
Abstract
Current clinical practice regarding inherited cardiac conditions has a biomedical focus, while psychological and social expertize and capacity are often lacking. As patient-centered care entails a multidisciplinary approach, the present study (a) explores barriers and facilitators of implementing patient-centered care in cardiogenetics and (b) contrasts various stakeholder viewpoints and perceived influence. We performed a three-round modified Delphi study using the input of a virtual expert panel comprising 25 medical professionals, 9 psychosocial professionals working in cardiogenetics, and 6 patient representatives. In round 1, the brainstorming phase and workshop breakout sessions were transcribed verbatim, coded and processed into unique statements listed as barriers and facilitators. In round 2, we asked the expert panel to validate, add or revise the list of barriers and facilitators. In round 3, the most relevant barriers and facilitators were ranked in importance. The experts identified 6 barriers dispersed across various levels of implementation. Having a blind spot for the patient perspective was of the highest importance, while the lack of multidisciplinary communication was ranked the lowest. We selected 9 facilitators: 2 were workflow related, 5 advocated various aspects of increased multidisciplinarity, and 2 suggested improvements in patient communication. This study revealed health system and organizational barriers and facilitators predominantly in implementing patient-centered care and only some patient-level factors. Some barriers and facilitators may be addressed easily (e.g., improving communication), while others may prove more complicated (e.g., biomedical thinking). Close interdisciplinary collaboration seems to be needed to implement PCC in cardiogenetics successfully.
Similar content being viewed by others

Introduction
The diagnosis of an inherited cardiac condition (ICC) poses the patient with a range of potential challenges. These include uncertainty, anxiety, complex treatment-related decision-making, and medically indicated lifestyle changes [1, 2]. Patients often experience multiple disease-related stressors, such as cardiac symptoms or physical restrictions. Patients may feel uncertain about their future or their family’s health, fearing sudden cardiac death or a decline in health. Genetic counseling is a communication process that helps patients and their families understand the medical and psychosocial implications of genetic testing [3]. Although the specific role of a cardiac genetic counsellor and specialized cardiac nurses have been described extensively [4,5,6], today the number of genetic counselors remains relatively small across the globe [7, 8].
Genetic testing to diagnose possible ICC is challenging, as it requires clinicians and, to a certain degree, patients to be knowledgeable about genetics [9, 10]. It also requires accurate and realistic expectations from all parties involved about the yield of genetic testing and its possibilities and limitations in disease management [5, 11].
Over the past decade, the importance of patient-centered care (PCC) has become increasingly recognized, covering three major themes: the patient experience, patient empowerment in decision-making, and building relationships between the healthcare provider(s) and the patient in care and treatment [12]. Information gathered from patient-reported outcome measures (PROMs) give insight into the patient perspective of health, and well-being. PROMs help tailor the consultation to patients’ personal needs and give them greater control over decisions and actions affecting their health and thus helps improving their quality of life (QOL) [13]. A complex disease group such as ICC requires a multifaceted approach, necessitating cardiology, genetics, medical psychology, and behavioral science [14]. However, clinical practice has a biomedical orientation, where behavioral and psychological sciences expertize and clinical capacity are often lacking. PCC focuses on patients’ health goals and guides therapeutic decisions by integrating these different perspectives into treatment modules for patients [15]. In cardiogenetics, the field that covers ICC, this would mean providing the information necessary to make a shared decision to undergo genetic testing [11] or opt for specific treatment pathways such as an implantable cardioverter-defibrillator (ICD). While this may positively influence patients’ understanding and recall of information, well-being, and overall satisfaction [16], the current clinical practice may not provide patients with enough contemplation time. In addition, many physicians may not believe they are equipped to understand thoroughly and to communicate difficult genetic results [5]. Finally, most clinicians endorse the important influence of emotional complaints, patient-reported well-being, and quality of life on medical prognosis. However, primarily generic health-related quality of life (HRQOL) instruments are used to assess disease-specific outcomes. The PROMs used to gauge the health-related quality of life in research [17,18,19] may not be ideal for routine outcome monitoring in the cardiogenetic clinic. Disease-specific measures are essential to serving the broad at-risk and patient groups.
The current study aimed to explore key barriers and facilitators for implementing PCC to improve clinical care in cardiogenetics and move the field toward PCC. We further explored differences between the stakeholders directly involved in caring for patients with ICCs (n = 34) or patient representatives (n = 6) to determine whether they experience different levels of influence regarding the identified barriers and facilitators.
Methods
Background & study design
The present study is part of a European project on developing patient-related outcome measures (PROMS) for cardiogenetics, executed with the European Rare Disease Network (ERN) GUARD-Heart. The project is a multidisciplinary, international collaboration of professionals caring for patients with a rare genetic cardiac disease and patient representatives. We performed a three-round modified Delphi study to fulfill our aims.
The Delphi study technique is an iterative feedback process and group facilitation technique that builds on ongoing data collection, created from a panel of expert stepwise input in subsequent rounds to arrive at group consensus. Experts communicate their knowledge and expertize to see how their opinions align with those of other stakeholders [20,21,22]. We modified our study design in 2 ways: panelists were not anonymous to the researcher, and we used a “ranking-type” Delphi study [21,22,23]. Figure S1 (online resource ESM_1) depicts the setup and analyses planned in the different Delphi rounds.
First, we took stock of the actual psychosocial care pathways in different European cardiogenetic centers and their use of PROMS. We then implemented four 2 h workshops that consisted of (I) information provision on the current psychosocial care status and a lecture on PCC, (II) an example of patient-reported outcomes in onco-genetics [24], (III) a case discussion, and (IV) the role of the patient organization in the care pathway. The second part of all the workshops was a brainstorming (12 focus groups) activity on implementing PCC in cardiogenetics. These focus groups comprised the first round of the Delphi study, in which we gathered opinions on the barriers and facilitators of implementing PCC in cardiogenetics. Then, in round 2, the various experts were asked to validate, add or revise the list of barriers and facilitators. We narrowed the item list in round 3 and ranked it according to importance.
Furthermore, we examined the stakeholders’ level of influence. We designed the initial online survey and the questionnaires for rounds two and three using Qualtrics XM. Data collection took place between October 2020 and September 2021.
Expert panel
Since ICC requires counseling and follow-up at the cardiology and genetic department and patients may need psychological and social guidance, we needed a multidisciplinary panel. Accordingly, we invited cardiologists, clinical geneticists, psychologists, genetic counselors, specialist nurses, and patient representatives working at or collaborating with ERN-associated cardiac centers as participants. An initial 24 ERN GUARD Heart-full members, 11 affiliated partners and 11 patient representative organizations were invited. Although there are no guidelines on the appropriate sample size for expert consensus on a Delphi forum, it is established that a minimum sample size of 10 experts (who are representative of at least three disciplines) is adequate for content validity [23, 25].
Procedure & analysis
Preparation phase: online inventory
We sent the online psychosocial care inventory (Qualtrics XM) together with the ERN GUARD-Heart newsletter via email. The survey came with an introduction letter, explaining the workshops’ objectives and study objectives. In addition to general demographics, five self-designed questions were asked about the circumstances and delivery of psychosocial care, with a yes, no-answer option and a text box to describe who provides psychosocial care.
Round 1: Brainstorming
We organized workshops on Zoom due to the COVID-19 pandemic. Per workshop, participants were divided into 3–4 breakout sessions with diverse expertize, and each session was moderated by a member of the broader project’s research team. Twelve sessions were video and audio recorded and transcribed verbatim. Several predetermined open-ended questions were asked to start discussions and prompt facilitators and barriers to implementing PCC as shown in Table S1 (online resource ESM_1).
Two authors (FeH and SVP) independently selected fragments from the session transcripts, coded them as barriers or facilitators, and classified them thematically. Disagreements were resolved by discussion or by adding a third assessor (3 instances), in which case the majority vote counted. We identified 10 fragments complicating PCC that could not be qualified as a barrier. Therefore, we added a third category of statements: General Complicating Factors (GCF). All authors agreed on the final version of the three-item lists.
Round 2: Validation
We used the barriers, facilitators and GCFs from round 1 to construct a digital questionnaire for a second round. The questionnaire contained 21 barrier statements, 28 facilitator statements, and 10 GCFs. We asked panelists to select (no limitation on total items of selection) the statements within each category they agreed with the most. The survey also included open-ended questions asking participants to add new elements or suggest alternatives and arguments for their choices. We sent 2 reminders (+1 and +3 weeks after the initial mailing). Six panelists suggested adding new items. We coded these additional items according to the round 1 procedure, resulting in a merge with already existing items.
Round 3: Narrowing down and ranking
Panelists received a personal feedback report on the results of round 2. This report compared their selected items with the group average and an invitation link to participate in round 3. We only selected items that reached the agreement threshold (40–50%). In this round, we asked the panel to rank the shorter list of barriers (6 items), facilitators (9 items) and GCFs (5 items) in order of importance on a Likert scale from 1 (most important) to 6 (least important). In addition, we asked stakeholders to indicate their level of influence on a VAS scale from 0 (no influence) to 100 (a lot of influence) for each of the barriers, facilitators and GCFs. We calculated mean ranks and their standard deviation for the barriers and facilitators for the total sample and split them by stakeholder category in SPSS 26.0.
Results
Participants
A total of 23 associated ERN-GUARD Heart centers professionals completed the inventory on psychosocial care provision. Table S2 (online resource ESM_1) provides an overview of the participants’ characteristics. In total, 40 participants subscribed for the workshops (65% females, mean age = 45 [range: 28–68], mean years working in the field = 12 [range: 2–33]). More than half of the participants were clinicians, and 22% were psychosocial healthcare workers, such as psychologists, genetic counselors, social workers, and specialized cardiac nurses. Seventy-one per cent of the participants completed round 1 (n = 28); 85% (n = 24) of those completed round 2 and 68% (n = 19) completed round 3.
Current psychosocial care provision
We found (Table 1) that psychosocial care was offered in approximately half of the centers and implemented in ICC’s care pathway. The majority (78%) assessed psychosocial needs concerning genetic testing. A psychology department or clinic provides psychosocial care in only five centers. PROMS were used to assess care needs in only one center.
Barriers and facilitators in implementing PCC in cardiogenetics
Round 1 (i.e., the brainstorming sessions) resulted in a list of 58 barrier statements and 49 facilitator statements, which we reduced after a duplicate check to a final list of 21 barrier statements, 28 facilitators and 10 statements expressing GCFs as shown in Table S3 (online resource ESM_2). Table 2 describes 6 barriers acknowledged by at least 50% of the experts (round 2), ranked in order of importance (round 3). Barriers were themed around the current biomedical care orientation, various aspects of lack of knowledge about ICC, workflow issues (such as concerns that working patient-centered will take up too much time, and how to organize follow-up care), and lack of communication. A blind spot for the patient perspective was of the highest importance, while the lack of communication between the various departments was ranked the lowest. Table 3 shows 9 selected facilitators acknowledged by at least 50% of our experts. Two were workflow related, five advocated various aspects of increased multidisciplinarity, and two suggested improvements in patient communication.
General complicating factors (GCFs) in implementing PCC in cardiogenetics
Four generally complicating factors were selected and acknowledged by at least 45% of the experts. Items may not be qualified as a barrier or facilitator but predominantly reflect the complexity of having a rare genetic cardiac disease, with needs dependent on the patients’ life stage. Table 4 shows the endorsement and ranking of the four GCFs. As the most important complicating factor, difficulties with disclosing diagnosis and disease risk to the family were chosen, followed by a general lack of awareness about the role of psychosocial factors and care in these patients.
Barriers and facilitators per profession
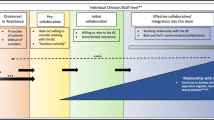
Figures 1, 2 display the 6 most significant barriers and 9 most essential facilitators for each stakeholder group. We observed differences between the stakeholder groups. The most crucial barrier lies at the patient level from the medical professional’s perspective. Clinicians question whether patients understand their information well enough to make an informed decision. Patient representatives and psychosocial professionals rank patient health illiteracy lower in positions 4 and 5, respectively. On the other hand, according to the psychosocial professionals and the patient representatives, the most significant barrier was the biomedical orientation of the current outcome assessment and the neglect of patient-reported outcomes. Clinicians rank this barrier as fourth, attaching substantially less importance.

This figure displays the six derived barriers to implementing patient-centered care in cardiogenetics for the three different stakeholder groups. For easier comparison, we have colored the cells, using the same colors for the same barrier. Yellow = workflow, Green = communication, Orange = biomedical orientation, Blue = lack of knowledge. The cells contain the following information per perspective: theme – ‘statement’ mean rank (SD). The term psychosocial worker encompasses psychologists, genetic counselors, social workers, and specialized cardiac nurses working in a cardiac genetic center.

This figure displays the nine derived facilitators to implement patient-centered care in cardiogenetics for the three different stakeholder groups. For easier comparison, we have colored the cells, using the same colors for the same facilitators. Yellow = workflow; Green = communication; Blue = multidisciplinary work. The cells contain per perspective: theme – ‘statement’ mean rank (SD). The term psychosocial worker encompasses psychologists, genetic counselors, social workers, and specialized cardiac nurses working in a cardiac genetic center.
An essential helping factor, according to the medical and psychosocial professionals’ perspective, was the multidisciplinary management of patients through sustained collaboration between the different departments involved in caring for patients with ICC. In addition, a structured assessment of the psychosocial needs of patients followed by an interdisciplinary discussion before decision-making on genetic testing would facilitate PCC according to both professional groups. These two facilitators are deemed less critical from the patient representatives’ perspective. In their view, the presence of a psychosocial worker dedicated to the cardio-genetic department would be the most helpful factor toward more patient-centered health care and starting conversations with patients about themselves. Other discrepancies between stakeholder groups became apparent, e.g., regarding the discussion of risk stratification choices and therapeutic consequences with the patient (relatively unpopular with clinicians) and the role of research programs (undesirable with patient representatives and psychosocial professionals).
General complicating factors (GFCs) per profession
Figure 3 displays the four most significant GFCs ranked separately for each stakeholder group. An essential factor indicated by physicians and psychosocial workers is the factor ‘illness complexity’-people with different lifestyles have different needs at cardiogenetic consultation. Patient representatives rank ‘lack of insight’ as a lack of awareness that psychosocial care is needed, as the most influential factor was hindering the implementation of PCC.

This figure displays the four derived general complicating factors (GFC) to implement patient-centered care in cardiogenetics for the three different stakeholder groups. For easier comparison, we have colored the cells, using the same colors for the same GCFs. Yellow = illness complexity, Green = patient needs, Blue = lack of insight. The cells contain the following information per perspective: theme – ‘statement’ mean rank (SD). The term psychosocial worker encompasses psychologists, genetic counselors, social workers, and specialized cardiac nurses working in a cardiac genetic center.
Level of influence
Figure 4 displays the level of influence of the three stakeholder groups on the 6 barriers and 9 facilitators. For the barriers, the level of influence was relatively moderate, with most estimated influences lying between 40 and 60%. Several results stood out. Patient representatives indicated considerable influence on assessing patient functioning and outcomes (84%). Likewise, they noted a significant impact on patient health literacy (82%). Patient representatives indicated the lowest influence on the perceived lack of time professionals have for PCC (37%). Psychosocial professionals estimated their influence on the perceived lack of time to work patient-centered and the uncertainty due to varying penetrance and variable expression of ICC to be the lowest (both 35%). Medical professionals felt most influential in improving patients’ health illiteracy (61%) and improving communication between departments (63%).

This figure displays mean level of influence (%), and the error bars reflect the standard error of the mean. We used the resulting overarching barriers and facilitators as input variables for the level of influence questions.
Generally, we found a more diverse picture in the facilitators than in the barriers, with larger standard deviations and most prominent in the opinions of patient representatives. For 7 out of 9 facilitators, patient representatives were pointed out to have little influence (<38%). Clinicians felt they could exert more influence on facilitators than barriers, with 6 out of 9 facilitators rated above 60%. Medical professionals estimated that they would have the most impact on being more open and transparent in communicating with patients and increasing collaboration across departments and disciplines. Psychosocial professionals indicated that they could influence (<67%) communicating with patients the most.
Discussion
The current study explored barriers and facilitators for implementing PCC in cardiogenetics using a three-round ranking-style Delphi technique. We generated consensus on a list of barriers and facilitators that highlighted the significance of partnership and collaboration between professionals and patients.
Overall, the experts arrived at six barriers to implementation, dispersed across multiple levels of healthcare delivery [26]. First, significant barriers at the healthcare system level, comprised the culture of health care delivery (biomedical orientation) and the absence of PROMs [26, 27]. Second, at the organizational level, workflow, resources and multidisciplinary teamwork were essential barriers. These findings exhibit considerable concordance with previous research on organizational barriers [26, 28]. Finally, an individual patient-oriented barrier comprises patients’ health literacy [29].
One of the significant observations was that clinicians think it will take more time to work in a patient-centered manner. Therefore, time or resource constraints are a key issue in today’s consultation. While it has already been described, there is an erroneous assumption that moving toward a patient-centered approach by adapting a shared decision consultation style [30] or ‘letting patients speak’ [31] will increase the consultation length. However, a study on the determinants of consultation length in general practice showed that consultation length was unaffected by the mention of psychosocial problems by the patient [32]. Shared decision-making may take longer than a standard-length consultation in the short term; once embedded in clinical care, there is some evidence it saves time [27]. The notion of time becomes less straightforward when a ‘standard length’ consultation results in no adherence to treatment by a patient with ICC; this might worsen symptoms and result in a need for more consultations later on [12].
There were essential differences between the perspectives of the various stakeholders. In addition to previous studies [19,20,21, 25] on barriers to PCC, this study revealed the biomedical orientation of current outcome assessment and the neglect of patient-reported outcomes of medical professionals, which patients and psychosocial professionals found to be a barrier to PCC. By focusing on exchanging medical information, one may miss significant patient concerns. Patients often come to their visits with multiple unspoken fears [31]; helping patients articulate these concerns may increase active patient participation, which is perceived as a facilitator for PCC [29].
For the facilitators, organizational and cultural aspects were of the most importance. All our experts expressed that interdisciplinary collaboration across the entire care pathway would help implement PCC; as observed in previous studies, experts describe a smooth flow of information within and between care teams as a vital facilitator [29, 33]. Medical and psychosocial care professionals were on the same page concerning the facilitator ranking. The patient representatives operationalized that collaboration with an in-house psychosocial healthcare worker at the cardio-genetics department is best to facilitate PCC. Other studies previously identified IT infrastructure as a viable option to reduce problems with fragmented care and vital to organizational effectiveness in promoting PCC [28, 33]. IT infrastructure did not emerge as an essential theme in this study, where stakeholders ranked it least important. At the individual level, we identified the professional expertize of employees and an empathic attitude of the staff as characteristics that determine the provision of PCC.
Our exploration also identified several general complicating factors inherent to the complexity of ICC in terms of the societal consequences the patient faces. For example, the extent and process of family disclosure and the general lack of awareness that psychosocial care is needed to resolve some of these harsh consequences. In genetics, much research data exist on legal, moral, and ethical implications [25,26,27]. There are many risks and benefits related to genetic testing (such as practical consequences, privacy issues, and insurability) upon which patients need information. Disclosure to family members is a delicate issue; patients sometimes hesitate to inform their relatives that they may be at risk for developing a specific disorder. Privacy concerns restrict the ability of healthcare providers to disseminate information directly to potentially affected relatives without authorization from the index patient [6]. Finally, patients worry that when a hereditary predisposition is identified, they might have difficulty obtaining health, life or disability insurance and experience employment issues [28]. While these issues complicate the care for patients with ICC, they also may be an incentive to deliver PCC.
Many of the barriers and facilitators identified in this study display similarities (e.g., workflow, teamwork, communication and culture) with previous studies that discussed the challenges to implementation of PCC at different levels: macro level policy measures (healthcare delivery) and micro level incentives at the organizational level and the patient-provider level [26, 29]. The level of influence stakeholders directly involved in the care for patients with ICC and patient representatives’ experience on the identified barriers and facilitators received no attention in other studies.
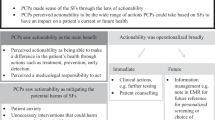
Overall, the expert panel experienced a significant influence on patients’ literacy. However, they (patient representatives and psychosocial workers) ranked it less as an essential obstacle (fourth or fifth place). They share so much impact at the patient level that they do not identify it as a barrier but rather as an opportunity to intervene.
Patient representatives and psychosocial workers identified ‘uncertainty due to variability and ‘time’ as essential barriers and stated low levels of influence on these barriers. How genetic test results are conveyed can vary considerably in different practice environments, countries, and laws. In genetic cardiology in Belgium, physicians try to disclose genetic test results to patients in the presence of a psychosocial healthcare worker (psychologist, genetic counsellor, social worker, specialized cardiac nurse). However, psychosocial workers do not control or disclose clinical information; they can clarify given information by psychoeducation.
There is a noticeable discrepancy between healthcare providers’ assessments of the patient’s needs, the level of influence they can exert on those needs and the care provided in practice. This study shows that stakeholders experience high levels of impact on many barriers and facilitators, and professionals notice many patient needs. However, we observed no change in clinical practice. Our general exploratory survey on current psychosocial care in genetic cardiology showed that psychosocial care and a psychosocial assessment regarding testing are often not performed by a psychologist or social worker. Instead, cardiologists and geneticists or centers only offer psychological counseling on the explicit demand of the patient or the next of kin.
Without a standardized assessment of the needs of patients, clinicians tend to rely on their subjective observation to decide if further psychological support is necessary. However, a study on the role of psychological stress in cardiogenetics emphasizes the importance of the routine inclusion of clinical psychologists in interdisciplinary teams [34]. Supporting teamwork and cohesion among staff members facilitates PCC. One of the core roles of psychologists in hospitals is clinical assessment, using tests to assess current functioning, coping strategies, and ascertain risk management of patients [35]. In addition, becoming a patient-centered, highly functional care team requires a clear definition of the roles and responsibilities of each team member [36].
Future research should consider the abovementioned challenges and quantify how the barriers and facilitators to implementing PCC in cardiogenetics affect daily practice. For example, specific PCC interventions (e.g., structural assessment across the healthcare pathway; explicit and consistent leadership) may be designed to overcome barriers such as the culture of care delivery (mono- vs multidisciplinary) and tested for their feasibility in daily clinical practice. Information gathered from PROMs may provide insight into the patient perspective of clinical management, health and well-being [13] and is considered a core element of PCC. However, primarily generic HRQOL instruments are used in research [19, 37,38,39,40]. Implementating HRQOL surveys in clinical practice routine outcome monitoring is still developing. Disease-specific PROMs are rare, and focus on ICD mainly [19, 39, 41]. Efforts to extend this work and design a disease-specific PROM for cardiogenetics are underway.
The patient and the cardiogenetic team can optimize patient care with improved communication, collaboration (shared decision-making), and merging of individual observations and expertize. Often, specialized training is not organized due to economic costs (organizational level resource constraint) [20, 26]. Therefore, different cardiogenetic centers could combine their expertize and provide training for all stakeholders (medical, psychosocial and patient representatives) to bridge the economic cost and the gaps in knowledge. To build relationships between professionals and patients, we first need to implement this joint expertize from all stakeholders and endorse collaboration, specialized training and shared decision-making to address the emotional concerns, well-being and quality of life issues in patients with ICC.
Several limitations should be considered when interpreting this study’s results. Although there are no guidelines on the appropriate sample size for expert consensus Delphi studies, it is established that a minimum sample size of 10 experts (who are representative of at least three disciplines) is adequate for content validity [25, 42]. The attrition rate in round 3 was 68%, which may affect the validity of the results. Nevertheless, according to Delphi-study recommendations, the dropout was still acceptable [21, 25]. Furthermore, the subdivision per profession made the subgroup sample size smaller than ideal. While it is essential to hear from different perspectives working in cardiogenetics, we should interpret the analyses per profession with caution due to the small sample size. The international composition of the expert panel and the diversity of participants is a strength of this study.
In conclusion, this study revealed health system and organizational barriers and facilitators to implementing PCC and some patient-level factors. The barriers and facilitators to which the experts assigned a high level of influence may be dealt with relatively quickly (e.g., improving communication and health literacy). Changing other barriers, such as biomedical dominance or lack of psychosocial expertize and capacity, may be more challenging. Moreover, close collaboration between medical and psychosocial professionals and patients seems to be needed to successfully implement PCC in cardiogenetics.
Data availability
The data underlying this paper are available in the paper and in its online supplementary material.
References
Tesson S, Butow PN, Sholler GF, Sharpe L, Kovacs AH, Kasparian NA. Psychological interventions for people affected by childhood-onset heart disease: a systematic review. Heal Psychol. 2019;38:151–61.
Platt J. A Person-Centered Approach to Cardiovascular Genetic Testing. Cold Spring Harb Perspect Med. 2020;10:1–14.
Resta R, Biesecker BB, Bennett RL, Blum S, Estabrooks Hahn S, Strecker MN, et al. A New Definition of Genetic Counseling: National Society of Genetic Counselors’ Task Force Report. J Genet Couns [Internet]. 2006;15:77–83. https://doi.org/10.1007/s10897-005-9014-3.
Ingles J, Yeates L, Semsarian C. The emerging role of the cardiac genetic counselor. Hear Rhythm. 2011;8:1958–62.
Cirino AL, Harris S, Lakdawala NK, Michels M, Olivotto I, Day SM, et al. Role of genetic testing in inherited cardiovascular disease: a review. JAMA Cardiol. 2017;2:1153–60.
Paljevic ED. Complexities of Cardiac Genetic Testing. J Nurse Pr [Internet]. 2019;15:139–.e1. https://doi.org/10.1016/j.nurpra.2018.09.009.
Middleton A, Hall G, Patch C. Genetic counselors and Genomic Counseling in the United Kingdom. Mol Genet Genom Med. 2015;3:79–83.
Doyle DL, Awwad RI, Austin JC, Baty BJ, Bergner AL, Brewster SJ, et al. 2013 Review and Update of the Genetic Counseling Practice Based Competencies by a Task Force of the Accreditation Council for Genetic Counseling. J Genet Couns. 2016;25:868–79.
Aatre RD, Day SM. Psychological Issues in Genetic Testing for Inherited Cardiovascular Diseases. Circ Genet. 2011;4:81–90.
Cirino AL, Ho CY. Genetic testing for inherited heart disease. Circulation 2013;128:1–10.
Musunuru K, Hershberger RE, Day SM, Klinedinst NJ, Landstrom AP, Parikh VN, et al. Genetic Testing for Inherited Cardiovascular Diseases: A Scientific Statement From the American Heart Association. Circ Genom Precis Med. 2020;13:e000067.
Ahmad N, Ellins J, Krelle H, Lawrie M, Health Foundation (Great Britain). Person-centred care: from ideas to action [Internet]. London: Health Foundation. 2014. p. 1–100. www.health.org.uk
Desomer A, Van den Heede K, Triemstra M, Paget J, De Boer D, Kohn LCI. Use of patient-reported outcome and experience measures in patient care and policy. Health Services Research (HSR) Brussels: Belgian Health Care Knowledge Centre (KCE). KCE Reports. 2018.
Tramonti F, Giorgi F, Fanali A. Systems thinking and the biopsychosocial approach: A multilevel framework for patient-centred care. Syst Res Behav Sci. 2021;38:215–30.
Caleshu C, Kasparian NA, Edwards KS, Yeates L, Semsarian C, Perez M, et al. Interdisciplinary psychosocial care for families with inherited cardiovascular diseases. Trends Cardiovasc Med. Elsevier Inc.; 2016;26:647–53.
Metcalfe SA. Genetic counselling, patient education, and informed decision-making in the genomic era. Semin Fetal Neonatal Med [Internet]. 2018;23:142–9. https://doi.org/10.1016/j.siny.2017.11.010.
Ingles J, Johnson R, Sarina T, Yeates L, Burns C, Gray B, et al. Social determinants of health in the setting of hypertrophic cardiomyopathy. Int J Cardiol. 2015;184:743–9.
Sandhu U, Kovacs AH, Nazer B. Psychosocial symptoms of ventricular arrhythmias: Integrating patient-reported outcomes into clinical care. Heart Rhythm. 2021;2:832–9. O2
van den Heuvel LM, Sarina T, Sweeting J, Yeates L, Bates K, Spinks C, et al. A prospective longitudinal study of health-related quality of life and psychological wellbeing after an implantable cardioverter-defibrillator in patients with genetic heart diseases. Hear Rhythm. 2022;3:143–51. O2
Hanssen DJC, Ras A, Rosmalen JGM. Barriers and facilitators to the implementation of interventions for medically unexplained symptoms in primary care: a modified Delphi study. J Psychosom Res [Internet]. 2021;143:110386 https://doi.org/10.1016/j.jpsychores.2021.110386.
Keeney S, Hasson F, McKenna H. Consulting the oracle: Ten lessons from using the Delphi technique in nursing research. J Adv Nurs. 2006;53:205–12.
Schmidt RC. Managing Delphi surveys using nonparametric statistical techniques. Decis Sci. 1997;28:763–74.
Okoli C, Pawlowski SD. The Delphi method as a research tool: An example, design considerations and applications. Inf Manag. 2004;42:15–29.
Eijzenga W, Bleiker EMA, Hahn DEE, Kluijt I, Sidharta GN, Gundy C, et al. Psychosocial Aspects of Hereditary Cancer (PAHC) questionnaire: development and testing of a screening questionnaire for use in clinical cancer genetics. Psychooncology. 2014;23:862–9.
Kennedy HP. Enhancing Delphi research: Methods and results. J Adv Nurs. 2004;45:504–11.
Scholl I, LaRussa A, Hahlweg P, Kobrin S, Elwyn G. Organizational- and system-level characteristics that influence implementation of shared decision-making and strategies to address them - a scoping review. Implement Sci. 2018;13:1–22.
Moore L, Britten N, Lydahl D, Naldemirci Ö, Elam M, Wolf A. Barriers and facilitators to the implementation of person-centred care in different healthcare contexts. Scand J Caring Sci. 2017;31:662–73.
Luxford K, Gelb Safran D, Delbanco T. Promoting patient-centered care: a qualitative study of facilitators and barriers in healthcare organizations with a reputation for improving the patient experience. Int J Qual Heal Care. 2011;23:510–5.
Vennedey V, Hower KI, Hillen H, Ansmann L, Kuntz L, Stock S. Patients’ perspectives of facilitators and barriers to patient-centred care: Insights from qualitative patient interviews. BMJ Open. 2020;10:1–11.
Foundation TH. Person-centred care made simple. What everyone should know about person-centred care. Heal Found [Internet]. 2016:45. https://www.health.org.uk/sites/default/files/PersonCentredCareMadeSimple.pdf
Fischer M, Ereaut G. When doctors and patients talk: Making sense of the consultation. London: the Health Foundation; 2012:1–57.
Deveugele M, Derese A, van den Brink-Muinen A, Bensing J, De Maeseneer J. Consultation length in general practice: cross sectional study in six European countries. BMJ. 2002;325:472.
Hower K, Vennedey V, Hillen H, Kuntz L, Stock S, Pfaff H, et al. Correction: Implementation of patient-centred care: which organisational determinants matter from decision maker’s perspective? Results from a qualitative interview study across various health and social care organisations. BMJ Open. 2019;9.
Hidayatallah N, Silverstein L, Stolerman M, McDonald T, Walsh CA, Paljevic E, et al. Psychological stress associated with cardiogenetic conditions. Per Med. 2014;11:631–40.
Wahass SH. The role of psychologist in health care delivery.pdf. J Fam Commun Med. 2005;12:63–70.
Greene SM, Tuzzio L, Cherkin D. A Framework for Making Patient-Centered Care Front and Center. Perm J. 2012;16:49–53.
Ingles J, Burns C, Barratt A, Semsarian C. Application of Genetic Testing in Hypertrophic Cardiomyopathy for Preclinical Disease Detection. Circ Genet. 2015;8:852–9.
Richardson E, Spinks C, Davis A, Turner C, Atherton J, McGaughran J, et al. Psychosocial Implications of Living with Catecholaminergic Polymorphic Ventricular Tachycardia in Adulthood. J Genet Couns. 2018;27:549–57.
Hickey KT, Sciacca RR, Biviano AB, Whang W, Dizon JM, Garan H, et al. The effect of cardiac genetic testing on psychological well-being and illness perceptions. Hear LUNG. 2014;43:127–32.
James CA, Tichnell C, Murray B, Daly A, Sears SF, Calkins H. General and disease-specific psychosocial adjustment in patients with arrhythmogenic right ventricular dysplasia/cardiomyopathy with implantable cardioverter defibrillators: A large cohort study. Circ Cardiovasc Genet. 2012;5:18–24.
Van Den Broek KC, Heijmans N, Van Assen MALM. Anxiety and Depression in Patients with an Implantable Cardioverter Defibrillator and Their Partners: A Longitudinal Study. Pacing Clin Electrophysiol. 2013;36:362–71.
Hasson F, Keeney S, McKenna H. Research guidelines for the Delphi survey technique. J Adv Nurs. 2000;32:1008–15.
Acknowledgements
We would like to thank all of the EPIC consortium members (European group for PROMS In Cardiogenetics) for their participation to the online survey, the workshops and the Delphi-study.
Funding
SVP is supported by the Innoviris Brussels Region BRIDGE grant IGenCare. (Grant number: BRGIMP12: https://researchportal.vub.be/en/projects/bridge-igencare-integrated-personalized-medical-genomics-care-sol).
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by [SVP], [FeH] and [NK]. The first draft of the paper was written by [SVP] and [NK] and all authors commented on previous versions of the paper. All authors read and approved the final paper.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
The Delphi study abides by the ethical requirements of the University Hospital of Brussels, aiming to assure ‘rigor, respect and responsibility’ in the conduct of the research project. Ethical approval was not required. Stakeholders participating in the Delphi-study were informed of the study and gave consent for participation.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
van Pottelberghe, S., Heine, F., Van Dooren, S. et al. Barriers and facilitators for the implementation of patient-centered care in cardiogenetics: a Delphi study among ERN GUARD-heart members. Eur J Hum Genet 31, 1371–1380 (2023). https://doi.org/10.1038/s41431-022-01268-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41431-022-01268-7
This article is cited by
-
Ambivalence and regret in genome sequencing
European Journal of Human Genetics (2023)
