
Abstract
Purpose
The true disease status of a population with suspected microbial keratitis (MK) cannot be verified. There is not an accurate (gold) reference standard to confirm infection and inter-test comparisons of sensitivity and specificity therefore lead to bias with questionable estimates of test utility. We present an alternative method to report results.
Methods
We used a decision to treat as the definition for MK. We retrospectively compared the results of corneal culture and polymerase chain reaction (PCR) as these are objective tests available for the three principal groups of pathogens. We then estimated the potential contribution of positive results, either alone or in combination, to support the working diagnosis.
Results
We included 2021 (77.4%) eyes with suspected bacterial keratitis, 365 (14.0%) with suspected acanthamoeba keratitis, and 226 (8.6%) with suspected fungal keratitis, all treated between July 2013 and December 2019. In these groups, there were 51.6% positive culture and 6.5% positive PCR results for bacteria, 19.0% and 40.5% for acanthamoeba, and 28.3% and 15.0% for fungi. Between groups the differences in the proportions of positive results from culture and PCR was statistically significant (P < 0.001). The added benefit of PCR to the result of culture in identifying a potential pathogen was 1.4% for bacteria (P = 0.6292), 24.4% for acanthamoeba (P = 0.0001), and 5.8% for fungi (P = 0.3853).
Conclusions
For suspected MK a comparison of the test positivity rate is an easily comprehensible outcome measure of test utility.
Similar content being viewed by others

Introduction
Microbial keratitis (MK) is infection of the cornea by bacteria, acanthamoeba or fungi. The proportions of these pathogens that are isolated from culture vary markedly between geographic areas, with fungi more prevalent in tropical regions [1,2,3,4,5]. A diagnosis of MK is based on multiple contributory data such as environmental risk (e.g. trauma, contact lens wear), clinical signs, the results of investigation and, less frequently, the response to therapy. Clinical signs can suggest the type of pathogen, particularly fungal or parasitic infection [6,7,8], but are unreliable for distinguishing the sub-types of bacterial infection [9]. Options for investigations include stains (e.g. Gram, Grocott, calcofluor white), culture on nutrient media, and molecular techniques such as polymerase chain reaction (PCR). Corneal culture can also be used to determine the sensitivity of an isolate to relevant antimicrobials [10, 11]. In vivo confocal microscopy (IVCM) can directly visualise acanthamoeba and fungi, although the accuracy is observer dependent [12,13,14], but bacteria, except for chains of Nocardia spp., are too small to be identified [15].
The relative accuracy of investigations for suspected MK is uncertain. The usual approach to assess this problem is to designate one test as a reference and then compare the positive and negative results obtained with a second test to give sensitivity and specificity values. For example, a positive culture (or IVCM for acanthamoeba or fungi) could be designated as the reference test, with PCR used as the comparison [16, 17]. The reference test is often called a gold standard, although this implies a test that is error-free with close to 100% sensitivity and specificity [18]. However, all investigations for MK have error rates that cannot be quantified, and the term reference standard rather than gold standard is recommended. Even then, in the absence of a reliable reference standard, presenting specificity and predictive values without a consideration of the limitations and potential sources of error is incorrect.
The purpose of this study is to compare the role of two investigations in the management of suspected MK. Rather than adopt one test as a reference standard we used the decision to treat as the working clinical diagnosis and then calculated the proportions of the two tests that were positive—the test positivity rate. An assumption is that the identification of any microbe by culture or PCR from a case of suspected MK is potentially significant, and that there are therefore no false positives. We have compared corneal culture and PCR because these are objective tests that are available for bacteria, fungi and acanthamoeba, with limited scope for observer error affecting the results. For cases that had tests performed multiple times over the course of a disease episode, we adopted the clinically relevant approach of giving priority to a positive result as this usually carries greater weight than a negative result for further clinical management [19].
Materials and methods
The Moorfields Institutional Review Board approved the study as an audit of clinical care that adhered to the tenets of the Declaration of Helsinki. We identified patients from the electronic patient record who were seen between July 2013 and December 2019 who had a topical antimicrobial prescribed hourly for keratitis. Briefly, the recommended first line therapies include levofloxacin 0.5% or moxifloxacin 0.5% for suspected bacterial keratitis, polyhexanide (PHMB) 0.02% for suspected acanthamoeba keratitis, and natamycin 5% or amphotericin 0.15% for suspected fungal keratitis. A case was defined as an eye treated hourly with an antimicrobial for keratitis that also had corneal culture and a PCR test. Eyes that had only one test or neither test were excluded and cases that had therapy for multiple indications (e.g. an antibiotic with an antifungal) were included in both the relevant groups. The various clinical signs (e.g. infiltrate, ulceration) that contributed to the initial decision to treat were not available. Any uncertainty about the primary indication for treatment (e.g. chlorhexidine prescribed for suspected acanthamoeba or fungal infection) was resolved by a review of the clinical records. We adopted a nominal interval for an episode of infection of fourteen days for suspected bacterial keratitis and three months for suspected acanthamoeba or fungal keratitis. Within these intervals we aggregated the investigation results, with a positive culture or PCR result given priority, to give a single positive or negative culture or PCR result for each disease episode. To reduce the risk of duplication of pathogens, analysis was limited to the first episode of keratitis per individual. Multiple different isolates were polymicrobial infections, whereas multiple isolates of the same organism during an episode of infection were considered as one isolate. To address the issue of potential bacterial contaminants, any isolate from solid agar or liquid enrichment media was significant, and any organism detected by PCR was also considered significant. We then performed a secondary analysis with exclusion of the culture and PCR results from possible ‘non-pathogens’ as defined by a medical microbiologist. Cultures from contact lenses or contact lens solutions were also excluded.
Corneal sample culture
Samples were collected by clinicians who had appropriate training. The hospital protocol recommends the use of the bent tip of a 21 G hypodermic needle to obtain a small biopsy of material, or to use a swab. Separate samples were directly inoculated onto blood agar, Sabouraud agar, and two enrichment media (Robertson’s Cooked Meat and Brain Heart Infusion) and sent for analysis (The Doctors Laboratory, London). The liquid media was sub-cultured on day five and incubated for a further 48 h. Bacterial isolates were usually identified using matrix-assisted laser desorption ionisation time-of-flight (MALDI-TOF) mass spectrometry (Bruker, Bremen, Germany). For suspected acanthamoeba infection samples were inoculated on non-nutrient agar, subsequently flooded with a heavy suspension of E.coli (about 4 McFarland) and then kept for 7 days at 30 oC and read finally at 7 days. Speciation of acanthamoeba was not performed. Mycology samples were incubated for 7 days at 35–37 oC, with positive samples sent to the National Reference Laboratory (Bristol) for species confirmation.
Specimen DNA extraction for PCR
Samples for PCR were collected with either a hypodermic needle or swab and sent for processing (Micropathology Ltd, Coventry, UK). Genomic DNA extraction was performed by re-suspending dry swabs or scrapes in 650 µl of nuclease free water (Severn Biotech). Each specimen was frozen for 10 minutes at −70 oC. Subsequently, a 200 µl aliquot was taken and added to lysozyme (25 µL at 100 mg/mL) and lysostaphin (10 µL at 1 mg/mL) and incubated for 30 min at 37 oC. An aliquot of 40 µl of Proteinase K was added with 200 µl of Lysis buffer and subjected to heat-treatment according to manufacturer’s instructions (Qiagen). Nucleic acid was extracted using the QiaSymphony Bio-Robot (Qiagen) and the QiaSymphony DSP DNA Mini Kit according to manufacturer’s instructions with a final DNA eluate of 200 µl.
Bacterial 16 S DNA assay
A single-round amplification was performed using the primers 8 f (ref. [20]) and a modification of the 533 R primer [21]. Each reaction mix consisted of 14 µl of 2 x MyTaq Mix (Meridian scientific), 0.5 µl of Evagreen Sybr Green (BIOTIUM), 5 µl of Nuclease free water (Severn Biotech) and 1 µM of the forward and reverse primers, to this mix a 5 µl aliquot of extracted DNA was added. The reaction mixes were subjected to thermal cycling on a Magnetic Induction real-time cycler with a programme of initial heating for 95 °C for 1 min 45 s, followed by 30 cycles of 95 °C for 20 s, 55 °C for 20 s and 72 °C for 20 s.
Acanthamoeba DNA detection by PCR
Semi-nested amplification was performed using a modification of the primers of Dhivya et al (2007) [22]. Each first round reaction mixture contained 1 x PCR Buffer, 1.5 mM MgCl2, 0.1 mM dNTPs, 1U Supertherm Taq Polymerase (LPI, UK) and 0.5 µM of the following primers: Acanthamoeba F, GGCCCAGATCGTTTACCGTGAA and Acanthamoeba Rb, TCT CAC AAG CTG CTR GGG GAG TCA. In the following second round reaction a 1 µl aliquot of first round reaction is added to a second round reaction mix that contained 1 x PCR Buffer, 1.5 mM MgCl2, 0.1 mM dNTPs, 1U Supertherm Taq Polymerase (LPI, UK) and 0.5 µM of the following primers: Acanthamoeba F2: AACGATGCCGAC CAGCGATTA and Acanthamoeba Rb: TCTCACAAGCTGCTRGGGGAGTCA. Both first and second round reaction mixes were subjected to thermal cycling on a programme of initial heating for 95 °C for 1 min 45 s, followed by 30 cycles of 95 °C for 20 s, 60 °C for 20 s and 72 °C for 20 s. PCR reactions were electrophoresed through a 3% agarose gel containing ethidium bromide and bands were visualised by UV transillumination.
Pan fungal DNA assay
A single-round amplification was performed using primers as described by Lau et al. (2007) [23]. Each reaction mix consisted of 25 µl of 2 x MyTaq Mix (Meridian scientific), 5 µl of Nuclease free water (Severn Biotech) and 1 µM of the forward and reverse primers, to this mix a 20 µl aliquot of extracted DNA was added. The reaction mixes were subjected to thermal cycling with a programme of initial heating for 95 °C for 1 min 45 s, followed by 40 cycles of 95 °C for 20 s, 60 °C for 20 s and 72 °C for 20 s. PCR reactions were electrophoresed through a 3% agarose gel containing ethidium bromide and bands were visualised by UV transillumination.
Bacterial 16 S and fungal 18 S rRNA gene sequencing
The amplicons from positive reactions were cleaned using an equal volume of SureClean (Bioline) according to manufacturer’s instructions. The amplicons were subsequently subjected to Sanger Sequencing using an ABI 3130XL instrument according to manufacturer’s instructions (Applied Biosystems).
Statistical analysis
For each group with a working diagnosis of bacterial, fungal and acanthamoeba keratitis the proportions with positive or negative culture and PCR results were recorded. For suspected bacterial keratitis the analysis was repeated for cases categorised by a clinical microbiologist (SD) as an isolate with high pathogenicity, or as an isolate that is rarely present as a contaminant, i.e. fastidious organisms and obligate anaerobes. Fisher’s exact test was used to compare proportions positive by groups.
Results
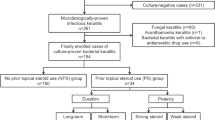
We identified 11,979 prescriptions for the hourly use of an antibiotic (excluding post-refractive surgery prophylaxis), 610 prescriptions for anti-amoebic therapy, and 347 prescriptions for antifungal therapy. We then filtered for unique eyes with a diagnosis of keratitis that had investigation with both corneal culture and PCR, which yielded 2612 cases with a working clinical diagnosis of MK, comprising 2021 (77.4%) eyes with suspected bacterial keratitis, 365 (14.0%) eyes with suspected acanthamoeba keratitis, and 226 (8.6%) eyes with suspected fungal keratitis. For these eyes the positive results from investigation for suspected bacterial keratitis were 51.6% for culture and 6.5% for PCR, for suspected acanthamoeba keratitis positive results were 19.0% for culture and 40.5% for PCR, and for suspected fungal keratitis the positive results were 28.3% for culture and 15.0% for PCR (Table 1). The differences in proportions between groups was statistically significant (P < 0.001). The added benefit of using PCR as an addition to culture (i.e. PCR was positive when culture was negative) was 1.4% for bacteria (P = 0.6292), 24.4% for acanthamoeba (P = 0.0001), and 5.8% for fungi (P = 0.3853). Conversely, the added benefit of using culture as an addition to PCR (i.e. culture was positive when PCR was negative) was 46.6% for bacteria (P = 0.0001), 2.7% for acanthamoeba (P = 0.6343) and 19.0% for fungi (P = 0.0003). Both investigations were negative in 47.0% of suspected bacterial keratitis cases, 56.7% of suspected acanthamoeba cases, and 65.9% of fungal cases (Table 1 and Fig. 1). When comparing all bacterial cultures with the result following exclusion of suspected non-pathogens, 1044 (51.6%) of all bacterial samples were culture positive with 131 (6.5%) positive by PCR, but this difference was reduced to 487 (36.1%) culture positive compared with 105 (7.8%) PCR positive when ‘non-pathogens’ were excluded (Table 1 and Fig. 1). The difference in proportions between results for these two groups was statistically significant (P < 0.001). Finally, PCR was negative in 90.1% of cases of culture positive bacterial keratitis (84.0% when only bacterial pathogens were included), 14.5% of cases of culture positive acanthamoeba keratitis, and 67.2% of cases of culture positive fungal keratitis.

Bar graph of the proportions of the four combinations of results from investigation by culture and PCR from, (1) 2021 cases with a working diagnosis of bacterial keratitis, (2) 1450 cases with a working diagnosis of bacterial keratitis from which a pathogenic bacterium was isolated, (3) 365 cases with a working diagnosis of acanthamoeba keratitis, and (4) 226 cases with a working diagnosis of fungal keratitis. Numbers are the percentage of the total cases for each of the four groups 1–4.
The characterisation of the 1210 bacterial isolates from 1044 positive cultures are shown in Supplementary Table 2 categorised as Gram positive or Gram negative isolates, with the bacteria considered as ‘probable pathogens’ for the purposes of this study highlighted in red text. The 112 fungal isolates that were identified from culture are shown in Supplementary Table 3, grouped as filamentary fungi or yeasts. A total of 104 bacterial samples were identified from both culture and by 16 S rRNA gene sequencing; 29 (27.9%) were concordant for only the genus, a further 53 (51.0%) were concordant at species level, but for 22 (21.2%) the results from the two methods were different. None of the bacteria identified by 16 S rRNA gene sequencing are difficult bacteria to culture. A total of 21 fungal samples were identified by both culture and 18 S rRNA gene sequencing; 4 (19%) were concordant for the genus, with a further 16 (76.2%) at the species, while in 1 (4.8%) the result from the two methods were different.
Discussion
Several sources of information can contribute to a diagnosis of MK, but the initial decision to start empiric therapy is usually based on the history and clinical signs. Investigation can then either support the management decision or indicate a change in therapy, with the expectation that this improves outcomes. However, both culture and PCR are susceptible to false negative error. Without an error-free reference standard the proportions of true or false negatives are unknown and this data cannot contribute to an assessment of the test accuracy [24,25,26]. An inter-test comparison of sensitivity and specificity based on a case definition of one or more positive investigations would also exclude cases in which all investigations were negative, leading to an overestimate of the ability of the test to detect infection [27, 28]. To address the problem of a lack of a ground truth for the diagnosis of corneal infection we have adopted a practical approach of using the decision to treat as the case definition, which reflects clinical practice and has the advantage that it includes all the potential cases of MK [24, 29,30,31]. We then compared the numbers of the results that supported the working diagnosis [32]. Even with this method, a persistent unresolved problem is confirmation bias due to a positive test result having greater weight than a negative result [33]. For MK it is also very likely that there is a correlation between the results of culture and PCR because some mechanisms causing test error (e.g. an inadequate sample, contamination) are common to both. This complicates some statistical comparisons of test outcomes such as latent class analysis, which assumes that the results of any two investigations are independent [34, 35]. Should a comparison be required for prospective studies, the level of agreement, or concordance between the working clinical diagnosis and the tests, are alternatives [36, 37]. Ultimately, rather than just the results of the tests, it is the impact that these investigations have on decision making and outcomes that should be reported.
Our results confirm that in suspected MK culture and PCR are often both negative (bacteria 47.0%, acanthamoeba 56.7%, fungi 65.6%), which indicates either a low detection rate for the tests, a low threshold for starting treatment, or a high prevalence of ulcerative keratitis that is not the result of microbial infection (sterile keratitis). The exclusion of cases that were treated but were not fully investigated probably means that even these figures for investigation-negative cases are likely to be an underestimate. Previous studies report a wide range of positive results from culture and PCR, which may reflect differences in the study inclusion criteria or variations in the ability of the tests to detect a pathogen, but this variation also makes interpretation of the utility of the tests problematic. For example, the reported ranges for positive results are 23–53% for bacterial culture and 26–46% for bacterial PCR [24, 29, 38,39,40,41,42,43,44], 7–55% for acanthamoeba culture and 12–94% for acanthamoeba PCR [16, 27, 45,46,47,48], and 25–68% for fungal culture and 37–93% for fungal PCR [24, 25, 30, 49,50,51,52,53,54,55,56]. Of note, the proportion of our cases positive with a validated bacterial PCR assay (6.5%) was markedly lower than previous studies that have used a positive culture as a reference standard. We also confirmed that the results from culture and PCR were not concordant (Table 1 and Fig. 1) as there were numerous instances when either culture or PCR was positive when the other test was negative, or when different organisms were identified. For suspected bacterial or fungal keratitis, the culture was often positive when PCR is negative [25, 54, 57], while, conversely, for suspected acanthamoeba keratitis the PCR was often positive when culture was negative. Others have confirmed a greater benefit of PCR for suspected acanthamoeba keratitis [24, 26, 28, 39, 57,58,59], although there are also reports where PCR was more sensitive than culture for suspected bacterial keratitis [24, 38, 57], or fungal keratitis [24, 25, 51, 52, 56, 57]. In our study, the difference between pathogen groups may be due in part to the assay employed. As gene sequencing was not performed for acanthamoeba a two-stage amplification can be used, which is likely to be more sensitive than the one stage amplification used for the pan-bacterial 16 S or pan-fungal 18 S assays. Two-stage amplification is not suited to bacterial or fungal PCR due the high risk of amplification of environmental contaminants, which would in turn impair the ability to perform a meaningful analysis for sequenced amplification products. Concordance between the result from culture and gene sequencing at the species level was better for fungi than bacteria, with 51.0% concordant for bacteria compared with 76.2% for fungi, which is similar to previous reports of 54% for bacteria and 89–92% for fungi [24, 29, 50]. This level of concordance is lower than has been reported for systemic infections, possibly because of contamination of the corneal samples by ocular surface flora [24, 29, 38]. With a high level of discordant results, deciding which of the two organism is the ‘true positive’ is currently impossible. Finally, we confirmed that at our tertiary referral centre acanthamoeba and fungi are still relatively uncommon causes for MK, but with proportions consistent with an increase in acanthamoeba and fungal infections in the last decades associated with contact lens wear [60,61,62,63].
Several variables can affect the results of corneal culture and PCR. Larger lesions are thought to have a greater microbial load, with higher DNA copy numbers, and more likely concordant for culture and PCR, while pre-treatment with a broad spectrum topical antimicrobial reduces the bacterial load [38, 39]. For PCR the sensitivity (ability to detect microbial DNA) may depend on the primers that are used [49], but more sensitive techniques such as real time PCR are not widely available for routine clinical use [16, 38, 47, 64, 65]. Perversely, although PCR has the potential to identify uncultured, dead, or unusual organisms [24, 30, 50, 66], an increased sensitivity may also make it more difficult to distinguish pathogens from contaminants [24]. Strategies to exclude microbes identified as part of the normal surface microbiome include ignoring isolates that are only cultured in enrichment broth or excluding organisms considered microbiologically to be non-pathogens, while PCR isolates with only one electrophoretic gel band may be excluded [29]. However, the definition of potential pathogens can change [67, 68], for example with the inclusion of aerobic, nonfermenting gram-negative rods Achromobacter xylosoxidans and Stenotrophomonas maltophilia [69, 70], and some coagulase negative Staphylococci such as Staphylococcus warneri and Staphylococcus pasteuri [10]. Because some probable pathogens in our study (e.g. Pseudomonas aeruginosa) were sometimes only isolated from enrichment broth, our strategy was to consider all bacterial isolates as a potential pathogen, but then to repeat the analysis following exclusion of potential non-pathogens. Interestingly, this strategy showed that the bacterial pathogen group was more likely to be culture negative and PCR positive.
The limitations of this retrospective study are that the use of a decision to treat as the case inclusion criterion probably has a low threshold for intervention because of the low risk of treatment with an antimicrobial compared to the adverse consequences of mistaken inaction. Second, the investigations may not have been applied systematically, as small ulcers are less likely to be investigated as they are often culture negative with a good outcome [12, 24, 42, 43]. There may also have been a preference to selectively perform the test most likely to give a positive result rather than perform both tests, with the patient excluded from the study. Importantly, as with previous publications, we could not estimate how good the tests were at discriminating between the presence or absence of infection. Finally, our results relate to clinical management within a large specialist hospital in the UK, and it is likely that the proportions of results vary across different catchment populations.
In conclusion, most patients with suspected MK are treated empirically with an antimicrobial, either without testing or before the results of tests are available. The result of culture or PCR should then indicate whether the treatment is adequate or whether an alternate therapy is required [71]. However, despite management guidelines for MK, it is unclear how often investigation triggers a change in management, and any difference in outcome between empirical treatment or therapy guided by investigation has not been quantified [72,73,74]. We have confirmed that culture and PCR are additive tests and not alternatives, with culture also used to determine the likely in vitro sensitivity of an isolate to antimicrobials, which cannot be assessed by PCR [38, 68, 72]. In our experience the speed advantage of PCR compared to culture for most bacteria is exaggerated when this is solely based on the cycle time for PCR without consideration of laboratory working practises [39, 56]. However, for slow growing bacterial isolates, and for acanthamoeba and fungi, the relative speed of PCR can still be an advantage [75]. Finally, because the proportions of true positive, true negative, false positive or false negative results cannot be reliably estimated in a population with suspected MK, we recommend that the working diagnosis, preferably based on an expert consensus to start treatment, should be the reference point for recruitment because it is a readily identifiable parameter that will include all the result options from subsequent investigations. We have then shown that the proportions of positive results, considered either singly or in combination and expressed as a percentage, is a simple and easily comprehensible outcome measure. How often these results then actually affect management and outcomes should be the focus of further research.
Summary table
What was known before
-
The role of investigation for the management of microbial keratitis (MK) is uncertain.
-
Corneal culture and polymerase chain reaction are imprecise when applied to MK with no accurate reference standard to compare test utility.
-
This has led to the use of statistical methods that overestimate test utility.
What this study adds
-
We describe the use of the decision to treat with an antimicrobial as a clinically relevant index on which to base a comparison of the utility of investigations.
-
An advantage of this method is that the results of all investigations are included in the analysis.
-
The proportion of positive tests that could contribute to the diagnosis is then an easily understood outcome measure.
References
Hsu HY, Ernst B, Schmidt EJ, Parihar R, Horwood C, Edelstein SL. Laboratory results, epidemiologic features, and outcome analyses of microbial keratitis: a 15-year review from St. Louis. Am J Ophthalmol. 2019;198:54–62.
Sand D, She R, Shulman IA, Chen DS, Schur M, Hsu HY. Microbial keratitis in Los Angeles: the Doheny Eye Institute and the Los Angeles County Hospital experience. Ophthalmology. 2015;122:918–24.
Lichtinger A, Yeung SN, Kim P, Amiran MD, Iovieno A, Elbaz U, et al. Shifting trends in bacterial keratitis in Toronto: an 11-year review. Ophthalmology. 2012;119:1785–90.
Leck AK, Thomas PA, Hagan M, Kaliamurthy J, Ackuaku E, John M, et al. Aetiology of suppurative corneal ulcers in Ghana and south India, and epidemiology of fungal keratitis. Br J Ophthalmol. 2002;86:1211–5.
Brown L, Leck AK, Gichangi M, Burton MJ, Denning DW. The global incidence and diagnosis of fungal keratitis. Lancet Infect Dis. 2021;21:e49–57.
Thomas PA, Leck AK, Myatt M. Characteristic clinical features as an aid to the diagnosis of suppurative keratitis caused by filamentous fungi. Br J Ophthalmol. 2005;89:1554–8.
Mascarenhas J, Lalitha P, Prajna NV, Srinivasan M, Das M, D’Silva SS, et al. Acanthamoeba, fungal, and bacterial keratitis: a comparison of risk factors and clinical features. Am J Ophthalmol. 2014;157:56–62.
Jongkhajornpong P, Nimworaphan J, Lekhanont K, Chuckpaiwong V, Rattanasiri S. Predicting factors and prediction model for discriminating between fungal infection and bacterial infection in severe microbial keratitis. PLoS ONE. 2019;20:e0214076.
Dahlgren MA, Lingappan A, Wilhelmus KR. The clinical diagnosis of microbial keratitis. Am J Ophthalmol. 2007;143:940–4.
Asbell PA, Sanfilippo CM, Sahm DF, DeCory HH. Trends in antibiotic resistance among ocular microorganisms in the United States From 2009 to 2018. JAMA Ophthalmol. 2020;138:439–50.
Kaye S, Tuft S, Neal T, Tole D, Leeming J, Figueiredo F, et al. Bacterial susceptibility to topical antimicrobials and clinical outcome in bacterial keratitis. Invest Ophthalmol Vis Sci. 2010;51:362–8.
Chidambaram JD, Prajna NV, Larke NL, Palepu S, Lanjewar S, Shah M, et al. Prospective study of the diagnostic accuracy of the in vivo laser scanning confocal microscope for severe microbial keratitis. Ophthalmology. 2016;123:2285–93.
Hau SC, Dart JKG, Vesaluoma M, Parmar DN, Claerhout I, Bibi K, et al. Diagnostic accuracy of microbial keratitis with in vivo scanning laser confocal microscopy. Br J Ophthalmol. 2010;94:982–7.
Kheirkhah A, Syed ZA, Satitpitakul V, Goyal S, Müller R, Tu EY, et al. Sensitivity and specificity of laser-scanning in vivo confocal microscopy for filamentous fungal keratitis: role of observer experience. Am J Ophthalmol. 2017;179:81–9.
Vaddavalli PK, Garg P, Sharma S, Thomas R, Rao GN. Confocal microscopy for Nocardia keratitis. Ophthalmology. 2006;113:1645–50.
Lehmann OJ, Green SM, Morlet N, Kilvington S, Keys MF, Matheson MM, et al. Polymerase chain reaction analysis of corneal epithelial and tear samples in the diagnosis of Acanthamoeba keratitis. Invest Ophthalmol Vis Sci. 1998;39:1261–5.
Rampini SK, Bloemberg GV, Keller PM, Büchler AC, Dollenmaier G, Speck RF, et al. Broad-range 16S rRNA gene polymerase chain reaction for diagnosis of culture-negative bacterial infections. Clin Infect Dis. 2011;53:1245–51.
Umemneku Chikere CM, Wilson K, Graziadio S, Vale L, Allen AJ. Diagnostic test evaluation methodology: a systematic review of methods employed to evaluate diagnostic tests in the absence of gold standard - An update. PLoS ONE. 2019;14:e0223832.
Wians FH. Clinical laboratory tests: which, why, and what do the results mean? Lab Med. 2009;40:105–13.
Liu WT, Marsh TL, Cheng H, Forney LJ. Characterization of microbial diversity by determining terminal restriction fragment length polymorphisms of genes encoding 16S rRNA. Appl Environ Microbiol. 1997;63:4516–22.
Sun Z, Li G, Wang C, Jing Y, Zhu Y, Zhang S, et al. Community dynamics of prokaryotic and eukaryotic microbes in an estuary reservoir. Sci Rep. 2014;4:6966.
Dhivya S, Madhavan HN, Rao CM, Rao KS, Ramchander PV, Therese KL, et al. Comparison of a novel semi-nested polymerase chain reaction (PCR) with a uniplex PCR for the detection of Acanthamoeba genome in corneal scrapings. Parasitol Res. 2007;100:1303–9.
Lau A, Chen S, Sorrell T, Carter D, Malik R, Martin P, et al. Development and clinical application of a panfungal PCR assay to detect and identify fungal DNA in tissue specimens. J Clin Microbiol. 2007;45:380–5.
Kim E, Chidambaram JD, Srinivasan M, Lalitha P, Wee D, Lietman TM, et al. Prospective comparison of microbial culture and polymerase chain reaction in the diagnosis of corneal ulcer. Am J Ophthalmol. 2008;146:714–23.
Embong Z, Wan Hitam WH, Yean CY, Rashid NHA, Kamarudin B, Abidin SKZ, et al. Specific detection of fungal pathogens by 18S rRNA gene PCR in microbial keratitis. BMC Ophthalmol. 2008;8:7.
Pasricha G, Sharma S, Garg P, Aggarwal RK. Use of 18S rRNA gene-based PCR assay for diagnosis of acanthamoeba keratitis in non-contact lens wearers in India. J Clin Microbiol. 2003;41:3206–11.
Goh JWY, Harrison R, Hau S, Alexander CL, Tole DM, Avadhanam VS. Comparison of in vivo confocal microscopy, PCR and culture of corneal scrapes in the diagnosis of acanthamoeba keratitis. Cornea. 2018;37:480–5.
Boggild AK, Martin DS, Lee TY, Yu B, Low DE. Laboratory diagnosis of amoebic keratitis: comparison of four diagnostic methods for different types of clinical specimens. J Clin Microbiol. 2009;47:1314–8.
Somerville TF, Corless CE, Sueke H, Neal T, Kaye SB. 16S Ribosomal RNA PCR versus conventional diagnostic culture in the investigation of suspected bacterial keratitis. Transl Vis Sci Technol. 2020;9:2.
Behera HS, Srigyan D. Evaluation of polymerase chain reaction over routine microbial diagnosis for the diagnosis of fungal keratitis. Optom Vis Sci. 2021;98:280–4.
Brook RH, Lohr KN. Efficacy, effectiveness, variations, and quality. Boundary-crossing research. Med Care. 1985;23:710–22.
Mallett S, Halligan S, Thompson M, Collins GS, Altman DG. Interpreting diagnostic accuracy studies for patient care. BMJ. 2012;345:e3999.
Linnet K, Bossuyt PMM, Moons KGM, Reitsma JBR. Quantifying the accuracy of a diagnostic test or marker. Clin Chem. 2012;58:1292–301.
Alonzo TA, Pepe MS. Assessing the accuracy of a New Diagnostic Test when a gold standard does not exist. 1998 [cited 2021 Jul 17]; Available from: https://biostats.bepress.com/uwbiostat/paper156/
Albert PS, Dodd LE. A cautionary note on the robustness of latent class models for estimating diagnostic error without a gold standard. Biometrics. 2004;60:427–35.
Reitsma JB, Rutjes AWS, Khan KS, Coomarasamy A, Bossuyt PM. A review of solutions for diagnostic accuracy studies with an imperfect or missing reference standard. J Clin Epidemiol. 2009;62:797–806.
Trikalinos TA, Balion CM. Chapter 9: options for summarizing medical test performance in the absence of a “gold standard.”. J Gen Intern Med. 2012;27:S67–75.
Shimizu D, Miyazaki D, Ehara F, Shimizu Y, Uotani R, Inata K, et al. Effectiveness of 16S ribosomal DNA real-time PCR and sequencing for diagnosing bacterial keratitis. Graefes Arch Clin Exp Ophthalmol. 2020;258:157–66.
Panda A, Pal Singh T, Satpathy G, Wadhwani M, Matwani M. Comparison of polymerase chain reaction and standard microbiological techniques in presumed bacterial corneal ulcers. Int Ophthalmol. 2015;35:159–65.
Bourcier T, Thomas F, Borderie V, Chaumeil C, Laroche L. Bacterial keratitis: predisposing factors, clinical and microbiological review of 300 cases. Br J Ophthalmol. 2003;87:834–8.
McLeod SD, Kolahdouz-Isfahani A, Rostamian K, Flowers CW, Lee PP, McDonnell PJ. The role of smears, cultures, and antibiotic sensitivity testing in the management of suspected infectious keratitis. Ophthalmology. 1996;103:23–8.
Morlet N, Minassian D, Butcher J, the Ofloxacin Study Group. Risk factors for treatment outcome of suspected microbial keratitis. Br J Ophthalmol. 1999;83:1027–31.
Tan SZ, Walkden A, Au L, Fullwood C, Hamilton A, Qamruddin A, et al. Twelve-year analysis of microbial keratitis trends at a UK tertiary hospital. Eye. 2017;31:1229–36.
Peng MY, Cevallos V, McLeod SD, Lietman TM, Rose-Nussbaumer J. Bacterial Keratitis: isolated organisms and antibiotic resistance patterns in San Francisco. Cornea. 2018;37:84–7.
Yera H, Zamfir O, Bourcier T, Ancelle T, Batellier L, Dupouy-Camet J, et al. Comparison of PCR, microscopic examination and culture for the early diagnosis and characterization of Acanthamoeba isolates from ocular infections. Eur J Clin Microbiol Infect Dis. 2007;26:221–4.
Holmgaard DB, Barnadas C, Mirbarati SH, O’Brien Andersen L, Nielsen HV, Stensvold CR. Detection and identification of Acanthamoeba and other nonviral causes of infectious keratitis in corneal scrapings by real-time PCR and next-generation sequencing-based 16S-18S gene analysis. J Clin Microbiol. 2021;59:e02224–20.
Ikeda Y, Miyazaki D, Yakura K, Kawaguchi A, Ishikura R, Inoue Y, et al. Assessment of real-time polymerase chain reaction detection of Acanthamoeba and prognosis determinants of Acanthamoeba keratitis. Ophthalmology. 2012;119:1111–9.
Tu EY, Joslin CE, Sugar J, Booton GC, Shoff ME, Fuerst PA. The relative value of confocal microscopy and superficial corneal scrapings in the diagnosis of Acanthamoeba keratitis. Cornea. 2008;27:764–72.
Zhao G, Zhai H, Yuan Q, Sun S, Liu T, Xie L. Rapid and sensitive diagnosis of fungal keratitis with direct PCR without template DNA extraction. Clin Microbiol Infect. 2014;20:O776–82.
Tananuvat N, Salakthuantee K, Vanittanakom N, Pongpom M, Ausayakhun S. Prospective comparison between conventional microbial work-up vs PCR in the diagnosis of fungal keratitis. Eye. 2012;26:1337–43.
Badiee P, Nejabat M, Alborzi A, Keshavarz F, Shakiba E. Comparative study of Gram stain, potassium hydroxide smear, culture and nested PCR in the diagnosis of fungal keratitis. Ophthalmic Res. 2010;44:251–6.
Vengayil S, Panda A, Satpathy G, Nayak N, Ghose S, Patanaik D, et al. Polymerase chain reaction-guided diagnosis of mycotic keratitis: a prospective evaluation of its efficacy and limitations. Invest Ophthalmol Vis Sci. 2009;50:152–6.
Gaudio PA, Gopinathan U, Sangwan V, Hughes TE. Polymerase chain reaction based detection of fungi in infected corneas. Br J Ophthalmol. 2002;86:755–60.
Ghosh A, Basu S, Datta H, Chattopadhyay D. Evaluation of polymerase chain reaction-based ribosomal DNA sequencing technique for the diagnosis of mycotic keratitis. Am J Ophthalmol. 2007;144:396–403.
Bagyalakshmi R, Therese KL, Madhavan HN. Application of semi-nested polymerase chain reaction targeting internal transcribed spacer region for rapid detection of panfungal genome directly from ocular specimens. Indian J Ophthalmol. 2007;55:261–5.
Ferrer C, Alió JL. Evaluation of molecular diagnosis in fungal keratitis. Ten years of experience. J Ophthalmic Inflamm Infect. 2011;1:15–22.
Eleinen KGA, Mohalhal AA, Elmekawy HE, Abdulbaki AM, Sherif AM, El-Sherif RH, et al. Polymerase chain reaction-guided diagnosis of infective keratitis - a hospital-based study. Curr Eye Res. 2012;37:1005–11.
Kowalski RP, Melan MA, Karenchak LM, Mammen A. Comparison of validated polymerase chain reaction and culture isolation for the routine detection of acanthamoeba from ocular samples. Eye Contact Lens. 2015;41:341–3.
Hoffman JJ, Dart JKG, De SK, Carnt N, Cleary G, Hau S. Comparison of culture, confocal microscopy and PCR in routine hospital use for microbial keratitis diagnosis. Eye [Internet]. 2021 Nov 5; Available from: https://doi.org/10.1038/s41433-021-01812-7
Ong HS, Fung SSM, Macleod D, Dart JKG, Tuft SJ, Burton MJ. Altered patterns of fungal keratitis at a London ophthalmic referral hospital: an eight-year retrospective observational study. Am J Ophthalmol. 2016;168:227–36.
Randag AC, van Rooij J, van Goor AT, Verkerk S, Wisse RPL, Saelens IEY, et al. The rising incidence of Acanthamoeba keratitis: a 7-year nationwide survey and clinical assessment of risk factors and functional outcomes. PLoS ONE. 2019;14:e0222092.
Tuft SJ, Tullo AB. Fungal keratitis in the United Kingdom 2003–2005. Eye.2009;23:1308–13.
Ting DSJ, Ho CS, Cairns J, Elsahn A, Al-Aqaba M, Boswell T, et al. 12-year analysis of incidence, microbiological profiles and in vitro antimicrobial susceptibility of infectious keratitis: the Nottingham Infectious Keratitis Study. Br J Ophthalmol. 2021;105:328–33.
Kuo M-T, Chang H-C, Cheng C-K, Chien C-C, Fang P-C, Chang TC. A highly sensitive method for molecular diagnosis of fungal keratitis: a dot hybridization assay. Ophthalmology. 2012;119:2434–42.
De Craene S, Knoeri J, Georgeon C, Kestelyn P, Borderie VM. Assessment of confocal microscopy for the diagnosis of polymerase chain reaction-positive acanthamoeba keratitis: a case-control study. Ophthalmology. 2018;125:161–8.
Reiman DA. The identification of uncultured microbial pathogens. J Infect Dis. 1993;168:1–8.
Schabereiter-Gurtner C, Maca S, Kaminsky S, Rölleke S, Lubitz W, Barisani-Asenbauer T. Investigation of an anaerobic microbial community associated with a corneal ulcer by denaturing gradient gel electrophoresis and 16S rDNA sequence analysis. Diagn Microbiol Infect Dis. 2002;43:193–9.
Woo PCY, Lau SKP, Teng JLL, Tse H, Yuen K-Y. Then and now: use of 16S rDNA gene sequencing for bacterial identification and discovery of novel bacteria in clinical microbiology laboratories. Clin Microbiol Infect. 2008;14:908–34.
Spierer O, Miller D, O’Brien TP. Comparative activity of antimicrobials against Pseudomonas aeruginosa, Achromobacter xylosoxidans and Stenotrophomonas maltophilia keratitis isolates. Br J Ophthalmol. 2018;102:708–12.
Wiley L, Bridge DR, Wiley LA, Odom JV, Elliott T, Olson JC. Bacterial biofilm diversity in contact lens-related disease: emerging role of Achromobacter, Stenotrophomonas, and Delftia. Invest Ophthalmol Vis Sci. 2012;53:3896–905.
Rodman RC, Spisak S, Sugar A, Meyer RF, Soong HK, Musch DC. The utility of culturing corneal ulcers in a tertiary referral center versus a general ophthalmology clinic. Ophthalmology. 1997;104:1897–901.
Austin A, Lietman T, Rose-Nussbaumer J. Update on the management of infectious keratitis. Ophthalmology. 2017;124:1678–89.
McDonald EM, Ram FSF, Patel DV, McGhee CNJ. Topical antibiotics for the management of bacterial keratitis: an evidence-based review of high quality randomised controlled trials. Br J Ophthalmol. 2014;98:1470–7.
Lin A, Rhee MK, Akpek EK, Amescua G, Farid M, Garcia-Ferrer FJ, et al. Bacterial keratitis Preferred Practice Pattern®. Ophthalmology. 2019;126:1–55.
Robaei D, Carnt N, Watson S. Established and emerging ancillary techniques in management of microbial keratitis: a review. Br J Ophthalmol. 2016;100:1163–70.
Acknowledgements
The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care. ST received salary support from the Department of Health through an award made by the National Institute for Health Research to Moorfields Eye Hospital NHS Foundation Trust and the University College London Institute of Ophthalmology for a Specialist Biomedical Research Centre for Ophthalmology. CB is part funded by the National Institute for Health Research (NIHR) Biomedical Research Centre at The Royal Marsden NHS Foundation Trust and the Institute of Cancer Research, London.
Author information
Authors and Affiliations
Contributions
ST and CB performed the literature search. ST and CB were responsible for the study concept and design. ST and JT collected the data. ST, SD and JT accessed and verified the data. ST and CB performed the statistical analysis. ST, CB, SD and JT were responsible for the interpretation of the data. ST drafted the manuscript. All authors critically revised the manuscript for important intellectual content. ST was the study supervisor. All authors reviewed the manuscript and had final responsibility for the decision to submit for publication.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Tuft, S., Bunce, C., De, S. et al. Utility of investigation for suspected microbial keratitis: a diagnostic accuracy study. Eye 37, 415–420 (2023). https://doi.org/10.1038/s41433-022-01952-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-022-01952-4
This article is cited by
-
False positive fungus results from investigation of microbial keratitis
Eye (2023)
-
The diagnostic dilemma of fungal keratitis
Eye (2023)
-
Impact of implementation of polymerase chain reaction on diagnosis, treatment, and clinical course of Acanthamoeba keratitis
Graefe's Archive for Clinical and Experimental Ophthalmology (2023)
