
Abstract
Falls represent a huge health and economic burden. Whilst many factors are associated with fall risk (e.g. obesity and physical inactivity) there is limited evidence for the causal role of these risk factors. Here, we used hospital and general practitioner records in UK Biobank, deriving a balance specific fall phenotype in 20,789 cases and 180,658 controls, performed a Genome Wide Association Study (GWAS) and used Mendelian Randomisation (MR) to test causal pathways. GWAS indicated a small but significant SNP-based heritability (4.4%), identifying one variant (rs429358) in APOE at genome-wide significance (P < 5e-8). MR provided evidence for a causal role of higher BMI on higher fall risk even in the absence of adverse metabolic consequences. Depression and neuroticism predicted higher risk of falling, whilst higher hand grip strength and physical activity were protective. Our findings suggest promoting lower BMI, higher physical activity as well as psychological health is likely to reduce falls.
Similar content being viewed by others

Humans utilise visual, proprioceptive and vestibular systems to stand upright and maintain balance1,2. These systems are critical for human function, with loss of balance and disorders of the balance system (e.g. vestibular disorders) increasing an individual’s risk of falls. Falls and fall related fractures represent a huge health and economic burden, with strong associations with increased morbidity, mortality and disability3,4. Determining factors that predict falls is challenging as they can be both intrinsic and extrinsic5 and the available evidence in this field remains limited, with the majority of studies focusing on older individuals.
Previous observational studies and several systematic reviews3,6,7,8,9,10 have highlighted the importance of a range of traits including adiposity, physical activity, previous falls, gait problems, vertigo, visual impairment, fear of falling, cognitive impairments and mental health problems in predicting falls. However, the majority of studies have focused on older individuals (60 years +) and not used methods that enable causal inference. Therefore, the results are not generalisable to the wider population and may be subject to confounding and reverse causality11,12. Understanding factors that cause falls is important, particularly when considering the possibility of modifiable risk factors that could potentially be targeted for prevention or intervention strategies.
A previous study by Trajanoska et al.13, performed a genome wide association study (GWAS) of self-reported falls using data from the UK Biobank. They demonstrated that despite the heterogeneity of factors contributing to fall risk, genetics was found to play a role, accounting for 2.7% of the overall susceptibility to falls. This study also showed positive genetic correlations between self-reported falls and fractures, insomnia, neuroticism, depressive symptoms and body mass index (BMI), as well as inverse correlations with muscle strength and intelligence. The falls measure used was a very broad, self-reported metric and as a result captured a wide variety of falls including falls related to accidents and falls not specific to balance issues.
Ideally, evidence of causal effects comes from well conducted randomised control trials (RCTs). However large-scale RCTs cannot always be performed because they can be costly, impractical, or even unethical14. One of the alternatives is to perform MR analyses that are similar to RCTs in terms of study design. MR (Fig. 1) uses genetic variation as a natural experiment to investigate the causal relations between potentially modifiable risk factors and health outcomes in observational data14.

Directed acyclic graph (DAG) showing the relationship between the instrumental variables (IV), exposure, confounders and outcome. The IV must not have a direct effect on the outcome or the confounders for the assumptions of MR to be withheld. The IV may only act through the exposure. (A) describes the association between the exposure (X) of interest and genetic variants (Z) in the genome. (B) describes the observational.
A previous MR study provided evidence that higher BMI causes higher risk of falling and stronger hand grip reduces fall risk13. However, this study used a broad, self-reported, metric for falls and there are still many unanswered questions regarding the potential factors that have been suggested to contribute to the occurrence of falls13. For example, there is conflicting observational evidence for a role of mental health including depression, anxiety and neuroticism in fall risk15,16. There is observational evidence suggesting adverse mental health raises fall risk. However, clinical interventions aimed at reducing falls via mental health treatment has not proved successful16,17.
In this study, we aimed to utilise hospital and primary care records from the UK Biobank to define a binary balance related falls outcome. With this metric, our objective is to conduct a GWAS to explore genetic correlations. Additionally, we will employ multiple MR methods to assess potential causal relationships between a variety of predictors. These predictors have been selected based on prior literature and will be examined in relation to our falls metric.
Methods
The UK Biobank
The UK Biobank is a health resource with extensive phenotypic and genetic data available for over 500,000 individuals, who were aged between 37 and 73 at recruitment (from 2006 to 2010). Full details of this study are available18,19. Genome-wide genetic data was available for all participants, with approximately 850,000 variants directly measured using the UK Biobank Axiom (~ 450,000 individuals) or the UK BiLEVE (~ 50,000 individuals) array. These were then imputed using the UK10K and 1000 genome reference panels. Extensive quality control was carried out by UK Biobank, as previously described19. We defined ancestry using principal components in the 1000 Genomes Cohort as previously described20. We included up to 451,036 UK Biobank participants genetically similar to the 1000 Genome European superancestry group which included 209,298 participants with data linked to GP codes. Genetic similarity was derived using principal component analysis using the 1000 Genomes Cohort as our reference, as previously described20.
Exposure and outcome measures
Exposures
Potential exposures were considered if there was a) prior evidence in the scientific literature of an association with falling and b) known genetic variants associated with the exposure for use in MR (see Genetic Analysis section). Briefly, the exposures fit into three categories: body mass (BMI and adiposity), physical activity (hand grip max strength, measured physical activity and sedentary time) and mental health (depression, anxiety and neuroticism). A full list of the exposures considered in this study is available in Table 1. For adiposity, we included genetically defined favourable and unfavourable adiposity (FA and UFA respectively). FA variants are associated with higher BMI and body fat, but lower risk of heart disease, diabetes and dyslipidaemia. In contrast UFA, is associated with higher fat and poorer metabolic profile21. These variants will allow us to test if it solely something about being fatter that increases falls risk or whether this is driven by poorer metabolic health22.
Outcomes
We derived a binary fall outcome metric using the hospital episode statistics (HES) and general practitioner (GP) records available in the UK Biobank23. First, we extracted 137 ICD-10 codes and 84 GP read2/read3 codes (Supplementary Table 1). We then reviewed these codes with a Consultant Otolaryngologist Hilton M) and removed fall codes that were unlikely to be related to balance issues (e.g. codes relating to diving or falling into water; Supplementary Table 1). The HES data included falls reported between 1995 and 2021 (mean age of falling = 69.8 years) and the GP data included falls reported between 1955 and 2017 (mean age of falling 61.2 years). For completeness, we also tallied the number of falls for each individual that had at least one fall code in their records. Any occurrences that occurred on the same date but were reported using a different code were counted as one fall rather than multiple falls.
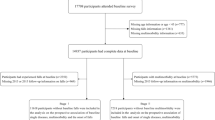
We defined controls as individuals with a HES or GP record and no recorded code relating to falls (including all fall codes; Supplementary Table 1). Our main analyses focused on the combined falls metric derived using both the HES and GP records, with 20,789 individuals reporting a balance related fall and 180,658 controls. We also repeated our analyses using a GP only derived metric (11,654 falls and 197,644 controls) and our HES only derived metric (23,236 falls and 408,650 controls) to test if the HES and GP records capture different types of falls. Finally, we derived a count of falls in the 20,789 reporting at least one fall.
During the baseline interview, all participants of the UK Biobank were asked to self-report falls within the last year. Although we did not use this metric to derive our balance related falls phenotype, we did check the overlap of cases with our metrics. Among our cases, 6447 individuals (31%) also reported a fall in the self-report data, while only 195 individuals (0.001%) among our controls reported a self-reported fall.
Statistical analyses
Observational associations
To test the association of a range of exposures with our binary falls metric we used logistic regression adjusting for age at UK Biobank baseline assessment and sex. To test if factors that predicted our binary falls metric also predicted number of falls, we used a Poisson model.
Genome-wide association analysis
Association analyses used imputed genotypes available from the UK Biobank24. Variants were excluded if imputation quality (INFO) was < 0.3 or the minor allele frequency (MAF) was < 0.1%. All individual variant association testing was performed using REGENIE (Version 2)25. This method accounts for population structure and employs a Firth logistic regression to account for unbalanced case–control phenotypes, such as our falls phenotype. A number of covariates were included at runtime: age, sex, UK Biobank assessment centre and genotyping platform (categorical UKBiLEVE array, UKB Axiom array interim release and UKB Axiom array full release).
Genetic correlations
We used linkage disequilibrium (LD) score regression26 to quantify the genetic overlap between a) our fall phenotype and b) 12 traits of interest with 3 publicly available GWASs and 7 internally run GWASs. This method uses the GWAS summary statistics from two GWASs and regresses them against a measure of how much variation each single nucleotide polymorphism SNP tags (its LD score). Correlations were reported if they reached a Bonferroni corrected P value (number of tests = 12; p < 0.0042).
Mendelian randomisation (MR)
We undertook MR analyses to further test the causal relationships between the 13 exposure traits (decided a priori on the grounds that they are common exposures with observational evidence of an association). Where possible we also tested the bidirectional association, with falls as the exposure. We performed several different types of MR analyses to account for data availability and various statistical biases in our models. Results are presented from the most appropriate method for each exposure (Table 1) but generally results were consistent across the different methodologies. The different MR methods are summarised below:
One-sample MR
We performed one sample MR analyses at the individual level within up to 430,944 unrelated UKB participants. The effects of grip strength, alcohol consumption, BMI and depression (defined using the Composite International Diagnostic Interview (CIDI) and the Patient Health Questionnaire (PHQ-9)) on falls were estimated with the two-stage least squares11 approach and observational associations were reported for reference. In these analyses we also considered our fall count metric as an outcome.
In all analyses, the exposure phenotypes were regressed on the genetic instruments and the predicted values were then used in the second stage to obtain the unconfounded estimate of the exposures’ causal effects. Where possible, no or minimal overlap of the gene selection study with UKB was preferred. However, this was not always possible (e.g. hand grip exposure also included UKB), in these cases MR Lap (see below) was also performed to account for sample overlap. We considered three options for the second stage of MR, based on the nature of the distribution of the falls phenotype. For our primary binary outcome logistic models were used. For the falls count metric, we utilised either a linear model or a Poisson model. It was anticipated that the latter approach would be the most appropriate as the falls count metric generally follows a Poisson distribution.
Two sample MR
The two-sample MR analyses used summary-level data from the REGENIE GWAS of the falls traits. Known SNPs for each exposure were extracted from the falls GWAS results, representing the association of the outcome and exposure-trait-SNP, whilst published coefficients from the primary GWAS represent the exposure association with the exposure-trait-SNP. Using a custom pipeline, we performed four two-sample MR methods: inverse-variance weighting (IVW); MR-Egger27; weighted median (WM); penalised weighted median (PWM)28. For the two-sample analyses the IVW approach represents our main analyses, with MR-Egger, WM and PWM used as sensitivity analyses to account for unidentified pleiotropy that could bias our results29.
MR lap
Several of our exposures included UK Biobank in the primary GWAS (Table 6) This can induce bias to MR analyses and contribute to Winner’s curse. To account for this, we utilised MRLap (https://github.com/n-mounier/MRlap)30. MRLap is designed to correct for weak instrument bias and winner’s curse, whilst also accounting for sample overlap. MRLap provides observed (uncorrected) and corrected IVW results and quantifies the difference between the observed and corrected effects. Detailed information about the method and its approach to adjusting for biases can be found in Mounier et al. Analyses performed with MRLap are summarised in Table 6. In addition, we tested the bidirectional relationship between falls and our exposures using this method (F Statistic = 21.7).
In both the two-sample MR and MR Lap where we had a binary exposure with summary statistics based on a log odds ratio (ln(OR)), our effect estimates represent a change in fall risk per change in the binary exposure on a log odds scale. Therefore for interpretation we calculated the odds of falling per doubling in the genetic risk for the binary predictor by multiplying the causal estimate by 0.693 (= ln2)31.
Sensitivity analysis in the MR framework
Sex-stratified MR to eliminate pleiotropy
In the one sample setting we also employed a novel approach to eliminate pleiotropy, which exploits sex specific associations32The genetic associations for grip strength are known to differ substantially between men and women based on previous evidence33 The instrument selection involved identifying SNPs that are stronger for one sex (gene-sex interaction), subtracting them, and extracting these from sex-specific falls GWAS.
Alcohol and smoking analyses
Alcohol and smoking univariable analyses were also performed in several subgroups of individuals, stratified by either alcohol drinking status (never versus ever) and smoking status (never, former and current). In never drinkers and never smokers we would not expect to see any association of our alcohol or smoking genetic instrument respectively.
All analyses were performed in R version 4.1.2.
Results
Demographics of the falls cases and controls can be found in Table 2. Briefly, individuals with a recorded fall were older, more likely to be female, have a higher BMI and lower maximum hand grip strength. Individuals reporting falls were also more likely to have a lower educational attainment and were more likely to report having depression and anxiety.
Of the 20,789 of individuals with a known fall, 6444 (31%) had more than one fall (range 2–59; Supplementary Fig. 1). Individuals reporting more falls were older, more likely to be female, have a higher BMI, a lower hand grip strength and spend less time doing physical activity. They were also more likely to have a lower educational attainment and more likely to report depression and anxiety (Table 3).
Observational evidence provided further evidence our exposures were associated with balance related falls
Observationally, several exposures were robustly associated with having a fall in UKB (Fig. 2; Table 3). For example, a one standard deviation (SD) higher BMI (4.8 kg/m2) was associated with 1.17 higher odds of falling (95% CI: 1.15, 1.19). In contrast a 1 SD higher hand grip strength (11.34 kg) was associated with 0.69 lower odds of falling (95% CI: 0.67, 0.70).

Forest plot representing the observational odds of falling for three main exposure groups: body mass, physical activity and mental health metrics. (IPAQ: International Physical Activity Questionnaire) (> 40 & > 100 mg PA: The sum of all actigraphy measures greater than or equal to 40 and 100 milli-gravity respectively).
There was also observational evidence for a role of mental health in fall risk. Both depression status and severity associated with higher risk of falling. For example, depression status was associated with 1.35 higher odds of falling (95%CI: 1.29,1.42) and a one unit higher severity of depression was associated with 1.06 higher odds of a fall (95%CI: 1.05,1.07). Anxiety was also associated with higher fall risk (OR:1.68, 95% CI: 1.55,1.80), as was higher anxiety severity (OR: 1.05, 95%CI: 1.04,1.05).
Observationally higher physical activity (measured using self-report and accelerometery data) was associated with a lower risk of falling. A 1-SD higher moderate to vigorous physical activity (MVPA) and + 40milligravitiy activity (40 mg) was associated with 0.78 (95% CI:0.76, 0.83) and 0.82 (95% CI:0.79, 0.86) lower odds of a fall respectively. Furthermore, a 1-SD higher score (1.14) on the self-reported international physical activity questionnaire (IPAQ) score was associated with 0.94 (95% CI: 0.92, 0.95) lower odds of a fall.
Observational results were generally similar for HES only and GP only derived falls (Supplementary Table 2).
GWAS of the balance falls metric identified one loci in the APOE gene
The genetic heritability of combined falls was 4.4% (2.8% for HES falls and 3.8% for GP falls). One locus was identified at genome wide significance (GWS; p < 5e−08) in our main analyses (Table 4). This mapped to the APOE gene, where rs429358 is a missense mutation, with the C-allele of the APOE-ε4 genotype being a major risk factor for Alzheimer’s disease. Here, the C-allele also predicts a higher likelihood of falling. This variant has been identified in many GWAS studies including plasma levels34, LDL-cholesterol35, superior frontal cortical thickness36, Alzheimer’s disease37 and longevity38.
When stratifying our analyses by age the lead SNP, rs429358, was associated with higher odds of a fall per risk increasing allele higher in both those over 65 (OR: 1.15; 95% CI:1.09, 1.20) and those 65 or under (OR: 1.05; 95% CI: 1.02, 1.09).
When looking at HES and GP falls alone, the APOE locus reached GWS in the HES derived fall metric, but not in the GP derived metric (p = 0.013). An additional GWS locus was identified in the HES alone fall phenotype, with variant rs2908008 in Chr 7 (Table 4). This variant is near the WNT16 gene which has previously been associated with heel bone mineral density39 and is the top locus in the most recent falls GWAS data from FINNGEN (https://r9.finngen.fi).
There was no evidence of an association between the two previously published GWAS hits from the self-reported falls GWAS13 (p > 0.08; Table 5).
Genetic correlations
After Bonferroni correction (p < 4.17E-03) we observed strong positive genetic correlations between the combined falls and the HES falls (rg: 0.86, p: 2.19e−27) and GP falls (rg: 0.99, p: 1.37e−51) data (Table 5). Similarly, a positive correlation was observed between HES falls and GP falls (rg: 0.7481, p: 6.75e−06) (Table 5). Our balance fall metric was also genetically correlated with the previously published self-reported falls GWAS (Table 5; rg: 0.70, p: 7.42e−17)13.
After Bonferroni correction the falls metric was positively genetically correlated with BMI, WHR, depression, neuroticism, Townsend Deprivation Index and cigarettes per day (Table 5). In contrast, negative genetic correlations were noted with hand grip strength, bone mineral density and years in education (Table 5). There was no evidence for a genetic correlation between falls and a) Alzheimer’s disease and b) anxiety (Table 5). The genetic correlations were repeated using the HES and GP derived falls metrics and were consistent (Supplementary Table 3).
Mendelian Randomisation (MR)
MR provided further evidence for a role of higher BMI in fall risk and evidence this is not solely due to poorer metabolic health
There was evidence from both one and two sample MR that higher BMI is causally associated with falling (Fig. 3a). For example, a 1-SD higher (4.5 kg) genetically instrumented BMI was associated with 1.26 higher odds of falling (95%CI: 1.12, 1.42). Whilst the more pleiotropy robust methods had wider uncertainty around the estimate, the associations were directionally consistent and there was no evidence of horizontal pleiotropy (p = 0.61; Table 6).

(a) Forest plot of 2-Sample MR results showing adiposity as the exposure and binary falls as the outcome. (b) Forest plot of MRLap results showing Physical Activity Phenotypes as the exposure and binary falls as the outcome. (c) Forest plot of MRLap results showing Mental Health Phenotypes as the exposure and binary falls as the outcome. (d) Forest plot of MRLap testing Bidirectional effect of Falls on metrics of interest. Binary Falls is treated as the exposure.
Genetic variants that make an individual fatter but metabolically healthier (e.g. lower risk of type 2 diabetes, lower risk of cardiovascular disease), termed favourable adiposity, were associated with higher risk of falling (OR: 1.39; 95% CI: 1.09, 1.69). Similarly, there was evidence that genetic variants associated with higher unfavourable adiposity (i.e. higher body fat percentage, high risk of type 2 diabetes etc.) also predicted falling (OR: 1.48; 95% CI: 1.28, 1.67) (Table 6).
MR provided evidence that longer educational duration is protective from falls
Using MR Lap to account for the exposure and outcome data both coming from the UK Biobank we provide evidence that a longer educational duration is protective for fall risk. For example, a genetically instrumented one year longer educational duration associated with 0.93 lower odds of falling (95%CI: 0.90, 0.95). Results were similar using standard 2-sample MR and a smaller set of variants that excluded UK Biobank (Table 6).
Higher physical strength and activity protect from fall risk
There was evidence after accounting for sample overlap that higher hand grip strength was protective from falling. A 1-SD higher genetically instrumented hand grip (~ 11.3 kg) was associated with 0.95 lower odds of falling (95% CI: 0.92, 0.97; Table 6, Fig. 3b). There was no evidence of bias from overlapping samples (P = 0.27). A higher genetic liability to falling did not predict hand grip) (Table 6).
A higher genetically instrumented overall physical activity was nominally associated with lower risk of falling (OR: 0.96; 95%CI: 0.93, 1.00; p = 0.038). MRLap did not provide evidence that the overlapping samples or weak instrument biased the results. There was no evidence of a bidirectional association between PA and falls (p = 0.90; Table 6).
Higher genetically instrumented actigraphy measured sedentary time was not associated with fall risk (OR: 1.08 95%CI: 0.97, 1.20) and there was no evidence that a genetically higher fall risk predicted sedentary time (p = 0.45).
Major depression and neuroticism predict falling but no evidence for a role of generalised anxiety
MR-Lap provided evidence that major depression, with the most up to date Psychiatric Genomics Consortium (PGC) summary statistics40 predicted falling (Fig. 3c). A twofold higher genetic liability to major depression was associated with 1.15 higher odds of an individual falling (95% CI: 1.04, 1.26). There was some evidence that sample overlap biased our results and therefore the corrected effects are presented (corrected difference p-value = 0.003) (Table 6. There was no evidence for a bidirectional relationship between depression and falls (Table 6; Fig. 3d).
There was evidence that neuroticism was causally associated with falling. A one SD higher genetic neuroticism (~ 3.27 units) associated with 1.08 higher odds of falling (95% CI: 1.04, 1.12). The estimates obtained with MR Lap correction were similar to the uncorrected estimates. A higher genetic liability to falling did not associate with neuroticism. There was no evidence that a higher genetic liability to generalised anxiety predicting falling or vice versa (Table 6).
Sensitivity analyses
One-Sample MR
To further test causal pathways, we also performed some univariate one-sample MR using both the binary falls metric and the count of falls in our 20,789 falls cases (Supplementary Table 8). These models indicate that alcohol, BMI and all depression measures (major depression, major depression severity and current depression) are positively causally associated with falls, whereas grip strength seems to exert a protective effect (Fig. 4). The Poisson modelling approach provides point estimates that are numerically similar to the binomial distribution of the dichotomous falls phenotype, but all are more precise (confidence intervals for the Poisson model are on average 11.51% narrower than those of the logistic regression). Therefore, the second-stage Poisson distribution seems to improve power as it retains the information regarding the number of falls. In summary, alcohol, BMI, depression measures, and grip strength appeared to influence the binary falls metric and the count of falls, with effect sizes of similar magnitude to the ones reported above.

Forest Plot for the effects of alcohol, BMI, CIDI, CRP, ever depressed status, grip strength, and PHQ9 on falls. Univariable MR. Three different modelling choices for the outcome of falls are presented (linear for normal distribution, logistic regression for binomial distribution, and Poisson distribution), The respective observational associations are presented.
Sex stratified MR
In the sex-stratified MR32, a total of 185 SNPs surpassed the F statistic threshold of 15 and were used as sex-specific instruments. There seems to be a protective causal effect of grip strength on risk of falls (RR: 0.74, 95% CI: 0.61, 0.91 p: 0.004).
GP only and HES only falls MR
MR analyses were repeated using the GP and HES only derived fall phenotypes. Generally, the results were consistent (Supplementary Fig. 6). Increased sedentary time was associated with an increased risk of falls in the GP derived metric in contrast to the results of the combined and HES fall metrics. Physical Activity was found to be non-significant in the GP metric (OR:0.993; 95%CI:0.959,1.027) but significant in the combined (OR: 0.965; 95%CI: 0.930, 0.999) and HES (OR 0.973; 95%CI: 0.949, 0.997) metrics.
Discussion
This study explored the genetic basis of a balance related fall phenotype derived from electronic health records. We provide further evidence that falls are a highly heterogenous polygenic trait with a small but significant SNP-based heritability (4.4%) and identified one locus in the APOE gene in GWAS. The study also used MR to test the causal role of a broad range of modifiable risk factors on falling, highlighting the importance of adiposity, depression and neuroticism in predicting falls, whilst improved physical functioning as defined by hand grip strength and physical activity protected from falls.
The GWAS signal identified in this study is a missense mutation in APOE gene (rs429358)41. The C-allele is the marker of the APOE-ε4 genotype which is a major risk factor for Alzheimer’s disease42, and here, was associated with higher odds of falling. This is a highly pleiotropic locus, which also associates with heart disease43, inflammation44 and dyslipidaemia45. Poorer health and frailty may explain the association with falling. A sensitivity analysis stratifying the association of the top hit by age (> 65 and ≤ 65) demonstrated that whilst the association was stronger in the older age group, an increased risk of falling remained in those under 65 (Supplementary Table 5).
The GWAS results for our balance related falls metric were correlated with the previous self-reported falls GWAS, however the variants previously identified by Trajanoska et al., were not associated with our falls metric (Table 5). These differences in findings may be explained by the different definitions of falling. Here, we used hospital and GP health records to code falls and restricted the falls codes to those that represent balance related falls. In contrast, the Trajanoska et al. used a self-reported fall metric, derived from positive responses to the question: “In the last year have you had any falls?” Methods of specifically identifying balance related falls, such as those used in the present study, are likely to capture more severe falls phenotypes, related to mechanisms of balance problems.
Genetic correlations provided evidence that risk of falling was positively correlated with BMI, WHR, depression and neuroticism, and negatively correlated with hand grip strength and bone mineral density. In these analyses there was no evidence of a genetic correlation between falling and physical activity, anxiety or Alzheimer’s disease. The correlation between falls, BMI hand grip strength is consistent with Trajanoska et al. However, our analysis also shows evidence of fall risk being genetically associated with lower bone mineral density in contrast to the findings of Trajanoska et al. which found no significant association.
Higher BMI was identified by MR as a risk factor for falling. This fits with evidence from several observational studies46,47 and the previous self-reported falls genetic study13. The relationship between BMI and falling may be explained by poorer health in those with a higher BMI and/or alterations to balance control48,49. More research is needed in this area as UK Biobank lacks power for analyses at lower BMIs. To gain further insight into the potential mechanisms by which higher BMI increases falls risk we used favourable and unfavourable adiposity genetic variants50, to instrument higher body fat percentage in the presence (unfavourable) and absence (favourable) of adverse metabolic consequences (i.e. type 2 diabetes, cardiovascular disease, dyslipidaemia). Both sets of genetic variants were associated with higher falls risk. This indicates that it is not solely the adverse metabolic health consequences of higher BMI driving the association, perhaps indicating the importance of BMI in balance control51,52.
Higher hand grip strength and physical activity were protective for falling. As previously noted by Trajanoska et al., lower hand grip was noted to increase the risk of falling. Here, we used novel MR methods that use sex stratified estimates to account for pleiotropy, providing further evidence for the protective role of hand grip on falls risk. Using MR approaches that account for weak instruments and sample overlap between the exposure and outcome summary statistics we provide evidence for a causal role in physical activity in reducing balance related falls risk which is consistent with previous work summarised in a systematic review of 8 studies investigating the use of physical activity programmes to increase balance performance and decrease fall risk53. This provides consistent evidence of the importance of muscle weakness as a risk factor for balance related falls and further highlights the benefits of remaining physically active throughout adult life.
We demonstrate that a higher genetic liability to depression increases an individual’s risk of falling. This fits with previous evidence54, including data from a meta-analysis of 17 prospective studies where depression was associated with falls55. There was no evidence that a higher genetic liability to falling predicted depression, but these analyses were limited by lower power. A higher genetic liability to neuroticism was also predictive of falls, adding to the observational evidence that neuroticism associates with falls56. Although it is still unclear as to whether the association between neuroticism and falls is mediated by depression as suggested by Turunen et al. or acts independently. Future work, should investigate the potential mediate effect of depression on neuroticism and falls, using multi-variable MR (MVMR) to determine if the association between neuroticism and falls is independent of depression.
Our results suggest that there is no evidence of a genetic correlation or a causal link between anxiety and risk of falling. This is in contrast to a recent meta-analysis of 18 studies which concluded that anxiety was positively associated with falls57. This may be partially explained by potential confounders such as fear of falling (FoF) and neuroticism driving the observed association between anxiety and falls. The literature surrounding FoF is sparce with measures of FoF such as the Falls Efficacy Scale International (FESI) lacking depth58 and studies generally focusing on older populations with specific conditions such as Parkinson’s57.
A recent qualitative study59 explored anxiety and FoF using semi-structured interviews. This study highlighted that the effect of FoF on fall risk is contextual and depends on an individual’s perception of control. Should one be worried about falling but this, in turn, increases their perception of potential risks and their own limitations then it acts protectively. However, should one have FoF, and this distracts the individual from their surroundings and potential risks then this is detrimental. This may explain the high heterogeneity (I2 = 71%) in the meta-analysis of the effects of anxiety on falls57 as well as the lack of causal evidence we see in this study. It should also be noted that rs429358, our lead hit, was associated with a lower odds of participation in the mental health questionnaires60 which may further bias the anxiety results towards the null.
This study has a number of strengths. It uses a refined balance falls metric in a large sample of individuals in the UK Biobank, rather than self-reported falls in the past year, which may be more reflective of health status over the last 12 months. However, we acknowledge that there are limitations using this derivation method. We were unable to capture falls that did not require a GP visit or hospital admission including visits to Accident and Emergency.
UK Biobank is not population representative, with a healthy volunteer bias61 and our analyses was restricted to those of European ancestry. Our analyses with actigraphy derived physical activity are susceptible to participation bias60. For example, individuals with actigraphy data had a fall prevalence of 7.7% compared to 10% in individuals without actigraphy data.
There are also inherent limitations of using binary outcome measures in MR analyses31. Genetic variants may influence the outcome through the associated continuous risk factor without changing the binary outcome itself31. However, we have observed that the genetic risk score for depression and other binary measures are associated with severity and is therefore representing an increased genetic liability to risk. We also acknowledge that GWASs of social traits such as depression and anxiety may be confounded by factors such as assortative mating and other indirect genetic effects.
This study has utilised several MR methods to account for potential biases associated with pleiotropy, sample overlap and weak instruments. In general, consistent results were seen across the different methods. Whilst each method has its own limitations, our use of multiple techniques, with consistent results, provides more confidence in our findings.
In conclusion, we have provided further evidence that fall risk is a heritable, heterogenous and polygenic trait, when using a balance related fall metric. We provide robust evidence for higher BMI (independent of metabolic consequences), depression, neuroticism and physical inactivity as risk factors for falling. Using multiple MR approaches, our study provides novel insights into factors that may cause falls, which can be used to optimise fall prevention strategies and to improve further research into balance control strategies.
References
Maurer, C., Mergner, T. & Peterka, R. J. Multisensory control of human upright stance. Exp. Brain Res. 171, 231–250 (2006).
Horak, F. B. Postural orientation and equilibrium: What do we need to know about neural control of balance to prevent falls?. Age Ageing 35, ii7–ii11 (2006).
Ma, R. et al. Predictors of falls and fractures leading to hospitalisation in 36 101 people with affective disorders: A large representative cohort study. BMJ Open 12, e055070 (2022).
CDC, CENTERS FOR DISEASE CONTROL AND PREVENTION. 2020: https://www.cdc.gov/injury/wisqars/index.html.
Gauchard, G., Chau, N., Mur, J. M. & Perrin, P. Falls and working individuals: Role of extrinsic and intrinsic factors. Ergonomics 44(14), 1330–1339 (2001).
Sherrington, C. et al. Evidence on physical activity and falls prevention for people aged 65+ years: Systematic review to inform the WHO guidelines on physical activity and sedentary behaviour. Int. J. Behav. Nutr. Phys. Act. 17(1), 1–9 (2020).
Iaboni, A. & Flint, A. J. The complex interplay of depression and falls in older adults: A clinical review. Am. J. Geriatr. Psychiat. 21(5), 484–492 (2013).
Alenazi, A. M. Functional reach, depression scores, and number of medications are associated with number of falls in people with chronic stroke. PMR 10(8), 806–816 (2018).
Delbaere, K. Determinants of disparities between perceived and physiological risk of falling among elderly people: Cohort study. BMJ. 341, 4165 (2010).
Zisakis, A., Exadaktylos, A. & Lindner, G. Fall-related emergency department admission: Fall environment and settings and related injury patterns in 6357 patients with special emphasis on the elderly. Minerva Med 105, 275–281 (2014).
Lawlor, D. A., Harbord, R. M., Sterne, J. A., Timpson, N. & Davey Smith, G. Mendelian randomization: Using genes as instruments for making causal inferences in epidemiology. Stat. Med. 27(8), 1133–1163 (2008).
Vandenbroucke, J. P. When are observational studies as credible as randomised trials?. Lancet 363, 1728–1731 (2004).
Trajanoska, K. et al. Genetic basis of falling risk susceptibility in the UK Biobank Study. Commun. Biol. 3(1), 543 (2020).
Davies, N. M., Holmes, M. V. & Smith, G. D. Reading Mendelian randomisation studies: A guide, glossary, and checklist for clinicians. Bmj 362, k601 (2018).
Bunn, F. et al. Preventing falls among older people with mental health problems: A systematic review. BMC Nurs. 13, 1–15 (2014).
Heslop, K. et al. Assessing falls risk in older adult mental health patients: A Western Australian review. Int. J. Mental Health Nurs. 21(6), 567–575 (2012).
Jo, K. H., Park, J. & Ryu, S. Y. The effects of mental health on recurrent falls among elderly adults, based on Korean Community Health Survey data. Epidemiol. Health 42, e2020005 (2020).
Sudlow, C. et al. UK biobank: An open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 12(3), e1001779 (2015).
Bycroft, C. et al. The UK Biobank resource with deep phenotyping and genomic data. Nature 562(7726), 203–209 (2018).
Jones, S. E. et al. Genome-wide association analyses in 128,266 individuals identifies new morningness and sleep duration Loci. PLoS Genet. 12(8), e1006125 (2016).
Yaghootkar, H. et al. Genetic evidence for a link between favorable adiposity and lower risk of type 2 diabetes, hypertension, and heart disease. Diabetes 65(8), 2448–2460 (2016).
Virtue, S. & Vidal-Puig, A. Adipose tissue expandability, lipotoxicity and the metabolic syndrome—An allostatic perspective. Biochim. Biophys. Acta BBA 1801(3), 338–349 (2010).
DNA Nexus. Available from: https://www.dnanexus.com/.
Bycroft, C. et al. The U.K. Biobank resource with deep phenotyping and genomic data. Nature 562, 203–209 (2018).
Mbatchou, J. et al. Computationally efficient whole-genome regression for quantitative and binary traits. Nat. Genet. 53, 1097–1103 (2021).
Bulik-Sullivan, B. An atlas of genetic correlations across human diseases and traits. Nat. Genet. 47(11), 1236–1241 (2015).
Bowden, J., Davey Smith, G. & Burgess, S. Mendelian randomization with invalid instruments: Effect estimation and bias detection through egger regression. Int. J. Epidemiol. 44(2), 512–525 (2015).
Bowden, J., Davey Smith, G., Haycock, P. C. & Burgess, S. Consistent estimation in Mendelian randomization with some invalid instruments using a weighted median estimator. Genet. Epidemiol. 40(4), 304–314 (2016).
Burgess, S. & Thompson, S. G. Interpreting findings from Mendelian randomization using the MR-Egger method. Eur. J. Epidemiol. 32, 377–389 (2017).
Mounier, N., Bias, Z. K. Correction for inverse variance weighting Mendelian randomization. bioRxiv, 2021.
Burgess, S. & Labrecque, J. A. Mendelian randomization with a binary exposure variable: Interpretation and presentation of causal estimates. Eur. J. Epidemiol. 33, 947–952 (2018).
Karageorgiou, V., Tyrrell, J., Mckinley, T. J. & Bowden, J. Weak and pleiotropy robust sex-stratified Mendelian randomization in the one sample and two sample settings. Genet. Epidemiol. 47(2), 135–151 (2023).
Jones, G. et al. Genome-wide meta-analysis of muscle weakness identifies 15 susceptibility loci in older men and women. Nat. Commun. 12, 654 (2021).
Caron, B. et al. Integrative genetic and immune cell analysis of plasma proteins in healthy donors identifies novel associations involving primary immune deficiency genes. Genome Med. 14(1), 28 (2022).
Richardson, T. G. et al. Characterising metabolomic signatures of lipid-modifying therapies through drug target mendelian randomisation. PLoS Biol. 20(2), e3001547 (2022).
Park, J. Y. et al. A missense variant in SHARPIN mediates Alzheimer’s disease-specific brain damages. Transl. Psychiatry 11(1), 590 (2021).
Moreno-Grau, S. et al. Genome-wide association analysis of dementia and its clinical endophenotypes reveal novel loci associated with Alzheimer’s disease and three causality networks: The GR@ ACE project. Alzheimer’s Dement. 15(10), 1333–1347 (2019).
Deelen, J. et al. A meta-analysis of genome-wide association studies identifies multiple longevity genes. Nat. Commun. 10(1), 3669 (2019).
Kemp, J. P. et al. Identification of 153 new loci associated with heel bone mineral density and functional involvement of GPC6 in osteoporosis. Nat. Genet. 49(10), 1468–1475 (2017).
Wray, N. R. et al. Genome-wide association analyses identify 44 risk variants and refine the genetic architecture of major depression. Nat. Genet. 50, 668–681 (2018).
UCSC, UCSC Genome Browser. https://genome.ucsc.edu/cgi-bin/hgTracks?db=hg38&lastVirtModeType=default&lastVirtModeExtraState=&virtModeType=default&virtMode=0&nonVirtPosition=&position=chr19%3A44908584%2D44908784&hgsid=1643981730_Fiyi4TTQQC4hbEuVoJ8AAlzuXQMv.
Poirier, J. et al. Apolipoprotein E polymorphism and Alzheimer’s disease. Lancet 342, 697–699 (1993).
Bis, J. C. et al. Meta-analysis of genome-wide association studies from the CHARGE consortium identifies common variants associated with carotid intima media thickness and plaque. Nat. Genet. 43(10), 940–947 (2011).
Said, S. et al. Genetic analysis of over half a million people characterises C-reactive protein loci. Nat. Commun. 13(1), 2198 (2022).
Hubáček, J. A. Genetic determination of dyslipidemia-What tell us the results of genome-wide association studies?. Vnitrni lekarstvi 62(11), 868–876 (2016).
Mitchell, R. J., Lord, S. R., Harvey, L. A. & Close, J. C. T. Associations between obesity and overweight and fall risk, health status and quality of life in older people. Aust. N. Z. J. Public Health 38, 13–18 (2014).
Merrill, Z., Perera, S., Chambers, A. & Cham, R. Age and body mass index associations with body segment parameters. J. Biomech. 88, 38–47 (2019).
Menegoni, F. et al. Gender-specific effect of obesity on balance. Obesity 17(10), 1951–1956 (2009).
Lee, J. J. et al. Relationship between obesity and balance in the community-dwelling elderly population. Am. J. Phys. Med. Rehabi. 99, 65–70 (2020).
Martin, S. et al. Genetic evidence for different adiposity phenotypes and their opposing influences on ectopic fat and risk of cardiometabolic disease. Diabetes 70, 1843–1856 (2021).
Dutil, M. et al. The impact of obesity on balance control in community-dwelling older women. Age 35, 883–890 (2013).
Del Porto, H., Pechak, C., Smith, D. & Reed-Jones, R. Biomechanical effects of obesity on balance. Int. J. Exerc. Sci. 5(4), 301–320 (2012).
Thomas, E. et al. Physical activity programs for balance and fall prevention in elderly: A systematic review. Medicine 98, e16218 (2019).
Choi, N. G. et al. Longitudinal associations of falls and depressive symptoms in older adults. Gerontologist 59(6), 1141–1151 (2019).
Deandrea, S. et al. Risk factors for falls in community-dwelling older people: A systematic review and meta-analysis. Epidemiology 21(5), 658–668 (2010).
Turunen, K. M. et al. Associations of neuroticism with falls in older adults: Do psychological factors mediate the association?. Aging Mental Health 26(1), 77–85 (2022).
Hallford, D. J., Nicholson, G., Sanders, K. & McCabe, M. P. The association between anxiety and falls: A meta-analysis. J. Gerontol. Series B: Psychol. Sci. Soc. Sci. 72, 729–741 (2017).
Yardley, L. et al. Falls efficacy scale—International. Archiv. Gerontol. Geriatr. https://doi.org/10.1037/t01443-000 (2005).
Ellmers, T. J., Wilson, M. R., Norris, M. & Young, W. R. Protective or harmful? A qualitative exploration of older people’s perceptions of worries about falling. Age Ageing 51(4), afac067 (2022).
Tyrrell, J. et al. Genetic predictors of participation in optional components of UK Biobank. Nat. Commun. 12(1), 886 (2021).
Fry, A. et al. Comparison of sociodemographic and health-related characteristics of UK biobank participants with those of the general population. Am. J. Epidemiol. 186(9), 1026–1034 (2017).
Aune, D. et al. BMI and all cause mortality: Systematic review and non-linear dose-response meta-analysis of 230 cohort studies with 374 million deaths among 303 million participants. Bmj 353, i2156 (2016).
Yengo, L. et al. Meta-analysis of genome-wide association studies for height and body mass index in ∼700000 individuals of European ancestry. Hum. Mol. Genet. 27(20), 3641–3649 (2018).
Howard, D. M. et al. Genome-wide meta-analysis of depression identifies 102 independent variants and highlights the importance of the prefrontal brain regions. Nat. Neurosci. 22, 343–352. https://doi.org/10.1038/s41593-018-0326-7 (2019).
Otowa, T. et al. Meta-analysis of genome-wide association studies of anxiety disorders. Mol. Psychiatry 21, 1391–1399. https://doi.org/10.1038/mp.2015.197 (2016).
Willems, S. et al. Large-scale GWAS identifies multiple loci for hand grip strength providing biological insights into muscular fitness. Nat. Commun. 8, 16015. https://doi.org/10.1038/ncomms16015 (2017).
Locke, A. et al. Genetic studies of body mass index yield new insights for obesity biology. Nature 518, 197–206. https://doi.org/10.1038/nature14177 (2015).
McGrath, R., Blackwell, T. L., Ensrud, K. E., Vincent, B. M. & Cawthon, P. M. The associations of handgrip strength and leg extension power asymmetry on incident recurrent falls and fractures in older men. J. Gerontol. A. Biol. Sci. Med. Sci. 76(9), e221–e227. https://doi.org/10.1093/gerona/glab133 (2021).
Thibaud, M. et al. Impact of physical activity and sedentary behaviour on fall risks in older people: a systematic review and meta-analysis of observational studies. Eur. Rev. Aging Phys. Act. 9, 5–15. https://doi.org/10.1007/s11556-011-0081-1 (2012).
Tan, G. J. et al. The relationship between alcohol intake and falls hospitalization: Results from the EPIC-Norfolk. Geriatr. Gerontol. Int. 21(8), 657–663. https://doi.org/10.1111/ggi.14219 (2021).
Ek, S. et al. Risk factors for injurious falls in older adults: The role of sex and length of follow-up. J. Am. Geriatr. Soc. 67(2), 246–253. https://doi.org/10.1111/jgs.15657 (2019).
Luciano, M. et al. Association analysis in over 329,000 individuals identifies 116 independent variants influencing neuroticism. Nat. Genet. 50, 6–11. https://doi.org/10.1038/s41588-017-0013-8 (2018).
Ware, J. et al. Genome-Wide Meta-Analysis of Cotinine Levels in Cigarette Smokers Identifies Locus at 4q13.2. Sci. Rep. 6, 20092. https://doi.org/10.1038/srep20092 (2016).
Clarke, T. K. et al. Genome-wide association study of alcohol consumption and genetic overlap with other health-related traits in UK Biobank (N=112 117). Mol. Psychiatry 22, 1376–1384. https://doi.org/10.1038/mp.2017.153 (2017).
Marioni, R. E. et al. Genetic variants linked to education predict longevity. PNAS 113(47), 13366–13371. https://doi.org/10.1073/pnas.1605334113 (2016).
Kim, T., Choi, S. D. & Xiong, S. Relationship between socio-economic factors and fall risk for elder Koreans. Adv. Intell. Syst. Comput. 789, 435–444 (2018).
Heesch, K. C., Byles, J. E. & Brown, W. J. Prospective association between physical activity and falls in community-dwelling older women. J. Epidemiol. Community Health. 62(5), 421–426. https://doi.org/10.1136/jech.2007.064147 (2008).
Funding
MS was supported by The Graham Cole PhD Studentship. This study was supported by the National Institute for Health and Care Research Exeter Biomedical Research Centre. The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
Author information
Authors and Affiliations
Contributions
J.T. conceived and designed the study. M.S., J.T., J.O. and V.K. contributed to the data analysis. M.S. and V.K. contributed to the figures and tables. M.S., J.T., V.K., J.O., F.C., G.W. and M.H. contributed to the writing of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Smith, M.C., O’Loughlin, J., Karageorgiou, V. et al. The genetics of falling susceptibility and identification of causal risk factors. Sci Rep 13, 19493 (2023). https://doi.org/10.1038/s41598-023-44566-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-44566-w
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
