
Abstract
Adenosine occasionally results in overestimation of fractional flow reserve (FFR) values, compared with other hyperemic stimuli. We aimed to elucidate the association of overestimation of FFR by adenosine with anatomically significant but functionally non-significant lesions (anatomical–functional mismatch) and its influence on reclassification of functional significance. Distal-to-aortic pressure ratio (Pd/Pa) was measured using adenosine (Pd/PaADN) and papaverine (Pd/PaPAP) in 326 patients (326 vessels). The overestimation of FFR was calculated as Pd/PaADN–Pd/PaPAP. The anatomical–functional mismatch was defined as diameter stenosis > 50% and Pd/PaADN > 0.80. Reclassification was indicated by Pd/PaADN > 0.80 and Pd/PaPAP ≤ 0.80. The mismatch (n = 72) had a greater overestimation of FFR than the non-mismatch (n = 99): median 0.02 (interquartile range 0.01–0.05) versus 0.01 (0.00–0.04), p = 0.014. Multivariable analysis identified the overestimation of FFR (p = 0.003), minimal luminal diameter (p = 0.001), and non-left anterior descending artery (LAD) location (p < 0.001) as determinants of the mismatch. Reclassification was indicated in 29% of the mismatch and was more frequent in the LAD than in the non-LAD (52% vs. 20%, p = 0.005). The overestimation of FFR is an independent determinant of anatomical−functional mismatch. Anatomical−functional mismatch, specifically in the LAD, may suggest a false-negative result.
Similar content being viewed by others

Introduction
Diameter stenosis (DS) of > 50% on invasive coronary angiography is deemed anatomically significant1. Coronary angiography alone, however, has limited ability to differentiate functionally significant lesions2,3,4,5,6,7. Pressure wire-derived fractional flow reserve (FFR) has emerged as the gold standard for assessing the functional impact of stenotic lesions, and a vessel with an FFR value ≤ 0.80 is considered to have functionally significant stenosis2,8,9,10,11. It is well known that the anatomical and functional significance of coronary lesions does not always match2,3,4. Previous studies have identified clinical and pathophysiological factors associated with anatomically significant but functionally non-significant lesions (anatomical–functional mismatch)3,4,5,6,7,12.
The principle of FFR is based on the premise that coronary pressure is linearly related to myocardial blood flow under maximal hyperemia9,13. If maximal hyperemia is not induced, an FFR value becomes erroneously higher than the true FFR value. This overestimation of FFR underestimates the severity of ischemia and poses a risk of leaving an ischemic lesion untreated14. Intravenous adenosine, used most widely for hyperemia induction13,15, occasionally fails to induce maximal hyperemia when compared with other hyperemic stimuli, especially if the subject has consumed caffeine, a competitive antagonist of the target receptor of adenosine16,17,18,19,20. Although an overestimation of FFR by adenosine may cause an anatomical–functional mismatch (DS > 50% and FFR > 0.80), the association between the overestimation of FFR by adenosine and anatomical–functional mismatch has not been fully explored. Previous studies on anatomical–functional mismatch have used only adenosine to produce hyperemia, thereby precluding assessment of adenosine’s role in the mismatch3,4,5,6,12. If the anatomical–functional mismatch is associated with the overestimation of FFR by adenosine, vessels having the mismatch with adenosine may show functional significance when using another stimulus.
Papaverine induces maximal hyperemia most reliably by directly relaxing the vascular smooth muscle, without involving the adenosine A2a receptors16,17,18,19,21. This study compared distal-to-aortic pressure ratio (Pd/Pa) associated with adenosine (Pd/PaADN) and Pd/Pa associated with papaverine (Pd/PaPAP), as a reference standard. We sought to determine whether (1) the overestimation of FFR by adenosine is associated with the discordance between the anatomical and functional significance and (2) functional significance in such lesions is reclassified when papaverine is used as the indicator.
Methods
Study patients
This study retrospectively analyzed the data of 365 consecutive patients with chronic coronary syndrome undergoing clinically indicated coronary angiography and an FFR assessment for coronary stenosis of 30–90% based on visual estimations during angiography. If FFR was measured in two or more vessels in a patient, only the first vessel was included in this study. All patients were asked to abstain from food and beverages for > 3 h before the catheterization. Periods for caffeine abstinence were left to the referring physicians’ discretion. This study excluded vessels with lesions on the coronary ostium, severe arrhythmia (e.g. atrial fibrillation or frequent ectopic beats), a prior coronary artery bypass graft, significant valvular disease, or any contraindications for adenosine or papaverine, as well as patients taking theophylline-containing medications. Patients with insufficient pressure data quality, including inadequate waveform tracings and signal drift more than ± 0.03 after the pullback of the pressure wire, were also excluded from the analysis.
The coronary physiology assessment was performed as part of the routine diagnostic coronary angiography procedures for clinical purposes. All methods were performed in accordance with the relevant guidelines and regulations. Written informed consent for the invasive physiology assessment was obtained from all of the patients before the procedure. The Institutional Review Board approved this retrospective study and waived the requirement to obtain patient approval and written informed consent for the review of patient data and medical records (reference #3234/ Showa University School of Medicine; 31 August, 2021).
Fractional flow reserve measurements
Diagnostic coronary angiography was performed in a standard manner. Thereafter, the FFR was measured using a 5- or 6-F guiding catheter without side holes and a commercially available FFR system (Philips Volcano or Abbott Vascular) in accordance with standardized procedures13. After administration of intracoronary isosorbide dinitrate, distal coronary pressure and aortic pressure were simultaneously measured at baseline and during hyperemia. The guiding catheter was disengaged from the ostium during FFR measurements, and special care was taken not to alter the wire position.
Adenosine was continuously given via a femoral vein or a large forearm vein at a dose of 140 μg/kg/min for more than 150 s9,13,15,22. When Pd/Pa values were not stable during adenosine infusion, adenosine was continued for more than 180 s. Papaverine was used as the last agent to obtain a reliable pull-back curve, as it induces hyperemia with minimal variations in Pd/Pa23. After confirming that Pd/Pa values had returned to the baseline level, with an interval of ≥ 5 min, intracoronary papaverine (8–10 mg in the right coronary artery or 12–15 mg in the left coronary artery) was given through the coronary catheter, followed by 5 ml of saline9,13. Approximately 20 s after the papaverine injection, an FFR pullback recording was performed manually, and the presence of pressure-wire drift was checked.
Data analysis
Fractional flow reserve
Experienced observers blinded to patients’ coronary angiography results and clinical data manually reviewed the pressure recordings. Pd/PaADN was determined during the steady-state hyperemic plateau phase > 60 s after the initiation of adenosine and > 15 s after the transition to hyperemia19,24. The lowest Pd/Pa values on a beat-to-beat basis for adenosine and papaverine were regarded as Pd/PaADN and Pd/PaPAP, respectively16,17,18,19,25. The overestimation of FFR by adenosine was defined as Pd/PaADN – Pd/PaPAP19.
Coronary angiography
Quantitative coronary angiography was performed with a commercially available system (CAAS Workstation version 7.5, Pie Medical Imaging) by independent investigators unaware of patients’ FFR results or clinical data. Reference diameter, minimum lumen diameter, and lesion length were measured using the external diameter of the catheter as a scaling device, and DS was calculated. Proximal location was defined as Syntax segments 1, 5, 6, and 1126. The anatomical–functional mismatch was defined as DS > 50% and Pd/PaADN > 0.80, and the reverse mismatch was defined as DS ≤ 50% and Pd/PaADN ≤ 0.80.
Reclassification of functional significance
Reclassification of functional significance was indicated by FFRADN > 0.80 and FFRPAP ≤ 0.80 (false-negative by adenosine), and reverse reclassification as FFRADN ≤ 0.80 and FFRPAP > 0.80 (false-positive by adenosine).
Statistical analysis
Continuous variables were presented as medians with interquartile ranges (IQRs). Categorical variables were expressed as frequencies with percentages. Between-group comparisons were made with unpaired-sample t-test or Mann–Whitney U test for quantitative variables and with the χ2 test or Fisher’s exact test for categorical variables, as appropriate. The correlation between DS and Pd/PaADN was assessed with Spearman’s rank correlation coefficient. Multivariable logistic regression analysis was used to determine factors associated with the anatomical–functional mismatch and the reverse mismatch. Clinical, angiographic, and hemodynamic parameters with a univariable association of p < 0.10 were entered into the multivariable model. Results were presented as odds ratios (ORs) and 95% confidence intervals (CIs). The numbers of the mismatch in vessels with DS > 50% and the reverse mismatch in vessels with DS ≤ 50% were compared between adenosine and papaverine using the McNemar test. Statistical analyses were performed using JMP® Pro, version 16.0.0. (SAS Institute Inc., Cary, NC, USA). A p value of < 0.05 was considered statistically significant.
Results
Patient and lesion characteristics
Of the 365 patients, 39 were excluded due to sensor drift (n = 13), insufficient waveform tracings (n = 10), side effects of adenosine (n = 8) or papaverine (n = 2), or difficulty in advancing the pressure wire far enough distal from the index lesion (n = 6), leaving 326 patients (326 vessels) in the analysis. Table 1 summarizes the patient and lesion characteristics.
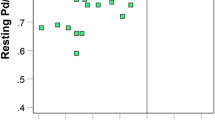
The median DS was 50.6% (IQR 42.4–57.5%), and the median Pd/PaADN was 0.79 (0.73–0.86). Figure 1 shows a scatter plot of DS and Pd/PaADN. The relationship between DS and Pd/PaADN was modest, with a large scatter (ρ =−0.223, p < 0.001). DS > 50% was observed in 171 vessels (52%), and DS ≤ 50% in 155 vessels (48%). Among the vessels with DS > 50%, 72 and 99 vessels demonstrated Pd/PaADN > 0.80 and Pd/PaADN ≤ 0.80, respectively. Of the vessels with DS ≤ 50%, 76 and 79 vessels showed Pd/PaADN ≤ 0.80 and Pd/PaADN > 0.80, respectively.

Scatter plot of DS and Pd/PaADN The anatomical‒functional mismatch was defined as DS > 50% and Pd/PaADN > 0.80, and the reverse mismatch as DS > 50% and Pd/PaADN ≤ 0.80. DS diameter stenosis, and Pd/PaADN distal-to-aortic pressure ratio associated with adenosine.
Anatomically significant vessels
Table 2 compares patient and lesion characteristics in vessels with DS > 50% between the mismatch (Pd/PaADN > 0.80) and non-mismatch (Pd/PaADN ≤ 0.80) groups. There was no significant difference in age, sex, body size, or coronary risk factors between groups. Concerning lesion characteristics, the mismatch group was associated with a higher frequency of non-LAD location (71% vs. 27%, p < 0.001), a greater reference diameter (3.1 mm [IQR 2.6–3.5 mm] vs. 2.7 mm [IQR 2.2–3.2 mm], p = 0.001), a larger minimal luminal diameter (1.3 mm [IQR 1.1–1.5 mm] vs. 1.1 mm [IQR 0.9–1.3 mm], p < 0.001), a smaller DS (55.8% [IQR 52.8–61.3%] vs. 59.0% [IQR 53.9–64.9%], p = 0.038), and a shorter lesion length (11.2 mm [IQR 7.9–15.8] vs. 13.2 mm [IQR 9.3–20.8], p = 0.029) than the non-mismatch group.
Pd/PaADN values were significantly higher than Pd/PaPAP values, regardless of the presence of anatomical–functional mismatch (0.78 [IQR 0.70–0.85] vs. 0.76 [IQR 0.68–0.83], p < 0.001 for all vessels with DS > 50%; 0.86 [IQR 0.82–0.89] vs. 0.84 [IQR 0.80–0.87], p < 0.001 for the mismatch group; and 0.72 [IQR 0.65–0.77] vs. 0.69 [IQR 0.61–0.76], p < 0.001 for the non-mismatch group). Figure 2 depicts the distributions of the overestimation of FFR by adenosine in the two groups. The mismatch group had a greater overestimation than the non-mismatch group (0.02 [IQR 0.01–0.05] vs. 0.01 [IQR 0.00–0.04], p = 0.014).

Comparison of overestimation of FFR by adenosine in anatomically significant vessels between the anatomical‒functional mismatch and non-mismatch groups. Distributions of overestimation of FFR by adenosine with box-and-whisker plots are shown. The overestimation of FFR by adenosine was defined as Pd/PaADN–Pd/PaPAP. DS diameter stenosis, Pd/PaADN distal-to-aortic pressure ratio associated with adenosine, and Pd/PaADN distal-to-aortic pressure ratio associated with papaverine.
Based on the results from the univariable analysis (Suppl. Table S1), we entered the overestimation of FFR (p = 0.014), non-LAD location (p < 0.001), reference diameter (p = 0.004), and minimal luminal diameter (p = 0.001) in the multivariable model. As shown in Table 3, multivariable logistic regression analysis identified the overestimation of FFR (OR per 0.01 increase: 1.16 [95% CI: 1.05–1.28], p = 0.003), non-LAD location (OR: 9.08 [95% CI: 4.15–19.88], p < 0.001), and minimal luminal diameter (OR per 0.1 mm increase: 1.31 [95% CI: 1.11–1.54], p = 0.001) as independent factors associated with the anatomical–functional mismatch.
Figure 3 displays a scatter plot of Pd/PaADN and Pd/PaPAP in vessels with DS > 50%. Compared to adenosine, papaverine significantly decreased the number of vessels with anatomical–functional mismatch (99 [58%] vs. 116 [68%], p = 0.001). In the mismatch group, the reclassification of functional significance by papaverine (Pd/PaADN > 0.80 and Pd/PaPAP ≤ 0.80) was observed in 29% (21/72). Of these, 12 vessels had an overestimation of FFR of ≥ 0.05, and 7 vessels had Pd/PaPAP values of ≤ 0.75. Reclassification was more frequently observed in LAD lesions than in non-LAD lesions (52% [11/21] vs. 20% [10/51], p = 0.005). In the non-mismatch group, reverse reclassification (Pd/PaADN ≤ 0.80 and Pd/PaPAP > 0.80) was observed in only 4% (4/99). In all vessels, Pd/PaADN showed borderline values (0.78–0.80), with small differences from Pd/PaPAP (≤ 0.03).

Scatter plot of Pd/PaADN and Pd/PaPAP in vessels with a diameter stenosis of > 50%. The dashed line indicates the line of identity. LAD left anterior descending artery, Pd/PaADN distal-to-aortic pressure ratio associated with adenosine, and Pd/PaADN distal-to-aortic pressure ratio associated with papaverine.
Anatomically non-significant vessels
Table 4 compares the patient and lesion characteristics in the vessels with DS ≤ 50% between the reverse mismatch (Pd/PaADN ≤ 0.80) and non-reverse mismatch (Pd/PaADN > 0.80) groups. The reverse mismatch group was associated with male sex (82% vs. 67%, p < 0.039), a higher frequency of non-LAD location (72% vs. 54%, p = 0.021), a smaller reference diameter (2.6 mm [IQR 2.3–3.1 mm]) vs. 2.9 mm [IQR 2.6–3.3 mm], p = 0.002), and a smaller minimal luminal diameter (1.5 mm [IQR 1.3–1.8 mm]) vs. 1.7 mm [IQR 1.6–2.1 mm], p < 0.001) compared to the non-reverse mismatch group. No significant difference in the overestimation of FFR was observed between the two groups (p = 0.224).
Based on the results of the univariable analysis (Suppl. Table S2), male sex (p = 0.042), body mass index (p = 0.061), LAD location (p = 0.022), reference diameter (p = 0.001), and minimal luminal diameter (p < 0.001) were included in the multivariable model. The results of the multivariable logistic regression analysis revealed the following as independent factors associated with the reverse mismatch (Table 5): male sex (OR: 2.43 [95% CI: 1.07–5.51], p = 0.034), LAD location (OR: 2.22 [95% CI: 1.05–4.67], p = 0.037), and minimal luminal diameter (OR per 0.1 mm increase: 0.75 [95% CI: 0.61–0.91], p = 0.034) as independent factors associated with the reverse mismatch (Table 5).
Compared to adenosine, papaverine significantly increased the number of vessels with the anatomical–functional reverse mismatch (76 [49%] vs. 85 [55%], p = 0.022). In the non-reverse mismatch group, reclassification of functional significance was observed in 11 vessels (14%). In the reverse mismatch group, reverse reclassification was in observed only 2 vessels (3%).
Discussion
Evaluating FFR values obtained with adenosine and papaverine in relation to DS on coronary angiography, we found that 1) the overestimation of FFR by adenosine was an independent determinant of the anatomical–functional mismatch; 2) in 30% of vessels with the anatomical–functional mismatch, functional significance was reclassified from negative by adenosine (Pd/PaADN > 0.80) to positive by papaverine (Pd/PaPAP ≤ 0.80); and 3) this reclassification was observed more frequently in LAD lesions (52%) than in non-LAD lesions (20%).
Anatomical–functional mismatch and overestimation of FFR by adenosine
An animal experimental study published in 1974 showed that hyperemic coronary flow starts to decrease from a DS of 50%27. Based on this result, the 50% threshold continues to be used to define anatomically significant stenosis. Obviously, a result derived from a controlled experiment in healthy animals cannot be accurately applied to patients with coronary artery disease. Patients requiring an FFR assessment often have diffuse atherosclerosis other than that at the site with minimal lumen diameter, which progressively decreases coronary pressure28,29. Unlike two-dimensional angiographic projection images, FFR reflects the totality of the physiological effects of patient characteristics, lesion characteristics, microvascular function, amount of myocardial mass subtended by the coronary artery stenosis, and hyperemia3,7,11,12,30,31,32. Consistent with prior studies3,12, non-LAD location and minimal luminal diameter were associated with an anatomical–functional mismatch. This study is first to demonstrate that the overestimation of FFR by adenosine is an independent determinant after adjusting for these known factors in the multivariable model.
There could be several potential factors associated with the overestimation of FFR observed in the present study. Although the 140 μg/kg/min dose of intravenous adenosine used in the present study has been recognized as the standard method for hyperemia induction9,13,15, a higher dose may be required, specifically when administered through a peripheral vein33.
Another potential explanation would be caffeine. The effects of caffeine on inhibiting adenosine hyperemia are definitively established34.While individually variable, caffeine reduces the average accuracy of all diagnostic metrics using vasodilatory stress. In the present study of Pd/PaPAP compared to Pd/PaADN without systematic pre-procedure instruction for caffeine abstinence, higher Pd/PaADN values than Pd/PaPAP values may have largely reflected caffeine effects in addition to other primary pharmacologic differences. Although a non-invasive imaging guideline recommends 12-h caffeine abstinence before adenosine stress tests35, more prolonged abstinence may be required for adenosine-induced FFR measurements. The overestimation of FFR by adenosine occurred at much lower serum caffeine levels than those found after the recommended 12-h abstinence and increased in a concentration–response manner19. Our present findings mirrored real-world clinical situations. The frequency of anatomical–functional mismatch was consistent with that of earlier investigations that used adenosine or adenosine triphosphate3,12. Although those investigations did not provide information about serum caffeine levels or the length of caffeine abstinence3,12, their results might be attributed in part to caffeine. Our present results suggest the need for standardized caffeine control before FFR measurements.
Reclassification of functional significance due to FFRADN overestimation
A large randomized trial confirmed that revascularization reduced adverse cardiac events in patients who had coronary stenosis with FFR ≤ 0.8010. Recent guidelines consider coronary lesions with DS > 50% and FFR ≤ 0.80 to be indicated for revascularization8,36. In this study conducted on real-world patients, the functional significance was reclassified from negative by adenosine to positive by papaverine in as many as 30% of vessels with the anatomical-functional mismatch. Notably, more than half of vessels with reclassification status had a large overestimation of FFR by adenosine more than 2 standard deviations between repeated adenosine-induced FFR measurements24. Even FFR values in the gray zone (0.76–0.80) were associated with a high rate of death or myocardial infarction when treated with medical therapy alone37. The reclassification, specifically due to a large overestimation of FFR, may lead to worse clinical outcomes.
The present and previous studies found non-LAD location to be an independent determinant of the anatomical–functional mismatch3,12. This is a reasonable result from a physiological point of view. Stenosis in the non-LAD vessels, which subtends smaller myocardial masses than that in the LAD, produces a less hyperemic gradient across the lesion. Even with the anatomically significant stenosis of DS > 50%, the non-LAD is less likely to have FFR ≤ 0.80 than the LAD. Indeed, in the present study, the frequency of the anatomical–functional mismatch was higher in the non-LAD than in the LAD. Of note, however, the reclassification was observed in more than one-half of LAD vessels with the anatomical–functional mismatch. Physicians should keep in mind that when using adenosine, the anatomical–functional mismatch, specifically in the LAD, may suggest a false-negative result.
Factors associated with anatomical–functional reverse mismatch
In agreement with previous studies3,5,12, our analyses revealed that male sex, LAD location, and minimal lumen diameter are independent determinants of the anatomical–functional reverse mismatch. A greater pressure gradient is produced across a lesion located in the LAD, subtending larger myocardial masses than a lesion located in the non-LAD3,12. Likewise, males (with larger myocardial masses than females) are likely to have lower FFR values5.
Clinical implications
Given that revascularization reduces adverse cardiac events even in patients with gray zone FFR values compared with medical therapy alone38, patients with overestimations of FFR may miss the opportunity to receive the benefits of revascularization. The concept of FFR was established under the assumption of minimal microvascular resistance9. Our findings underscore the importance of inducing maximal hyperemia in FFR measurements to avoid misinterpretations of the FFR results. Significantly, more than half of LAD lesions with the anatomical–functional mismatch demonstrated false-negative results. Considering that stenotic lesions in the LAD carry a worse prognosis than in other locations39, LAD lesions with anatomical–functional mismatch are more clinically relevant.
FFR overestimations by adenosine (i.e. insufficient adenosine-induced hyperemia) will not be identified unless another hyperemic stimulus is used. Serum caffeine was reported to be a major determinant19; however the serum caffeine level is unpredictable even after caffeine abstinence because it depends on various factors, including the inter-individual variation in caffeine’s half-life, patient compliance, and the recently ingested caffeine dose. In the context of a lack of a rapid test kit to detect serum caffeine, the anatomical–functional mismatch provides a clue to insufficient adenosine-induced hyperemia.
Study limitations
We acknowledge several limitations to this study. First, we did not determine the clinical significance of the anatomical–functional mismatch and/or the reclassification due to the overestimation of FFR by adenosine. This was because some of the vessels with DS > 50% and negative FFR results by adenosine were revascularized based on positive FFR results by papaverine. Further research is warranted to address this topic. Second, microvascular function was not assessed. High microcirculatory resistance might affect the overestimation of FFR. However, in the presence of insufficient adenosine-induced hyperemia, microcirculatory resistance cannot be accurately assessed by adenosine. Multiple injections of papaverine to measure microcirculatory resistance, together with FFR, may carry an increased risk of side effects. Third, the patients' serum caffeine levels were not measured in this study. Lastly, the order of hyperemic agents was fixed (papaverine last) because papaverine was used to obtain a reliable pullback curve. Although papaverine was administered after confirming that Pd/Pa values had returned to the baseline level, adenosine’s carry-over effect cannot be excluded.
Conclusions
The overestimation of FFR by adenosine compared to papaverine is an independent determinant of anatomical–fucntional mismatch. It should be kept in mind that anatomical–functional mismatch, specifically in the LAD and potentially due to caffeine, may suggest a false-negative result.
Abbreviations
- CI:
-
Confidence interval
- DS:
-
Diameter stenosis
- Pd/Pa:
-
Distal-to-aortic pressure ratio
- Pd/PaADN :
-
Distal-to-aortic pressure ratio associated with adenosine
- Pd/PaPAP :
-
Distal-to-aortic pressure ratio associated with papaverine
- FFR:
-
Fractional flow reserve
- IQR:
-
Interquartile range
- LAD:
-
Left anterior descending artery
- OR:
-
Odds ratio
- Pa:
-
Mean aortic pressure
- Pd:
-
Mean distal coronary pressure
References
Sianos, G. et al. The SYNTAX Score: An angiographic tool grading the complexity of coronary artery disease. EuroIntervention 1, 219–227 (2005).
Tonino, P. A. et al. Angiographic versus functional severity of coronary artery stenoses in the FAME study fractional flow reserve versus angiography in multivessel evaluation. J. Am. Coll. Cardiol. 55, 2816–2821 (2010).
Park, S. J. et al. Visual-functional mismatch between coronary angiography and fractional flow reserve. JACC Cardiovasc. Interv. 5, 1029–1036 (2012).
Toth, G. et al. Evolving concepts of angiogram: fractional flow reserve discordances in 4000 coronary stenoses. Eur. Heart J. 35, 2831–2838 (2014).
Kang, S. J. et al. Sex differences in the visual-functional mismatch between coronary angiography or intravascular ultrasound versus fractional flow reserve. JACC Cardiovasc. Interv. 6, 562–568 (2013).
Adjedj, J. et al. Visual and quantitative assessment of coronary stenoses at angiography versus fractional flow reserve: The impact of risk factors. Circ. Cardiovasc. Imaging 10(7), e006243 (2017).
Adjedj, J., Stoyanov, N. & Muller, O. Comparison of coronary angiography and intracoronary imaging with fractional flow reserve for coronary artery disease evaluation: An anatomical-functional mismatch. Anatol. J. Cardiol. 20, 182–189 (2018).
Neumann, F. J. et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 40, 87–165 (2019).
Pijls, N. H. & Sels, J. W. Functional measurement of coronary stenosis. J. Am. Coll. Cardiol. 59, 1045–1057 (2012).
De Bruyne, B. et al. Fractional flow reserve-guided PCI for stable coronary artery disease. N. Engl. J. Med. 371, 1208–1217 (2014).
Jeremias, A., Kirtane, A. J. & Stone, G. W. A test in context: Fractional flow reserve: accuracy, prognostic implications, and limitations. J. Am. Coll. Cardiol. 69, 2748–2758 (2017).
Yonetsu, T. et al. Significance of microvascular function in visual-functional mismatch between invasive coronary angiography and fractional flow reserve. J. Am. Heart Assoc. 6(6), e005916 (2017).
Toth, G. G. et al. Standardization of Fractional Flow Reserve Measurements. J Am Coll Cardiol. 68, 742–753 (2016).
Pijls, N. H., Tanaka, N. & Fearon, W. F. Functional assessment of coronary stenoses: Can we live without it?. Eur. Heart J. 34, 1335–1344 (2013).
Layland, J., Carrick, D., Lee, M., Oldroyd, K. & Berry, C. Adenosine: Physiology, pharmacology, and clinical applications. JACC Cardiovasc. Interv. 7, 581–591 (2014).
Matsumoto, H. et al. Feasibility of intracoronary nicorandil for inducing hyperemia on fractional flow reserve measurement: Comparison with intracoronary papaverine. Int. J. Cardiol. 314, 1–6 (2020).
Matsumoto, H. et al. Effect of caffeine on intravenous adenosine-induced hyperemia in fractional flow reserve measurement. J. Invasive Cardiol. 26, 580–585 (2014).
Matsumoto, H. et al. Is caffeine abstention necessary before adenosine-induced fractional flow reserve measurement?. J. Am. Coll. Cardiol. 66, 1943–1945 (2015).
Tanaka, H.et al. Linear concentration-response relationship of serum caffeine with adenosine-induced fractional flow reserve overestimation: a comparison with papaverine. EuroIntervention. 17(11), e925–e931 (2021).
Wilson, R. F., Wyche, K., Christensen, B. V., Zimmer, S. & Laxson, D. D. Effects of adenosine on human coronary arterial circulation. Circulation 82, 1595–1606 (1990).
Wilson, R. F. & White, C. W. Intracoronary papaverine: An ideal coronary vasodilator for studies of the coronary circulation in conscious humans. Circulation 73, 444–451 (1986).
Seto, A. H., Tehrani, D. M., Bharmal, M. I. & Kern, M. J. Variations of coronary hemodynamic responses to intravenous adenosine infusion: Implications for fractional flow reserve measurements. Catheter Cardiovasc. Interv. 84, 416–425 (2014).
Mizukami, T. et al. Duration of hyperemia with intracoronary administration of papaverine. J. Am. Heart Assoc. 10, e018562 (2021).
Johnson, N. P. et al. Repeatability of fractional flow reserve despite variations in systemic and coronary hemodynamics. JACC Cardiovasc. Interv. 8, 1018–1027 (2015).
De Luca, G., Venegoni, L., Iorio, S., Giuliani, L. & Marino, P. Effects of increasing doses of intracoronary adenosine on the assessment of fractional flow reserve. JACC Cardiovasc. Interv. 4, 1079–1084 (2011).
Serruys, P. W. et al. Assessment of the SYNTAX score in the syntax study. EuroIntervention 5, 50–56 (2009).
Gould, K. L. & Lipscomb, K. Effects of coronary stenoses on coronary flow reserve and resistance. Am. J. Cardiol. 34, 48–55 (1974).
Gould, K. L. et al. Frequency and clinical implications of fluid dynamically significant diffuse coronary artery disease manifest as graded, longitudinal, base-to-apex myocardial perfusion abnormalities by noninvasive positron emission tomography. Circulation 101, 1931–1939 (2000).
De Bruyne, B. et al. Abnormal epicardial coronary resistance in patients with diffuse atherosclerosis but “Normal” coronary angiography. Circulation 104, 2401–2406 (2001).
van de Hoef, T. P. et al. Non-hyperaemic coronary pressure measurements to guide coronary interventions. Nat. Rev. Cardiol. 17(10), 629–640 (2020).
Kim, H. Y. et al. Physiological severity of coronary artery stenosis depends on the amount of myocardial mass subtended by the coronary artery. JACC Cardiovasc. Interv. 9, 1548–1560 (2016).
Gotberg, M. et al. The evolving future of instantaneous wave-free ratio and fractional flow reserve. J. Am. Coll. Cardiol. 70, 1379–1402 (2017).
Lindstaedt, M. et al. Adenosine-induced maximal coronary hyperemia for myocardial fractional flow reserve measurements: Comparison of administration by femoral venous versus antecubital venous access. Clin. Res. Cardiol. 98, 717–723 (2009).
Kitkungvan, D. et al. Quantitative myocardial perfusion positron emission tomography and caffeine revisited with new insights on major adverse cardiovascular events and coronary flow capacity. Eur. Heart J. Cardiovasc. Imaging. 20, 751–762 (2019).
Dorbala, S. et al. Single photon emission computed tomography (spect) myocardial perfusion imaging guidelines: Instrumentation, acquisition, processing, and interpretation. J. Nucl. Cardiol. 25, 1784–1846 (2018).
Knuuti, J. et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur Heart J. 41(3), 407–477 (2019).
Adjedj, J. et al. Significance of intermediate values of fractional flow reserve in patients with coronary artery disease. Circulation 133, 502–508 (2016).
Kubo, T. et al. Retrospective comparison of long-term clinical outcomes between percutaneous coronary intervention and medical therapy in stable coronary artery disease with gray zone fractional flow reserve- comfortable retrospective study. Circ J. 82, 3044–3051 (2018).
Greenbaum, A. B. et al. Comparison of medicine alone, coronary angioplasty, and left internal mammary artery-coronary artery bypass for one-vessel proximal left anterior descending coronary artery disease. Am. J. Cardiol. 86, 1322–1326 (2000).
Author information
Authors and Affiliations
Contributions
Contributions of authors: H.M., conception, design, data collection, analysis of data, and drafting the manuscript; R.M., data collection, analysis of data; S.H., analysis of data, critical revision of the manuscript; H.T., data collection, analysis of data; S.K., data collection, analysis of data; H.T. data collection, analysis of data; T.S., critical revision of the manuscript, and final approval of submission. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Matsumoto, H., Masaki, R., Higuchi, S. et al. Impact of overestimation of fractional flow reserve by adenosine on anatomical–functional mismatch. Sci Rep 12, 14962 (2022). https://doi.org/10.1038/s41598-022-19330-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-022-19330-1
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
