
Abstract
Recent trials have shown remarkable efficacy from combined trastuzumab and chemotherapy in the adjuvant setting of breast cancer. In spite of these successes, refractory breast cancer has emerged as a clinically problematic outcome for a subset of patients managed this way. In an effort to clarify and optimize the treatment regimens for breast cancer patients who are candidates to receive trastuzumab, we sought to analyze whether a distinctive genetic signature could be characterized that would reliably predict the treatment outcome. The ability to predict who will respond and who will become refractory to this agent will allow for improved, rational clinical management of these patients and further stratify the personalized nature of this treatment regimen. In this study, 41 consecutive cases of breast carcinoma with well-documented amplification of the human epidermal growth factor receptor-2 gene and corresponding banked fresh-frozen tissue were identified and divided into two separate groups based on whether they received trastuzumab or not. The first group consisted of 12 patients who had received trastuzumab in the adjuvant setting, of which three later experienced tumor recurrence. The second group consisted of 10 patients not treated with trastuzumab, of which 6 were later found to have recurrence. Differentially expressed genetic profiles were determined using human genome-wide Illumina Bead Microarrays. The differentially expressed genes for non-recurrence vs recurrence in the trastuzumab-treated group were distinct from those in the same comparison group in the untreated group. Differential expression of key genes indentified in this study might offer an insight into a possible mechanism of trastuzumab resistance in breast carcinoma, and may emerge as potential predictive biomarkers indicative of trastuzumab resistance.
Similar content being viewed by others


Main
Human epidermal growth factor receptor-2 (HER2) belongs to the type I family of tyrosine kinase receptors involved in the signal transduction pathways that regulates epithelial cell growth, differentiation, apoptosis and metastasis. With the exception of HER2, which has no ligand, the HER proteins exist at the plasma membrane in an inactivated form that activates on ligand binding.1, 2
Overexpression of HER2 occurs in approximately 18–20% of invasive breast cancers.3, 4 HER2 overexpression deregulates downstream signaling networks, which in turn affect tumor cell growth and survival and have been previously documented to predict for a poor clinical outcome.5 A ‘crosstalk’ between signaling networks that regulate growth and survival is known to exist in epithelial tumors. In breast cancers, this crosstalk has been shown to exist between the HER2 pathway and estrogen receptor α and a key regulator of cell growth and survival, insulin-like growth factor receptor 1, the latter of which is also upregulated in breast cancers.6, 7, 8
Trastuzumab, a monoclonal antibody that targets HER2, has significantly improved disease-free and overall survival when combined with chemotherapy for patients with breast cancers treated in both the adjuvant and metastatic settings.2, 9, 10, 11 Pre-clinical studies indicate synergistic antitumor activity when trastuzumab is combined with a number of anticancer drugs. As well, additive cytotoxic interactions between trastuzumab and other agents, including paclitaxel, have been shown.12 However, a subset of patients who initially received trastuzumab in the adjuvant setting eventually develop recurrent, resistant tumor within 1 year of treatment.13 The emergence of refractory tumors has become a significant clinical problem, with numerous pre-clinical studies already having investigated such possible etiologies for this resistance as HER2 downstream signaling, crosstalk pathways and HER2 gene mutations.14
The clinical, financial and emotional implications of a trastuzumab treatment regimen cannot be overlooked. An entire year must be committed to intravenous therapy for those patients that will receive this agent. Notable side effects include a significant risk for cardiotoxicity especially following adjuvant anthracyclines.15, 16 Although initially thought to be reversible, the idea of the transient nature of this therapy-related cardiac dysfunction has been recently called into question.15 Finally, for the estimated 15 000 patients predicted to be eligible to receive trastuzumab, the collective financial burden has been calculated to be as high as $750 million per year.17 Therefore, the ability to predict trastuzumab resistance will have a tremendous effect in all aspects of the health care for breast cancer patients. The intent of this study was to identify a genetic signature that could predict trastuzumab resistance and poor clinical outcome. To our knowledge, this is the first study to determine whether a distinct molecular signature of gene expression exists in patients known to clinically show resistance to trastuzumab.
Materials and methods
Patients’ Selection
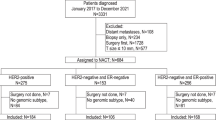
A total of 151 patients with amplified HER2 detected by fluorescence in situ hybridization were identified from the files of the Roswell Park Cancer Institute between the years 2001 and 2009. For all cases, tissue was collected on extirpation and delivered to the Department of Pathology in under 5 min. Thereafter, appropriate portions of tumor were selected and snap frozen within 5 min. The biospecimen inclusion criteria for this study included the existence of banked, fresh-frozen tumor, tumor occupying >80% of the tissue and extracted RNA that met the Illumina platform's workable criteria (see below). Of the 151 patients initially identified, only 42 were found to fulfill the aforementioned criteria and therefore warrant inclusion into this study.
Clinicopathologic data including patient's age at diagnosis, race, tumor histologic type, stage, grade, size, hormonal receptor and lymph node status were abstracted from their medical records. Data on receipt of adjuvant chemotherapy, receipt or no receipt of trastuzumab, and duration of disease-free survival were recorded. Two separate groups were readily identified: those treated with trastuzumab and those not treated with trastuzumab. The first group was further subcategorized based on whether or not they developed resistance to trastuzumab therapy. Patients were considered resistant to this therapeutic approach if they showed local or distant tumor recurrence within 2 years of being treated with trastuzumab. In contrast, patients who did not receive adjuvant trastuzumab therapy were divided into two groups; a poor-prognosis group if they had local or distant tumor recurrence within 2 years, and a good-prognosis group if they were disease free for >2 years. These groups did not include patients who presented with distant organ metastases (stage 4). Review of the patients’ medical records along with performing the gene array of the patients’ samples was approved by the institutional review board.
RNA Preparation
Total RNA from 42 patients were prepared using the TRizol Reagent (Invitrogen, Carlsbad, CA, USA) following the manufacturer's instructions. After elution, RNA samples were concentrated by EtOH precipitation at −20 °C overnight and resuspended in nuclease-free water. Before labeling, RNA samples were quantitated using a ND-1000 spectrophotometer (NanoDrop) and evaluated for degradation using a 2100 Bioanalyzer (Agilent Technologies, Sanat Clara, CA, USA). By Illumina criteria, samples were required to have a RIN >7, an OD 260:280 of 1.9–2.0, an OD 260/230 >1.8 and >1.5 28S:18S ratio of the ribosomal bands for gene expression array analysis.
Gene Expression Assay
Expression profiling was accomplished using the HumanHT-12 v3 whole-genome gene expression direct hybridization assay (Illumina). Initially, 250 ng total RNA was converted to cDNA, followed by an in vitro transcription step to generate labeled cRNA using the Ambion Illumina TotalPrep RNA Amplification Kit (Ambion, Austin, TX, USA) as per the manufacturer's instructions. The labeled probes were then mixed with hybridization reagents and hybridized overnight to the HumanHT-12 v3 BeadChips. Following washing and staining, the BeadChips are imaged using the Illumina BeadArray Reader to measure fluorescence intensity at each probe. The intensity of the signal corresponded to the quantity of the respective mRNA in the original sample.
Data Analysis
BeadChip data files were analyzed with Illumina's GenomeStudio gene expression module and Bioconductor package to determine gene expression signal levels.18 Briefly, the raw intensity of Illumina Human HT-12 v3.0 gene expression array was scanned and extracted using BeadScan, with the data corrected by background subtraction in GenomeStudio module. The lumi module in the R-based Bioconductor Package was used to transform the expression intensity into log2 scale.19 The log2 transformed intensity data were normalized using the Quantile normalization algorithm.
For data quality control, we first filtered out sample 11142 from further analysis as it stood out as an outlier with the majority of genes undetected (Figure 1, Table 3). This led to 41 samples for further clinicopathologic and microarray data analysis. Then, we filtered out the genes whose expression-detection P-value was >0.05 (ie, indistinguishable from the background intensity) across >75% of samples. Approximately 17 000 genes among 37 849 genes passed this filtering for downstream analysis. Several notable genes including PIK3CA, MUC4 and AKT were filtered out from subsequent analysis. For example, PIK3CA was not expressed (P>0.05) in all but one sample.

Box plot of expression-detection P-value for all 42 samples. The expression-detection P-value is to test the null hypothesis of whether the expression intensity of a given gene is indistinguishable from the background intensity. Y axis: expression-detection P-value; X axis: samples (patients). Patient 11142 (shown in gray) stand out as an outlier showing majority of genes undetectable (large P-value). For data quality control, we filtered out this sample for further analysis. This led to 41 samples for further clinicopathologic and microarray data analysis.
We then performed eight separate comparisons based on the following collected patients’ characteristics: age (<50 vs ≥50 or <40 vs ≥40), race (black vs white), tumor stage (advanced vs early), hormonal receptor status (hormonal receptor– vs hormonal receptor+), menopausal status (pre- vs post-), non-recurrence vs recurrence in the trastuzumab-non-treated group and responsive vs resistant in the trastuzumab-treated group. We used the Limma program in the R-based Bioconductor package to calculate the level of gene differential expression for each comparison.20 Briefly, for each comparison, a linear model was fit to the data (with cell means corresponding to the different conditions and a random effect for array). For each comparison, we obtained the list of differentially expressed genes constrained by P-value <0.05.
Following single gene-based significance testing, we use the expression value of differentially expressed genes (P<0.05) to cluster the patients for each comparison. Our purpose was to test whether the identified differentially expressed genes for each comparison were able to serve as gene signature to classify patients into their corresponding clinicopathologic groups. Hierarchical clustering based on the average linkage of Pearson correlation was used.21 All calculations were carried out using statistical software available in the R package.
Results
Clinicopathologic Findings
A total of 41 HER2-positive breast cancer patients treated between 2001 and 2009 at the Roswell Park Cancer Institute had tumors amenable to microarray analysis for this study. Patient characteristics are shown in Table 1. In total, 21 of 41 cases (51%) analyzed were <50 years at time of diagnosis; the median age was 49 years (range 28–82). Two-thirds of the cases had high-grade tumors and the majority of individuals had ductal histology. The median and range of follow-up was between 3 and 111 (median 29 months). Five patients died, two because of breast cancer and three of unknown reason. Patients were composed of 12 with trastuzumab treated, 10 not treated with trastuzumab, 5 who presented with distant organ metastases (stage 4), 4 who were lost to follow-up and 9 that had <2 years follow-up but with no tumor recurrence. In the trastuzumab-treated group, three patients had tumor recurrence at 3, 18 and 19 months, respectively. In the group not treated with trastuzumab, six patients had tumor recurrence after a median of 10 months and range of 3 and 24 months (Tables 2 and 3).
Gene Expression Findings
Identification of differentially expressed genes
Eight separate comparisons were performed based on the following collected patients’ characteristics: trastuzumab-treated group (responsive vs resistant), trastuzumab-non-treated group (no recurrence vs recurrence), age (<50 vs ≥50 or <40 vs ≥40), race (black vs white), tumor stage (advanced vs early), hormonal receptor status (hormonal receptor– vs hormonal receptor+) and menopausal status (pre- vs post-).
For the trastuzumab-treated group (responsive vs resistant), we identified 770 differentially expressed genes at the statistically significant level of P<0.05, with 281 genes upregulated in patients found to be responsive to trastuzumab while 489 genes were downregulated. For the trastuzumab-non-treated group, we identified 509 statistically significant (P<0.05) differentially expressed genes with 329 genes upregulated in patients with no recurrence while 189 were genes downregulated. The number of identified differentially expressed genes with a P<0.05 and the subgroup restricted by desired fold change for each comparison are summarized in Table 4.
Patients clustering based on differentially expressed genes
The expression value of differentially expressed genes identified from each comparison was used to cluster the patients into their corresponding clinicopathologic groups. As shown in Figure 2, the 770 differentially expressed genes derived from the trastuzumab-treated group separated into three trastuzumab-resistant and nine trastuzumab-responsive patients. In the same way, the 509 differentially expressed genes derived from those not treated with trastuzumab separated into six patients with recurrence and four with no recurrence (Figure 3).

Hierarchical clustering of patient samples based on differentially expressed genes (P<0.05) obtained from the trastuzumab-treated group, responsive vs resistant. (a) Clustering dendrogram: Y initial means resistant while N initial means responsive. (b) Clustering heat map: red means upregulated while green means downregulated.

Hierachical clustering of patient samples based on differentially expressed genes (P<0.05) obtained from the trastuzumab-non-treated group, non-recurrence vs recurrence. (a) Clustering dendrogram: Y initial means recurrence while N initial means non-recurrence. (b) Clustering heat map: red means upregulated while green means downregulated.
The patient clustering results using differentially expressed genes derived from the other seven comparisons is shown in Figure 4. The results show that those respective differentially expressed genes can more or less separate the patients into their corresponding clinicopathologic groups. As expected, better clustering performance was obtained in hormonal receptor status and tumor stage categories, and worse clustering performance was observed in age and menopause status.

Hierarchical clustering of patient samples based on differentially expressed genes (P<0.05) obtained from comparing (a) age (<50 vs ≥50); (b) age (<40 vs ≥40); (c) race (black vs white); (d) tumor stage (advanced vs early); (e) hormone receptor status (hormone receptor– vs hormone receptor+); (f) menopause status (pre- vs post-).
Few overlap between differentially expressed gene sets
We grouped the differentially expressed genes from age (<50 vs ≥50 or <40 vs ≥40), race (black vs white), tumor stage (advanced vs early), hormonal receptor status (hormonal receptor– vs hormonal receptor+) and menopausal status (pre- vs post-) into one non-redundant differentially expressed genes set. This differentially expressed gene set, termed ‘other’, is composed of 3456 unique genes showing differential expression in at least one of the six comparisons above.
As shown in Figure 5, we found that there was little overlap between the three differentially expressed gene sets: trastuzumab-treated, untreated and ‘others’. Only two differentially expressed genes were shared by all three differentially expressed genes sets. The lack of overlap between the gene sets derived from the trastuzumab-treated and non-treated groups were of particular interest. Only 23 differentially expressed genes were shared between the 770 (3.0%) trastuzumab-treated group and the 509 (4.5%) trastuzumab-untreated group and only 1 differentially expressed gene was shared when a ≥twofold change was included as a restrictive criteria.

Venn diagrams show little overlap for differentially expressed genes derived from different comparisons, including three groups, trastuzumab-treated, trastuzumab-non-treated and other. The latter group represents the unions of differentially expressed genes from the other six separate comparisons of clinicopathologic data (age, race, tumor stage, hormonal receptor status and menopause status). (a) Differentially expressed genes as defined by P<0.05. (b) Differentially expressed genes with at least 1.5-fold change. (c) Differentially expressed genes with at least twofold change.
Further functional annotation of differentially expressed genes with at least a twofold change showed that the composition of enriched function term was different between the two different groups (Figure 6). Remarkably, the trastuzumab-treated differentially expressed genes were enriched for genes involved in nucleic acid binding while the trastuzumab-untreated profile was enriched in immunity and defense. The complete differentially expressed gene list between these two groups with the stipulation of at least a twofold change is listed in Tables 5 and 6.

Enriched function annotation for differentially expressed genes with at least twofold change. Functional annotations are considered enriched with P-values <0.1 as reported by NCBI DAVID API server (default setting). (Left) Enriched biological process term; (Right) enriched molecular function term. The number following each enriched functional term is the number of annotated differentially expressed genes. (a) Functional annotation for differentially expressed genes from the trastuzumab-treated group. (b) Functional annotation for differentially expressed genes from the trastuzumab-non-treated group. (c) Functional annotation for other differentially expressed genes.
Previously described significant genes in trastuzumab resistance of pre-clinical studies
Previous studies have shown that the HER2 signaling pathway might have an important role in trastuzumab resistance.14 Therefore, we tested the hypothesis whether the HER2 signaling pathway members were significantly dysregulated in the trastuzumab-treated comparison group. Briefly, the 17 000 genes were ranked based on the t-statistics score for comparing the mean expression value of trastuzumab treatment (responsive vs resistant). This ranked list was used to analyze whether the t-statistical score of genes from the HER2 signaling pathway were significantly deviated from those in the rest of the gene sets. Statistical significance was estimated by Kolmogorov–Smirnov test.22 The HER2 pathway data set was obtained from KEGG database with manual addition from existing literature.
The HER2 pathway was significantly dysregulated in the trastuzumab-treated group response comparison (K–S test, P<0.017). However, only the PTPN11 gene in the HER2 pathway showed a statistically significant differential expression at the single gene level (P<0.05). The HER2 pathway was not found to be significantly dysregulated in the other six comparisons (eg, P=0.21 in trastuzumab-non-treated comparison).
We further checked a compiled list of genes that might have a role in trastuzumab resistance as suggested by previous literature that included PTEN, PIK3, mTOR, MAPK and vascular endothelial growth factor (VEGF) (Table 7). However, there was no evidence of differential expression.
Discussion
Human breast tumors are diverse in their natural history and in their responsiveness to treatments.23 The revelation of distinctive molecular portraits for human breast cancers has had tremendous implications on breast cancer therapy and research. Breast cancers can now be subdivided into three categories: ER+/luminal-like, basal-like and HER2+; the latter of which can be further subdivided into ER+ and ER–.24, 25 This discovery had enabled further work into identifying predictors for survival through the identification of distinctive gene signatures. Two tests are now clinically available that can predict clinical outcome and indicate therapy in ‘estrogen receptor-positive lymph node-negative’ breast cancer patients with Mammaprint and Oncotype DX gene profiles.26, 27
The advent of immunotherapy and the implications it may have on tumors have recently introduced another variable that needs to be taken into consideration. The therapeutic humanized monoclonal antibody trastuzumab is still a mystery in its mechanism of action and lately, the reason for the emergence of resistance to it. The suggested mechanism of action is disruption of functional dimers involving HER2, reduction of extracellular domain shedding (which is thought to result in a constitutively active receptor (p95HER2)), and the recruitment of immune effector cells, which results in antibody-dependent cellular cytotoxicity.28, 29 For resistance, there are many suggested mechanisms of action that have included the hypothesis that they may exist, a reduction of antibody affinity because of MUC4 overexpression.30, 31 We have previously suggested the existence of a HER2 gene mutation located in the immunoagent's corresponding binding site as a mechanism for trastuzumab resistance. However, DNA sequencing was unable to validate the initial findings of temperature gradient capillary electrophoresis except for one case, which had a single missense point mutation.32 Downstream signaling pathway members have also been suggested as a potential source for trastuzumab resistance and have included the genes p27 Kip1, PTEN, PI3K, mTOR and Akt.33, 34, 35 Crosstalk with other pathways including insulin-like growth factor receptor-1, ER pathway and VEGF has also been suggested to be involved in trastuzumab resistance.36, 37, 38 However, these studies were all pre-clinical or in cell lines.
Partially based on these previous findings, we therefore sought to examine whether a distinctive genetic profile existed that would be able to discriminate HER2 patients into good and poor clinical outcomes and into trastuzumab responsive or resistant. A strength of this study was the use of actual, well annotated, clinical biospecimens. We based this assumption on the hypothesis that the phenotypic diversity of HER2+ breast tumors might be accompanied by a corresponding diversity in gene expression patterns that we could capture using cDNA microarrays.
Although initially stratifying patients into responsive or resistant groups was somewhat artificial, we found from our data that a 2-year cut-off was reasonable. In the group treated with trastuzumab, the three patients who had tumor recurrence did so within 19 months while the other nine patients had no recurrence at all after at least a 33-month follow-up. For the untreated trastuzumab group, a 2-year cut-off was reasonable based on similar clinical outcomes. For those patients with tumor recurrence, all did so within a 24-month timeframe. Patients who were disease free had no recurrence after at least a 49-month follow-up period.
Although the sample size was too small for a definitive conclusion, we believe that our findings shed meaningful insights into the clinical care of breast cancer patients that warrant further investigation. From the clinical data, it was expected that clustering based on trastuzumab-treated (responsive vs recurrence) and trastuzumab-non-treated (recurrence vs no recurrence) would have distinctive profiles. In addition, to a lesser extent, it was expected that the other clinicopathologic variables would have some differences in the expression profiles as they related to hormonal receptor status and tumor stage but not age, race or menopausal status. There was little overlap between the treated, and untreated trastuzumab groups with those in the ‘other’ groups. This implies that clinicopathologic differences may involve alternative molecular mechanisms and therefore perhaps, underlying distinctive gene sets.
Multiple genes had variable expression profiles in both the trastuzumab-treated and -untreated groups. Although the predominant genes that were differentially expressed in the trastuzumab-treated group involved DNA binding, those in the untreated group were found to be annotated to immunity and defense. Therefore, we suggest that the mechanism (DNA binding) by which patients who were treated with trastuzumab and subsequently developed recurrence may be different from those who were not treated and had a poor clinical outcome (immunity and defense). However, given the small sample size, these findings should be interpreted with caution as a larger group will be needed to validate these findings.
We further examined the genes that were previously reported to be involved in trastuzumab resistance including PTEN, PIK3, mTOR, MAPK and VEGF and found no significant changes.33, 34, 35, 36, 37, 38 There are three possible explanations; these genes may not exert their role at the transcriptional level, the study sample size was too small or an actual absence in the role of trastuzumab resistance. The latter might be true because our study was conducted on actual patients and their tissues rather than in the pre-clinical setting. AKT, IGF-R1, p27 Kip1 and MUC4 were filtered out. In addition, we looked into HER2 pathway members. Interestingly, we found that known participants in this pathway were significantly dysregulated in the trastuzumab-treated group. However, only the PTPN11 gene in the HER2 pathway showed significant alterations at the single gene level, indicating that there were modest but consistently coordinated changes in the HER2 pathway components that can lead to significant dysregulation. Remarkably, the HER2 pathway was not found to be significantly dysregulated in all other seven comparisons.
Of particular note was our observation on the expression levels of tissue inhibitor metallopeptidase 1, which was found to be upregulated in patients noted to be responsive to trastuzumab (Table 5). Tissue inhibitor metallopeptidase 1 is one of the naturally occurring inhibitors of matrix metalloproteinases that affects cellular proliferation, apoptosis and angiogenesis, both dependent on and independent of its matrix metalloproteinase-inhibiting function. The prognostic value of tissue inhibitor metallopeptidase 1, on mRNA or protein level, was extensively studied in breast cancers with conflicting results.39 However, all of these studies did not correlated tissue inhibitor metallopeptidase 1 with HER2 overexpression. In our study, tissue inhibitor metallopeptidase 1 was upregulated in the responsive patients. Therefore, tissue inhibitor metallopeptidase 1 can be included with the gene set that could potentially predict trastuzumab responsiveness.
In conclusion, there were distinctive gene signatures for trastuzumab resistance in trastuzumab-treated patients and poor clinical outcome in those patients not treated with this agent. Additional studies with larger group will be needed to validate our results and to pare down the number of genes that could serve as reliable predictors for trastuzumab resistance. Such a gene set may have clinical utility in the planning of which therapeutic strategy to use as well as a prognostic tool for HER2-positive breast cancer patients
References
Yarden Y, Sliwkowski MX . Untangling the ErbB signalling network. Nat Rev Mol Cell Biol 2001;2:127–137.
Pinkas-Kramarski R, Soussan L, Waterman H, et al. Diversification of Neu differentiation factor and epidermal growth factor signaling by combinatorial receptor interactions. EMBO J 1996;15:2452–2467.
Yaziji H, Goldstein LC, Barry TS, et al. HER-2 testing in breast cancer using parallel tissue-based methods. JAMA 2004;291:1972–1977.
Owens MA, Horten BC, Da Silva MM . HER2 amplification ratios by fluorescence in situ hybridization and correlation with immunohistochemistry in a cohort of 6556 breast cancer tissues. Clin Breast Cancer 2004;5:63–69.
Slamon DJ, Clark GM, Wong SG, et al. Human breast cancer: correlation of relapse and survival with amplification of the HER-2/neu oncogene. Science 1987;235:177–182.
Camirand A, Lu Y, Pollak M . Co-targeting HER2/ErbB2 and insulin-like growth factor-1 receptors cause synergistic inhibition of growth in HER2-overexpressing breast cancer cells. Med Sci Monit 2002;8:521–526.
Lu Y, Zi X, Zhao Y, et al. Insulin-like growth factor-I receptor signaling and resistance to trastuzumab (Herceptin). J Natl Cancer Inst 2001;93:1852–1857.
Harris LN, You F, Schnitt SJ, et al. Predictors of resistance to preoperative trastuzumab and vinorelbine for HER2-positive early breast cancer. Clin Cancer Res 2007;13:1198–1207.
Joensuu H, Kellokumpu-Lehtinen PL . Adjuvant docetaxel or vinorelbine with or without trastuzumab for breast cancer. N Engl J Med 2006;354:809–820.
Piccart-Gebhart MJ, Procter M, Leyland-Jones B, et al. Trastuzumab after adjuvant chemotherapy in HER2-positive breast cancer. N Engl JMed 2005;353:1659–1672.
Romond EH, Perez EA, Bryant J, et al. Trastuzumab plus adjuvant chemotherapy for operable HER2-positive breast cancer. N Engl J Med 2005;353:1673–1684.
Pegram MD, Konecny GE, O’Callaghan C, et al. Rational combinations of trastuzumab with chemotherapeutic drugs used in the treatment of breast cancer. J Natl Cancer Inst 2004;96:739–749.
Nahta R, Esteva FJ . Herceptin. mechanisms of action and resistance. Cancer Lett 2006;232:123–138.
Pegram MD . Can we circumvent resistance to ErbB2-targeted agents by targeting novel pathways? Clin Breast Cancer Suppl 2008;8 (Suppl 3):S121–S130.
Telli ML, Hunt SA, Carlson RW, et al. Trastuzumab-related cardiotoxicity: callin into question the concept of reversibility. J Clin Oncol 2007;25:3525–3533.
Tan-Chiu E, Yothers G, Romond E, et al. Assessment of cardiac dysfunction in a randomized trial comparing doxorubicin and cyclophosphamide followed by paclitaxel, with or without trastuzumab as adjuvant therapy in node-positive, human epidermal growth factor receptor 2-overexpressing breast cancer: NSABP B-31. J Clin Oncol 2005;23:7811–7819.
Hillner BE, Smith TJ . Do the large benefits justify the large costs of adjuvant breast cancer trastuzumab? J Clin Oncol 2007;25:611–613.
Gentleman RC, Carey VJ, Bates DM, et al. Bioconductor: open software development for computational biology and bioinformatics. Genome Biol 2004;5:R80.
Du P, Kibbe WA, Lin SM . Lumi. A pipeline for processing Illumina microarray. Bioinformatics 2008;24:1547–1548.
Smyth GK . Linear models and empirical Bayes methods for assessing differential expression in microarray experiments. Stat Appl Genet Mol Biol 2004;3:R3.
Eisen MB, Spellman PT, Brown PO, et al. Cluster analysis and display of genome-wide expression patterns. Proc Natl Acad Sci USA 1998;95:14863–14868.
Subramanian A, Tamayo P, Mootha VK, et al. Gene set enrichment analysis: a knowledge-based approach for interpreting genome-wide expression profiles. Proc Natl Acad Sci USA 2005;102:15545–15550.
Tavassoli FA, Schnitt SJ . Pathology of the Breast. Elsevier: New York, 1992.
Perou CM, Sørlie T, Eisen MB, et al. Molecular portraits of human breast tumours. Nature 2000;17:747–752.
T Sørlie T, Perou CM, Tibshirani R, et al. Gene expression patterns of breast carcinomas distinguish tumor subclasses with clinical implications. Proc Natl Acad Sci USA 2001;98:10869–10874.
Van de Vijver MJ, He YD, van’t Veer LJ, et al. A gene-expression signature as a predictor of survival in breast cancer. N Engl J Med 2002;347:1999–2009.
Paik S, Shak S, Tang G, et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J Med 2004;351:2817–2826.
Hudis CA . Trastuzumab-mechanism of action and use in clinical practice. N Engl J Med 2007;357:39–51.
Weiner LM, Adams GP . New approaches to antibody therapy. Oncogene 2000;19:6144–6151.
Moniaux N, Andrianifahanana M, Brand RE, et al. Multiple roles of mucins in pancreatic cancer, a lethal and challenging malignancy. Br J Cancer 2004;91:1633–1638.
Carraway KL, Perez A, Idris N, et al. Muc4/sialomucin complex in the mammary gland and breast cancer. J Mammary Gland Biol Neoplasia 2001;6:323–337.
Khoury T, Mojica W, Hicks DG, et al. Trastuzumab binding site mutations in HER2 positive invasive breast cancer: a potential predictor of less aggressive disease and trastuzumab resistance. Breast Cancer Res Treat 2006;100 (Suppl 1):S31 (abstract 308).
Nahta R, Takahashi T, Ueno NT, et al. P27Kip1 down-regulation is associated with trastuzumab resistance in breast cancer cells. Cancer Res 2004;64:3981–3986.
Nagata Y, Lan KH, Zhou X, et al. PTEN activation contributes to tumor inhibition by trastuzumab, and loss of PTEN predicts trastuzumab resistance in patients. Cancer Cell 2004;6:117–127.
Lu CH, Wyszomierski SL, Tseng LM, et al. Preclinical testing of clinically applicable strategies for overcoming trastuzumab resistance caused by PTEN deficiency. Clin Cancer Res 2007;13:5883–5888.
Nahta R, Yuan LXH, Zhang B, et al. Insulin-like growth factor-I receptor/ human epidermal growth factor receptor 2 heterodimerization contributes to trastuzumab resistance of breast cancer cells. Cancer Res 2005;65:11118–11128.
Chung Y-L, Sheu M-L, Yang S-C, et al. Resistance to tamoxifen-induced apoptosis is associated with direct interaction between Her2/neu and cell membrane estrogen receptor in breast cancer. Int J Cancer 2002;97:306–312.
du Manoir JM, Francia G, Man S, Mossoba M, et al. Strategies for delaying or treating in vivo acquired resistance to trastuzumab in human breast cancer xenografts. Clin Cancer Res 2006;12:904–916.
Sieuwerts AM, Usher PA, Meijer-van Gelder ME, et al. Concentrations of TIMP1 mRNA splice variants and TIMP-1 protein are differentially associated with prognosis in primary breast cancer. Clin Chem 2007;53:1280–1288.
Acknowledgements
We thank the Alpha Foundation for its financial support.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Khoury, T., Kanehira, K., Wang, D. et al. Breast carcinoma with amplified HER2: a gene expression signature specific for trastuzumab resistance and poor prognosis. Mod Pathol 23, 1364–1378 (2010). https://doi.org/10.1038/modpathol.2010.125
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/modpathol.2010.125
Keywords
This article is cited by
-
Therapeutic Effect of pHLIP-mediated CEACAM6 Gene Silencing in Lung Adenocarcinoma
Scientific Reports (2019)
-
Allellic HER-2 codon 655 polymorphism and the influence of plasma HER-2 levels in breast cancer Egyptian female patients
Comparative Clinical Pathology (2014)
-
Expression and clinical significance of carcinoembryonic antigen-related cell adhesion molecule 6 in breast cancers
Breast Cancer Research and Treatment (2013)
-
Simultaneous copy number gains of NUPR1 and ERBB2 predicting poor prognosis in early-stage breast cancer
BMC Cancer (2012)
-
Erythropoietin receptor expression and its relationship with trastuzumab response and resistance in HER2-positive breast cancer cells
Breast Cancer Research and Treatment (2012)
