10.1371/journal.pone.0061691 (2013).
Classification and Diagnosis of Diabetes. Standards of medical care in diabetes-2022. Diabetes Care 45, S17-s38. https://doi.org/10.2337/dc22-S002 (2022).
Acknowledgements
The authors thank the staff and participants of the study for their indispensable contributions.
Funding
This study was funded by "Tianjin Medical Talents" project, the second batch of high-level talents selection project in health industry in Tianjin, no. TJSJMYXYC-D2-014. Key Project of Natural Science Foundation of Tianjin, no. 22JCZDJC00590.Scientific Research Funding of Tianjin Medical University Chu Hsien-I Memorial Hospital, no. ZXY-ZDSYSZD-1.Tianjin Science and Technology Major Special Project and Engineering Public Health Science and Technology Major Special Project, no. 21ZXGWSY00100.Tianjin Key Medical Discipline (Specialty) Construct Project no. TJYXZDXK-032A. The funder was not for profit.
Author information
Authors and Affiliations
Contributions
P.B.: Data curation, Formal Analysis, Visualization, Writing—original draft. X.S.: Validation, Writing—original draft. L.C.: Investigation, Resources. S.Z.: Funding acquisition, Writing—review & editing. Y.L.: Investigation, Resources. HL: Investigation. P.Y.: Project administration, Funding acquisition, Resources, Supervision, Writing—review & editing. All authors of this paper have read and approved the final version submitted.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bai, P., Shao, X., Chen, L. et al. Association between circadian physical activity trajectories and incident type 2 diabetes in the UK Biobank. Sci Rep 14, 6459 (2024). https://doi.org/10.1038/s41598-024-57082-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-57082-2
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
