
Abstract
Celiac disease (CD) is caused by inflammatory CD4+ T-cell responses to dietary gluten. It is unclear whether interleukin (IL)-21 and IL-17A contribute to CD onset and lesion severity; therefore, we investigated IL-21 and IL-17A expression in biopsies from pediatric CD patients with different histopathological scores. High numbers of IL-21-producing cells were observed in pediatric CD lesions, even Marsh 1–2 lesions, whereas increased numbers of IL-17 secreting cells were not observed. Intraepithelial lymphocytes, CD4+ T cells and also neutrophils secreted IL-21. Flow cytometry of lamina propria cells revealed a large population of IL-21- and interferon-γ (IFN-γ)-secreting CD3+ T cells that did not secrete IL-17A. Adult CD patient biopsies also contained high numbers of IL-21-positive cells; however, enhanced numbers of IL-17-positive cells were observed in a small subgroup of patients with severe lesions. As duodenal tissue damage increases contact with microbe-associated molecular patterns, we hypothesized that microbial sensing by Toll-like receptors (TLRs) modulates T cell–derived cytokine secretion. Costimulation with TLR3 ligands during polyclonal T-cell activation significantly increased IL-21 secretion, whereas TLR2 ligands selectively enhanced IL-17A. These results demonstrate that an IL-17A-independent increase in IL-21 production by CD4+ T cells is characteristic of pediatric CD. We hypothesize that incidental IL-17 secretion is caused by tissue damage rather than gluten-specific responses.
Similar content being viewed by others


INTRODUCTION
Celiac disease (CD) is characterized by small intestinal enteropathy with villous atrophy, crypt hyperplasia, and increased numbers of infiltrating lymphocytes in the epithelium and lamina propria. CD4+ T lymphocytes with specificity for dietary gluten drive the mucosal inflammation in CD via the secretion of proinflammatory cytokines. In particular, production of the cytokine interferon-γ (IFN-γ) by gluten-specific CD4+ T cells is thought to play a role in intestinal epithelial damage.1, 2 However, other CD4+ T cell–derived cytokines, in particular interleukin-21 (IL-21), have recently been suggested to contribute to the pathogenesis of CD.3
IL-21 has received increasing attention, as genome-wide association studies for CD identified risk variants in the IL-2/IL-21 gene region.4 Detection of increased IL-21 mRNA expression in duodenal biopsies of untreated adult CD patients has supported a possible role for IL-21 in disease pathogenesis.3 CD4+ T cells,5 natural killer T cells,6 and neutrophils7 have the capacity to secrete IL-21. Isolated lamina propria lymphocytes (LPLs) and intraepithelial lymphocytes (IELs) from CD patients were shown to produce IL-21.8 Additionally, IL-21 can be produced by gluten-reactive CD4+ T cells derived from biopsies of CD patients.9 IL-21 may contribute to intestinal damage via enhancing the production of IFN-γ, as neutralization of IL-21 in gliadin-stimulated biopsy cultures results in reduced IFN-γ production.3 However, IL-21 may be involved in multiple aspects of CD pathogenesis as it can also regulate the growth, survival, and function of B, T, and natural killer cells and limit the differentiation and suppressive capacity of regulatory T cells.10, 11 Currently, the relative frequency, localization, and phenotype of the IL-21-producing cells in CD lesions remain largely unknown. Moreover, the relationship between IL-21 secretion and the severity of intestinal lesions, based on the Marsh score, has not been determined. IL-21 may be derived from different CD4+ T cells. For example, T helper 17 cells (Th17) produce IL-21, in addition to IL-17A, IL-17F, and IL-22,10, 12, 13, 14 and T follicular helper cells15 and T regulatory-1 cells can also produce IL-21.16 As two studies have demonstrated increased expression of IL-17 mRNA in mucosal biopsies from CD patients, compared with biopsies from patients on a gluten-free diet or healthy tissue,17, 18 it is conceivable that Th17 cells are the source of IL-21 in CD. However, this hypothesis is contradicted by the finding that gliadin-specific T cell lines secrete IL-21 but not IL-17.9
To dissect the role of IL-21 in the pathogenesis of CD, we investigated the expression of IL-21 in situ by immunohistochemical staining of small intestinal biopsies from a well-defined cohort of new-onset pediatric CD patients with different histopathological scores.
Furthermore, we phenotyped the IL-21-producing cells by flow cytometric analyses of polyclonally restimulated LPLs and by immunohistochemical staining for IL-17 in small intestinal biopsies from CD patients. Our analysis focused on pediatric CD patients and was aimed at new-onset disease. For comparison, we also analyzed biopsies from adult patients with CD. To obtain insight into the possible causes of the varied patterns of IL-17 release observed in pediatric and adult CD patients, we determined whether particular microbe-associated molecular patterns were involved in enhancing the secretion of IL-17 or IL-21 by CD4+ T cells.
Our results demonstrate that increased IL-21 production is observed in pediatric CD patients, even in lesions with low Marsh scores. The IL-21-secreting cells were mostly CD4+ and secreted IFN-γ and low levels of IL-10, but not IL-17. In a small subgroup of adult patients, IL-17 secretion was more intense. Such incidental increases in IL-17 secretion may be associated with the encounter of Toll-like receptor 2 (TLR2) ligands in lesional tissue, as TLR2 ligation of activated T cells selectively enhanced IL-17 release, whereas TLR3 ligation favored IL-21 release.
RESULTS
Biopsies from pediatric CD patients contain increased numbers of IL-21-producing cells
To investigate the presence of IL-21-secreting cells in situ in biopsies from pediatric CD patients, an IL-21 immunohistochemical detection method was developed for paraffin-embedded tissue. In control tissue biopsies with a Marsh score of 0, only a few IL-21-positive cells were observed in the lamina propria, whereas the isotype control staining was negative (Figure 1a,f). Relative to control tissue with a Marsh score of 0, duodenal mucosa with a Marsh score of 1–3 contained higher numbers of IL-21-secreting cells (Figure 1a–e). The majority of the IL-21-positive cells were randomly distributed within the lamina propria (Figure 1d,e). Quantification of the numbers of IL-21-positive cells demonstrated a significant difference between CD patients with a Marsh score of 1–3 and control patients (P<0.05; Figure 2a). It is noteworthy that even the biopsies from patients with low Marsh scores (Marsh 1–2) contained significantly higher numbers of IL-21-positive cells than the control tissues (Marsh 0). In tissue with Marsh 3B or 3C lesions, IL-21-positive cells were also detected between the epithelial cells. These results are consistent with recent data showing that IL-21 is also produced by IELs in the lesional tissue of CD patients.8 Quantification of these cells on histology revealed increased numbers of IL-21 secreting IELs in tissue with higher Marsh scores (Figure 2b). It should be noted that the number of IL-21 positive IELs varied between patients. Moreover, mildly positive cells were difficult to detect because of background staining in the inflamed tissue. Therefore, flow cytometric analysis was used to confirm that IELs isolated from lesional tissue secreted IL-21 (Figure 2c).

Increased numbers of interleukin-21 (IL-21)-producing cells are observed in biopsies from pediatric celiac disease (CD) patients. (a–e) Immunohistochemical detection of IL-21 in paraffin-embedded duodenal biopsies from (a) a pediatric control patient (Marsh score 0) and CD patients with a (b) Marsh score of 1, (c) Marsh score of 3A, (d) Marsh score of 3B, and (e) Marsh score of 3C. (f) Isotype control antibody staining of a biopsy from a CD patient with a Marsh score of 3B. Original magnification ×20. The images are representative of all 57 CD patients and controls.

Increased numbers of interleukin-21 (IL-21)-positive cells are observed in pediatric celiac disease (CD) mucosa compared with control mucosa. (a) Quantification of the number of IL-21-positive cells in the lamina propria lymphocytes (LPLs) in the different patient groups. Positive cells were counted at an original magnification of ×63 in a field of 6,000 μm2. (b) Quantification of the number of intraepithelial IL-21-positive cells in the different patient groups. Positive cells were counted at an original magnification of ×63 per 500 μm length. The slides were analyzed in blinded manner by two independent investigators. Each point represents a single subject; the horizontal bars represent the mean values. *P<0.05 compared with Marsh score 0, Mann–Whitney U-tests. Intraepithelial lymphocytes (IELs) were isolated from CD patients, the cells were stimulated for 5 h with phorbol 12-myristate 13-acetate (PMA)/ionomycin and Brefeldin, and the expression of intracellular cytokines was detected by flow cytometry. (c) Representative dotplots of isotype staining and IL-21 staining in CD3+ IELs of a Marsh 2 patient.
The majority of IL-21-producing cells coexpress CD4 and IFN-γ
As IL-21 can be produced by CD4+ T cells,5 we performed immunohistochemical double staining for IL-21 and CD4 on paraffin-embedded duodenal biopsies from pediatric CD patients. Double staining for IL-21 and CD4 demonstrated the presence of IL-21 in CD4+ cells (Figure 3a), although CD4neg IL-21+ cells were also detected. Analysis of the CD4neg revealed that polymorphonuclear cells within the lamina propria stained positive for IL-21. CD15+ neutrophils have been shown to have to capacity to secrete IL-21.7 Double staining for CD15 and IL-21 revealed the presence of IL-21+CD15+ cells in CD lesions (Figure 3b). Next, we isolated LPLs from the duodenal biopsies of five pediatric CD patients. IL-21-producing cells were further phenotyped by flow cytometric analysis of freshly isolated phorbol 12-myristate 13-acetate (PMA) and calcium ionophore-restimulated peripheral blood mononuclear cells (PBMCs) and LPLs from the same five pediatric CD patients. IL-21+ LPLs revealed no IL-21 staining in CD3+CD8+ cells, suggesting that the IL-21-producing cells may be CD3+CD4+. Further analysis of the CD3+ population revealed that 92.91±5.16% of the IL-21-producing cells were αβ T cell receptor (TCR) positive, whereas 1.95±0.79% of the IL-21+ cells were γδ TCR positive (Figure 3c). Moreover, the analysis did not reveal strong expression of the T follicular helper cell marker C-X-C chemokine receptor type 5 (CXCR5) in IL-21-secreting cells (data not shown). These data demonstrate that the majority of IL-21-producing T cells in the lamina propria of pediatric CD patients consist of CD3+ αβTCR-positive T cells.

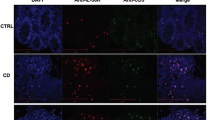
The majority of interleukin-21 (IL-21)-producing cells in celiac disease (CD) biopsies coexpress CD4 and interferon-γ (IFN-γ). (a) Representative immunofluorescent double staining of paraffin-embedded duodenal biopsies from a control patient (Marsh score 0; left) and a CD patient with a Marsh score of 3C (right). Green indicates IL-21 staining, red indicates CD4 staining, and blue indicates 4',6-diamidino-2-phenylindole (DAPI) nuclear counterstaining. Original magnification ×20. (b) Representative immunofluorescent double staining of paraffin-embedded duodenal biopsies from a CD patient with a Marsh score of 3A. Green indicates IL-21 staining, red indicates CD15 staining, and blue indicates DAPI nuclear counterstaining. Original magnification ×20. Peripheral and lamina propria lymphocytes (LPLs) were isolated from five different CD patients. The cells were stimulated for 5 h with phorbol 12-myristate 13-acetate (PMA)/ionomycin and Brefeldin, and the expression of αβ T cell receptor (TCR) and γδ TCR and intracellular cytokines were detected by flow cytometry. (c) Percentage of CD3+IL-21+ LPLs expressing αβ TCR and γδ TCR in 5 CD patients. Data indicate mean±s.d. (d, e) Representative dotplots of double stained cells showing the coexpression of IL-21 and IFN-γ (left panel), IL-21 and IL-17A (middle panel), or IL-21 and IL-10 (right panel) gated using the appropriate isotype control antibodies. Quantitative analysis of the percentage of cytokine-producing cells within the CD3+ population of (f) peripheral blood lymphocytes and (g) lamina propria cells isolated from five CD patients; box and whiskers plot; the horizontal bars represent the mean values.
Next, the expression of Th cell–related cytokines by T cells was determined (Figure 3d–g). In all of the LPL isolates, a clear CD3+IL-21+ population was detected, whereas the population of IL-17A-producing cells was small. Nearly two-thirds of the IL-21-positive cells coexpressed IFN-γ, whereas <12% of the IL-21-positive cells were IL-17A positive. Interestingly, IL-10-producing cells were virtually absent in restimulated LPLs (Figure 3e,g and Supplementary Figure S1 online for isotype stainings). All of the cytokines tested were detectable in PBMCs, including IL-17A, yet similarly to LPLs, only a small percentage of IL-21+IL-17A+ cells could be detected (Figure 3d,f and Supplementary Figure S1 online for isotype stainings). In conclusion, the majority of IL-21-secreting LPLs coexpress IFN-γ but are negative for IL-17 and IL-10.
Increased numbers of IL-17A-producing cells are not observed in biopsies from pediatric CD patients
To establish whether a small number of Th17 cells could be detected in IL-21-positive CD biopsies, immunohistochemical staining for IL-17A was performed in serial sections of the duodenal tissues from the pediatric CD patients. As shown in Figure 4, IL-17A-positive cells were detected in the lamina propria of CD patients and controls. However, in contrast to the increased numbers of IL-21-secreting cells observed with increasing Marsh score, the numbers of IL-17A-positive cells did not vary with the Marsh score (Figure 4a–d). Consequently, quantification of the numbers of IL-17A-positive cells in all biopsies demonstrated no significant difference between CD patients and control tissues (Figure 4f). These data indicate that IL-21 is not produced by Th17 cells in the inflamed tissue of untreated, new-onset pediatric CD patients.

The number of interleukin-17A (IL-17A)-producing cells is not increased in biopsies from pediatric celiac disease (CD) patients. (a–d) Representative IL-17A staining of paraffin-embedded duodenal biopsies from (a) a pediatric control patient (Marsh score 0) and CD patients with a (b) Marsh score of 3A, (c) Marsh score of 3B, and (d) Marsh score of 3C. (e) IL-17A isotype control antibody staining of a biopsy from a CD patient with a Marsh score of 2. Original magnification ×20. The images are representative of all 41 CD patients and controls. (f) Quantification of the number of IL-17A-positive cells in the different pediatric patient groups. Positive cells were counted at an original magnification of ×63 in a field of 6,000 μm2. All slides were analyzed by two independent investigators in a blinded manner. Each point represents a single subject; the horizontal bars represent the mean values. No significant differences were observed between the groups, Mann–Whitney U-test.
Presence of IL-21- and IL-17A-secreting cells in the mucosa of pediatric patients with inflammatory bowel disease
IL-17A-secreting cells are involved in the pathogenesis of inflammatory bowel disease (IBD).19, 20 To detect colocalizing IL-17A- and IL-21-producing cells, intestinal biopsies from pediatric IBD patients diagnosed with Crohn’s disease or ulcerative colitis were immunohistochemically stained for IL-21 and IL-17A. Although most of the biopsies from active IBD patients contained high numbers of IL-21-secreting cells, the localization of IL-21-secreting cells in IBD was different to CD. As previously stated, IL-21-secreting cells were randomly distributed within the lamina propria in CD (Figure 1). In IBD, IL-21-secreting cells were located in the lamina propria, with the appearance of increased numbers of cells in inflamed regions, such as in damaged crypts or ulcerative lesions (Figure 5 a). By costaining serial sections of the same intestinal biopsies for IL-21 and IL-17A, we detected that IL-21-secreting cells co-localized to the same areas of inflamed mucosa as the IL-17A-secreting cells (Figure 5c,d). Quantification of IL-21- and IL-17-secreting cells is depicted in Figure 5i. These findings demonstrate that enhanced, concomitant IL-21 and IL-17A release may be detected in the inflammatory infiltrates of biopsies from pediatric IBD patients.

Presence of interleukin (IL)-21- and IL-17A-secreting cells in the mucosa of pediatric patients with inflammatory bowel disease (IBD). Representative IL-21 and IL-17A staining of serially sectioned paraffin-embedded biopsies from pediatric IBD patients. (a, b) IL-21 staining and (c, d) IL-17A staining of a terminal ileum biopsy from a patient with Crohn’s disease. (e, f) IL-21 staining and (g, h) IL-17A staining of a colon descendens biopsy from a Colitis ulcerosa patient. Original magnification ×20 or ×40. (i) Quantification of the number of IL-21- and IL-17A-positive cells in the IBD patient group. Data from colonic biopsies (n=19) and small intestinal (terminal ileum) biopsies (n=7) of the IBD patient group were combined. Positive cells were counted at an original magnification of ×63 in a field of 6,000 μm2. The slides were analyzed by two independent investigators in a blinded manner. Each point represents a single subject; the horizontal bars represent the mean values.
A small subgroup of adult CD patients exhibits simultaneous expression of IL-21 and IL-17A
To assess whether the enhanced secretion of IL-21 in the absence of increased numbers of IL-17-producing cells was specifically attributed to early-onset CD in children, IL-21 and IL-17A were analyzed using immunohistochemistry in biopsies from a limited number of adult CD patients. Overall, as in pediatric CD, higher numbers of IL-21-secreting cells were observed in the lamina propria of adult CD patients, whereas the numbers of IL-17A-positive cells did not significantly increase with lesion severity. However, a small subgroup of Marsh 3C biopsies contained slightly increased numbers of IL-17A-positive cells (Figure 6a–d). As shown in Figure 6a,c, immunohistochemical staining of IL-21 and IL-17 in serial sections of these few Marsh 3C biopsies with high numbers of IL-17-secreting cells revealed both increased numbers of IL-21- and IL-17A-secreting cells within the same region.

A small subgroup of adult celiac disease (CD) patients exhibit simultaneous expression of interleukin (IL)-21 and IL-17A. (a) IL-21 staining of a biopsy from an adult CD patient with a Marsh score of 3C. (b) Quantification of the number of IL-21-positive cells in the different adult patient groups. (c) IL-17A staining of a serial section of the biopsy shown in b. This adult CD patient biopsy with a Marsh score of 3C was representative of the subgroup that showed increased numbers of IL-17A-positive cells. (d) Quantification of the number of IL-17A-positive cells in the different patient groups. Positive cells were counted at an original magnification of ×63 in a field of 6,000 μm2. All slides were analyzed by two independent investigators. Each point represents a single subject; the horizontal bars represent the mean values. *P<0.05 compared with Marsh score 0, Mann–Whitney U-test.
In conclusion, overall, increased numbers of IL-21-producing cells, but not IL-17A-producing cells, were present in biopsies from adult CD patients, as well as pediatric CD patients. Incidentally, concomitant expression of IL-21 and IL-17 was observed in severe Marsh 3C lesions in biopsies from adult CD patients.
TLR2 and TLR3 ligation on CD4+ T cells differentially enhance the release of IL-17A and IL-21, respectively
As an incidental, concomitant increase in the production of IL-21 and IL-17 was observed in severe CD lesions in biopsies from adult patients, we hypothesized that a bystander stimulus associated with tissue destruction and barrier dysfunction may be involved in the stimulation of IL-17 release. Microbe-associated molecular patterns, e.g. TLR ligands, are released in response to damage and may modulate cytokine release by CD4+ T cells. Previous studies have shown that CD4+ T cells are responsive to microbial stimuli resulting in the modulation of cytokine secretion.21 Therefore, we first investigated which TLRs are expressed by CD4+ T cells. The mRNA expression profile of highly purified CD4+ T cells obtained from healthy donors was determined. Comparison of naive (CD4+CD45RA) and memory (CD4+CD45RO) or total CD4+ T cells to PBMCs revealed that TLR2, TLR3, and TLR7 mRNA were expressed by purified healthy donor-derived naive and memory CD4+ T cells, whereas the expression of TLR4 was very weak or absent (Figure 7a). Next, we investigated whether the production of IL-21 and IL-17 by CD4+ T cells was differentially affected by stimulation with particular TLR ligands. When healthy donor–derived CD4+ T cells were activated for 48 or 120 h in the presence of the TLR3 ligand polyinosinic-polycytidylic acid (poly I:C), a significant increase in IL-21 release, but not IL-17A secretion, was induced (Figure 7b,c and Supplementary Figure S2A online). In contrast, stimulation with the TLR2 ligand Pam3Cys enhanced IL-17A release, but did not alter IL-21 secretion (Figure 7b and Supplementary Figure S2A online). The patterns of cytokine release in response to TLR ligation varied between donors and were more consistent for TLR3 activation (Figure 7c). Activation of CD4+ T cells in the presence of a TLR7 ligand CL097 did not affect IL-21 or IL-17 release (data not shown). Flow cytometric analysis showed no increase in the frequency of IL-21-producing cells after poly I:C stimulation or Pam3Cys stimulation at 48 h (data not shown). However, after 120 h of co-culture with TLR3 ligand, the percentage of IL-21-producing cells, but not of IL-17-producing cells, was increased (Figure 7d). Moreover, stimulation for 120 h with TLR2 ligand enhanced the percentage of IL-17- but not IL-21-producing cells (Figure 7d). It should be noted that the increase in the percentage of cytokine-producing cells was dependent on the strength of the T-cell activation with a ratio of 1 anti-CD3 anti-CD28-coated bead to 4 T cells, giving maximal effect for TLR2-mediated IL-17 responses (Figure 7d and Supplementary Figure S2B online). Furthermore, TLR3 stimulation of highly purified memory (CD45RO) and naive (CD45RA) CD4+ T cells during 48 h of anti-CD3 anti-CD28 activation revealed that memory T cells were the main population of IL-21-secreting cells, whereas no IL-21 secretion by naive T cells was detected (Supplementary Figure S2C online). Further study with different conditions is required to establish whether TLR3 activation affects IL-21 secretion during naive T-cell differentiation. These results demonstrate that ligation of TLR3 during CD4+ T-cell activation acts as a costimulus that enhances IL-21 release but not IL-17 release, whereas ligation of TLR2 enhances IL-17 release but not IL-21 release. As such, the local encounter of TLR ligands within the intestinal lamina propria could modulate cytokine secretion during T-cell activation and elicit cytokine release as a bystander effect to the gliadin-induced cytokine response.

Toll-like receptor 3 (TLR3) ligation enhances the release of interleukin-21 (IL-21), but not IL-17A, by CD4+ T cells. (a) Expression of TLR2, TLR3, TLR4, and TLR7, and glyceraldehyde 3-phosphate dehydrogenase (GAPDH) mRNA was determined in highly purified healthy donor-derived cell-sorted CD4 cells, CD4+CD45RA cells, CD4+CD45RO cells, and peripheral blood mononuclear cells (control) using PCR. Data from one of two representative experiments are shown. (b, c) CD4+ T cells were purified from six healthy donors by depletion of non-CD4+ T cells using magnetically labeled antibodies (Dynal). The isolated CD4+ T cells were activated in culture using anti-CD3 anti-CD28 beads (Dynabeads) in a ratio of 1 bead per 2 T cells in the absence (control) or presence of polyinosinic-polycytidylic acid (poly I:C; 25 μg ml−1) and/or Pam3Cys (1 μg ml−1). After 48 h, the supernatants were collected and the secretion of IL-21 and IL-17A protein were measured using enzyme-linked immunosorbent assays (ELISAs). (b) IL-21 and IL-17A response in the activated CD4+ T cells of a single representative individual. (c) Cytokine release by activated CD4+ T cells in response to TLR stimulation, expressed as the percentage increase compared with control anti-CD3 anti-CD28 bead stimulation. Each dot represents a single individual; the horizontal bars represent the mean values. (d) After 120 h of culture, the CD4+ T cells were reactivated for 5 h with phorbol 12-myristate 13-acetate (PMA; 0.05 μg ml−1) and ionomycin (0.5 μg ml−1) in the presence of Brefeldin A for the last 4 h. The cells were harvested, fixed, permeabilized, stained for IL-21 and IL-17A, and analyzed by flow cytometric analysis. The percentage of cytokine-secreting cells in response to TLR stimulation is expressed as the percentage increase compared with control anti-CD3 anti-CD28 bead stimulation. Each dot represents a single individual; the horizontal bars represent the mean values. Data are representative of two independent experiments using cells from three different donors; *P<0.05 vs. control (n=3), paired t-tests.
DISCUSSION
In this study we investigated the role of IL-21-producing cells in pediatric CD using two complementary methods, i.e., direct immunohistochemical analysis of biopsies and intracellular flow cytometric analysis of freshly isolated LPLs. This study demonstrates that increased numbers of IL-21-producing cells were present in the lamina propria of the small intestine in pediatric CD patients ranging in age from 1 to 11 years (mean, 4.9), compared with non-CD control patients. Phenotypically, the IL-21+ cells were predominantly CD4+ αβTCR+ T cells, of which the majority coproduced IFN-γ but not IL-17 or IL-10.
Previously, it has been shown that the expression of IL-21 is upregulated in the small intestinal mucosa of adult CD patients as compared with healthy controls. In particular, in adult CD patients, IELs and LPLs were shown to produce IL-21.3, 8 Here, we show for the first time that increased numbers of IL-21-producing cells can readily be detected in situ in the lamina propria of early-diagnosed CD patients. Extensive analysis of this cohort of pediatric patients demonstrated that high numbers of IL-21-positive cells were already present in biopsies with mild lesions with a Marsh score of 1–2. Not only CD3+αβ TCR+ lymphocytes and IELs secreted IL-21, but also a population of neutrophilic IL-21-secreting cells was detected on histology. Neutrophils have recently been shown to have IL-21-secreting capacity.7 These B cell–helper neutrophils were reported to stimulate diversification and production of immunoglobulin in the marginal zone of the spleen. In CD, neutrophilic influx has been reported previously.22 Whether IL-21-secreting neutrophils in the celiac lesion have a specific function in B-cell stimulation will need to be investigated. Using serial tissue sections of our pediatric CD patient cohort, we established that the number of IL-17-secreting cells did not increase with disease score and remained comparable with nondiseased control tissues. Previous studies that used different cell culture techniques to study the role of IL-21 and IL-17 in CD have led to discrepancies regarding the role of IL-17-producing cells in the pathogenesis of CD.9, 18 In one study, biopsy-derived purified T cells from CD patients contained an increased percentage of IL-17-producing cells, and stimulation of these cells with gliadin for 5 days led to increased IL-17 mRNA expression.23 In a second study, a combination of intracellular cytokine staining with DQ2-α-II-gliadin peptide tetramer staining revealed that polyclonal T cell lines derived from CD biopsies contain IL-17-secreting cells; however, the gluten-reactive T cells that produced IL-21 and IFN-γ were IL-17 negative.9 These data infer that differences in the technical approaches yield different interpretations of the role of Th17 cells in CD pathogenesis. The advantage of immunohistochemistry is that it circumvents the possible pitfall of selective survival of T-cell subsets in culture. Therefore, our data establish that IL-21 secretion occurs independently of IL-17 release in early-onset CD. It should be noted that increased numbers of IL-17A-positive cells were detected in the inflamed mucosa of pediatric IBD patients, and IL-17A-positive cells colocalized with IL-21-positive cells in the infiltrates of IBD lesions, in line with the role of Th17 cells in the pathogenesis of IBD.19, 24 To further confirm our findings, we performed polyclonal restimulation of freshly isolated lamina propria cells from newly diagnosed pediatric patients with phorbol ester and calcium ionophore, and demonstrated that a large majority of lamina propria IL-21-secreting CD4+ T cells produced IFN-γ; however, few IL-17-producing cells were detected. Our data show that no increase in the number of IL-17-producing cells is detected in pediatric CD, irrespective of TCR specificity. These data agree with a recent study demonstrating that human leukocyte antigen (HLA)-DQ2-restricted gluten-reactive CD4+ T cell lines derived from adult CD patients produce IFN-γ and IL-21, but not IL-17.9
Having established that IL-21-producing cells predominate in Marsh 1–2 CD lesions, and the numbers of IL-17-producing cells did not increase with Marsh score in young, newly diagnosed CD patients, it was questioned whether the pattern of IL-21- and IL-17-producing cells changed with age at diagnosis. Indeed, increased numbers of IL-21-secreting cells and low numbers of IL-17-positive cells were also detected in biopsies from adult CD patients. However, the number of IL-17-secreting cells in adult CD biopsies was more variable. In particular, a subgroup of adult patient biopsies with Marsh scores of 3C had higher numbers of IL-17-producing cells. Mucosal IL-17A-producing cells contribute to protective antimicrobial responses and epithelial barrier integrity.25 Therefore, a possible explanation for the incidental increase in IL-17 secretion observed in the biopsies from our adult CD cohort may be that IL-17 is secreted in response to bacterial triggers in damaged tissue, but is not directly related to the gluten-specific T-cell response. As CD4+ T cells express TLRs (Figure 7) and have been shown to respond to TLR stimulation,21 we hypothesized that an incidental increase in IL-17 production by CD4+ T cells may be stimulated by TLR ligation. Indeed, our data demonstrated that stimulation of CD4+ T cells with the TLR2 ligand Pam3Cys favored the release of IL-17 but not IL-21. A technical consequence of our finding is that TLR ligand contamination should be ruled out in digested gliadin restimulation cultures, to ensure gliadin-specific restimulation effects in T cells.
Further analysis of TLR stimulation revealed that stimulation with the TLR3 ligand during CD4+ T-cell activation enhanced IL-21 release but not IL-17 release. TLR3 is activated by double-stranded RNA from viruses26 and mRNA released from necrotic cells27 that has relevance for CD, as an epidemiological study showed that repeated infections with rotavirus, a double-stranded RNA virus, may increase the risk of CD autoimmunity in childhood.28 Moreover, poly (I:C) is a synthetic double-stranded RNA TLR3 ligand that, when injected into mice, results in transient activation of tissue transglutaminase-2 and villous atrophy in the small intestine, both hallmarks of human CD enteropathy.29, 30 The fact that enhanced IL-21 release is mediated by TLR3, but not TLR2 ligation, in CD4+ T cells strengthens the hypothesis that the pattern of CD inflammation has the signature of a TLR3-mediated response. It should be noted that TLR3 ligation acts as a cofactor enhancing IL-21. A TCR signal is a prerequisite for the production of IL-21 as culture of T cells with TLR3 alone did not yield detectable IL-21 release (data not shown). As activation of T cells in the presence of TLR3 ligand enhanced the percentage of IL-21-secreting cells in vitro, we hypothesize that TLR3 ligation in response to tissue damage may play a possible role in specifically perpetuating the IL-21-driven inflammation in CD.
In summary, this study demonstrates that increased numbers of IL-21-secreting CD4+ T cells in the lamina propria are characteristic for CD and are even detectable in mild lesions. Our data, together with existing knowledge, argue that IL-21 plays a causative role in the pathogenesis of CD. IL-21 is a pleiotropic cytokine that, in cooperation with cytokines such as IL-15, may be involved in multiple inflammatory pathways. IL-21 may be an important enhancer of IFN-γ production in CD4+ T cells, as blocking of IL-21 activity in CD mucosal biopsy cultures reduced IFN-γ secretion.3 With respect to IELs, IL-21 may be involved in increasing the number of intraepithelial CD8+ T cells, as overexpression of IL-21 in mice selectively enhances the accumulation of memory CD8+ T cells.31 IL-21 may also contribute to CD-associated autoantibody production, as IL-21 acts directly on B cells to regulate Bcl-6 (B-cell lymphoma 6) expression and germinal center responses.32 As IL-21 has been shown to increase the resistance of inflammatory T cells to regulatory T cells in an in vitro culture system,11 IL-21 may be involved in inhibition of the anti-inflammatory response in CD. Future studies are required to determine the precise role of IL-21 in the course of CD development.
METHODS
Patients and controls. Pediatric patients (age 1–11 years, mean 4.9) with a suspected diagnosis of CD who underwent an esophagogastroduodenoscopy at Erasmus MC–Sophia Children’s Hospital (Rotterdam, The Netherlands) were approached for participation in this study. After diagnosis, the patients with biopsy-proven CD were included in the patient group, whereas children with a normal intestinal histology and negative autoantibodies were included in the control group. Patients diagnosed with other diseases were excluded from the study. The histopathological grade of the duodenal biopsies was based on the Marsh score33 (Marsh 0, n=10; Marsh 1, n=9; Marsh 2, n=2; Marsh 3A, n=8; Marsh 3B, n=11; and Marsh 3C, n=12). All CD patients had positive serum anti-endomysium and/or anti-transglutaminase-2 antibodies. For comparison, intestinal biopsies from children with IBD diagnosed with Colitis ulcerosa (n=10) or Crohn’s disease (n=9) were also obtained (age 7–18 years, mean 13.9). The study received ethical approval from the local Ethics Committee (Erasmus MC, Rotterdam, The Netherlands) and the parents or guardians of all patients provided signed informed consent.
Immunohistochemistry on paraffin sections. For immunohistochemistry, the sections were deparaffinized and endogenous peroxidases were quenched with 3% H2O2 in methanol for 20 min. Antigen retrieval was performed by microwave treatment in citrate buffer (10 mM, pH 6.0). The sections were blocked for 1 h in 10% normal human serum diluted in 10 mM Tris, 5 mM EDTA, 0.15 M NaCl, 0.25% gelatine, and 0.05% Tween-20, pH 8. Antibody incubation was performed overnight at 4 °C using anti-IL-17A (1:50; R&D Systems, Abingdon, UK) or anti-IL-21 (1:100; Lifespan Biosciences, Seattle, WA). Immunoreactive sites were detected with biotinylated secondary rabbit anti-goat or goat anti-rabbit serum using the Vectastain ABC Elite Kit (Vector Laboratories, Burlingame, CA) and 3,3′-diaminobenzidine tetrahydrochloride (Sigma-Aldrich, Zwijndrecht, The Netherlands), and the nuclei were counterstained with hematoxylin (Vector Laboratories).
For double immunofluorescent staining, anti-IL-21 and anti-CD4 Ab-8 (Thermo Scientific, Fremont, CA) or anti-CD15 (BD Biosciences, Breda, The Netherlands) were used followed by goat anti-rabbit secondary antibody fluorescently labeled with DyLight-488 or goat anti-mouse secondary antibody labeled with DyLight-594 (Thermo Scientific). The sections were mounted in medium for fluorescence containing 4′,6-diamidino-2-phenylindole (Vector Laboratories). An isotype-matched negative control was performed for each immunostaining. The positive cells were counted by two independent investigators in a field of 6,000 μm2.
Images were acquired and analyzed using a Leica DM5500B upright microscope and LAS-AF image acquisition software (Leica Microsystems, Rijswijk, The Netherlands).
Lymphocyte isolation. PBMCs were isolated using a Ficoll-Hypaque gradient. CD4+ T cells from 6 CD patients (Marsh score >3A) were purified by negative depletion using magnetically labeled antibodies (Dynabeads; Invitrogen, Carlsbad, CA) according to the manufacturer’s instructions. LPLs or IELs were isolated from the duodenal samples of five CD patients, as previously described.34 The average yield of LPLs was approximately 1–1.5 × 106 cells per patient.
TLR expression on purified T cells. CD4+ T cells, CD4+CD45RA+ T cells, and CD4+CD45RO+ T cells were purified from PBMCs obtained from a healthy donor using flow cytometric cell sorting; the purity of the populations was 99, 99, and 90%, respectively. Total RNA was purified from the sorted T cells and nonsorted PBMCs (control) using the NucleoSpin RNA XS kit (Machery-Nagel, Düren, Germany). Up to 1 μg RNA was reverse transcribed to single-stranded complementary DNA using a mix of random hexamers (2.5 μM) and oligo(dT) primers (20 nM). The reverse transcription reaction was performed in a total volume of 25 μl containing 0.2 mM of each dNTP (Amersham Pharmacia BioTech, Piscataway, NJ), 200 U Moloney murine leukemia virus reverse transcriptase (Promega, Madison, WI) and 25 U RNAsin (Promega). The conditions for the reverse transcription reaction were 37 °C for 30 min, 42 °C for 15 min, and 94 °C for 5 min. The complementary DNA was diluted fivefold and stored at −20 °C. Conventional PCR or real-time quantitative PCR using the AbiPrismR 7900 Sequence Detection System (PE Applied Biosystems, Foster City, CA) using general fluorescence-based detection with SYBR green were performed using the specific primers listed below. The PCR products were purified and visualized by agarose gel electrophoresis.
TLR primers. Specific primers were designed across different constant region exons resulting in the following primers: GAPDH: forward 5′-GTCGGAGTCAACGGATT-3′, reverse 5′-AAGCTTCCCGTTCTCAG-3′; TLR2: forward 5′-GCTGGTGGCAATAACTTC-3′, reverse 5′-AGGCCCACATCATTTTC-3′; TLR3 forward 5′-GCACGAATTTGACTGAACT-3′, reverse 5′-TCCAATTGCGTGAAAAC-3′; TLR4 forward 5′-CCTGGACCTGAGCTTTAAT-3′, reverse 5′-CCACCAGCTTCTGTAAACTT-3′; TLR7 forward 5′-CTGCCCTGTGATGTCACT-3′, reverse 5′-CGCTGGGGAGATGTCT-3′.
Cell culture and cytokine analysis. Isolated CD4+ T cells were activated in culture using anti-CD3 anti-CD28 beads (Dynabeads, Invitrogen) in the absence (control) or presence of 1 μg ml−1 Pam3Cys (EMC Microcollections, Tübingen, Germany), 25 μg ml−1 poly I:C (Sigma-Aldrich), 5 μg ml−1 lipopolysaccharide (Sigma-Aldrich), or 5 μg ml−1 of the imidazoquinoline-derivative CL097 (Invivogen, San Diego, CA). After 48 and 120 h, the concentrations of IL-21 and IL-17A in the cell supernatants were measured using the Ready-SET-go! Kit (eBiosciences, San Diego, CA) and Duoset (R&D Systems) enzyme-linked immunosorbent assays, respectively.
Flow cytometry. PBMCs and LPLs were reactivated for 5 h with 0.05 μg ml−1 phorbol 12-myristate 13-acetate (Sigma-Aldrich) and 0.5 μg ml−1 ionomycin (Sigma-Aldrich) in the presence of Brefeldin A for the last 4 h (3 μg ml−1; eBiosciences). After reactivation, the cells were stained for flow cytometry using monoclonal antibodies against CD3, CD4, CD8, αβ TCR, and γδ TCR (all from BD Biosciences), fixed with 2% formalin solution, and intracellular staining was performed using saponin (Sigma-Aldrich), followed by IL-21 (eBiosciences), IL-17A (eBiosciences), IFN-γ (BD Biosciences), IL-10 (BD Biosciences), or the appropriate isotype controls (all from eBiosciences). Flow-cytometric analysis was performed using the FACSCanto II (BD Biosciences).
Statistics. Prism (Graphpad Software, La Jolla, CA) was used to perform statistical analysis using paired sample t-tests or the Mann–Whitney U-test, as indicated in the figure legends. The P-values of <0.05 were considered statistically significant.
References
Green, P.H. & Cellier, C. Celiac disease. N. Engl. J. Med. 357, 1731–1743 (2007).
Nilsen, E.M. et al. Gluten induces an intestinal cytokine response strongly dominated by interferon gamma in patients with celiac disease. Gastroenterology 115, 551–563 (1998).
Fina, D. et al. Interleukin 21 contributes to the mucosal T helper cell type 1 response in coeliac disease. Gut 57, 887–892 (2008).
van Heel, D.A. et al. A genome-wide association study for celiac disease identifies risk variants in the region harboring IL2 and IL21. Nat. Genet. 39, 827–829 (2007).
Parrish-Novak, J., Dillon, S.R., Nelson, A., Hammond, A., Sprecher, C., Gross, J.A. et al. Interleukin 21 and its receptor are involved in NK cell expansion and regulation of lymphocyte function. Nature 408, 57–63 (2000).
Coquet, J.M. et al. IL-21 is produced by NKT cells and modulates NKT cell activation and cytokine production. J. Immunol. 178, 2827–2834 (2007).
Puga, I. et al. B cell-helper neutrophils stimulate the diversification and production of immunoglobulin in the marginal zone of the spleen. Nat. Immunol. 13, 170–180 (2012).
Sarra, M. et al. IL-15 positively regulates IL-21 production in celiac disease mucosa. Mucosal. Immunol. 6, 244–255 (2012).
Bodd, M. et al. HLA-DQ2-restricted gluten-reactive T cells produce IL-21 but not IL-17 or IL-22. Mucosal. Immunol. 3, 594–601 (2011).
Nurieva, R. et al. Essential autocrine regulation by IL-21 in the generation of inflammatory T cells. Nature 448, 480–483 (2007).
Peluso, I. et al. IL-21 counteracts the regulatory T cell-mediated suppression of human CD4+ T lymphocytes. J. Immunol. 178, 732–739 (2007).
Harrington, L.E. et al. Interleukin 17-producing CD4+ effector T cells develop via a lineage distinct from the T helper type 1 and 2 lineages. Nat. Immunol. 6, 1123–1132 (2005).
Park, H. et al. A distinct lineage of CD4 T cells regulates tissue inflammation by producing interleukin 17. Nat. Immunol. 6, 1133–1141 (2005).
Ivanov, I.I. et al. The orphan nuclear receptor RORgammat directs the differentiation program of proinflammatory IL-17+ T helper cells. Cell 126, 1121–1133 (2006).
O'Shea, J.J. & Paul, W.E. Mechanisms underlying lineage commitment and plasticity of helper CD4+ T cells. Science 327, 1098–1102 (2010).
Pot, C. et al. Cutting edge: IL-27 induces the transcription factor c-Maf, cytokine IL-21, and the costimulatory receptor ICOS that coordinately act together to promote differentiation of IL-10-producing Tr1 cells. J. Immunol. 183, 797–801 (2009).
Castellanos-Rubio, A., Santin, I., Irastorza, I., Castano, L., Carlos Vitoria, J. & Ramon Bilbao, J. TH17 (and TH1) signatures of intestinal biopsies of CD patients in response to gliadin. Autoimmunity 42, 69–73 (2009).
Monteleone, I. et al. Characterization of IL-17A-producing cells in celiac disease mucosa. J. Immunol. 184, 2211–2218 (2010).
Fujino, S. et al. Increased expression of interleukin 17 in inflammatory bowel disease. Gut 52, 65–70 (2003).
Brand, S. Crohn’s disease: Th1, Th17 or both? The change of a paradigm: new immunological and genetic insights implicate Th17 cells in the pathogenesis of Crohn's disease. Gut 58, 1152–1167 (2009).
Kabelitz, D. Expression and function of Toll-like receptors in T lymphocytes. Curr. Opin. Immunol. 19, 39–45 (2007).
Beitnes, A.C., Raki, M., Brottveit, M., Lundin, K.E., Jahnsen, F.L. & Sollid, L.M. Rapid accumulation of CD14+CD11c+ dendritic cells in gut mucosa of celiac disease after in vivo gluten challenge. PLoS One 7, e33556 (2012).
Fernandez, S. et al. Characterization of gliadin-specific Th17 cells from the mucosa of celiac disease patients. Am. J. Gastroenterol. 106, 528–538 (2011).
Nielsen, O.H., Kirman, I., Rudiger, N., Hendel, J. & Vainer, B. Upregulation of interleukin-12 and -17 in active inflammatory bowel disease. Scand. J. Gastroenterol. 38, 180–185 (2003).
Korn, T., Bettelli, E., Oukka, M. & Kuchroo, V.K. IL-17 and Th17 Cells. Annu. Rev. Immunol. 27, 485–517 (2009).
Alexopoulou, L., Holt, A.C., Medzhitov, R. & Flavell, R.A. Recognition of double-stranded RNA and activation of NF-kappaB by Toll-like receptor 3. Nature 413, 732–738 (2001).
Kariko, K., Ni, H., Capodici, J., Lamphier, M. & Weissman, D. mRNA is an endogenous ligand for Toll-like receptor 3. J. Biol. Chem. 279, 12542–12550 (2004).
Stene, L.C., Honeyman, M.C., Hoffenberg, E.J., Haas, J.E., Sokol, R.J., Emery, L. et al. Rotavirus infection frequency and risk of celiac disease autoimmunity in early childhood: a longitudinal study. Am. J. Gastroenterol. 101, 2333–2340 (2006).
Siegel, M., Strnad, P., Watts, R.E., Choi, K., Jabri, B., Omary, M.B. et al. Extracellular transglutaminase 2 is catalytically inactive, but is transiently activated upon tissue injury. PLoS One 3, e1861 (2008).
Zhou, R., Wei, H., Sun, R., Zhang, J. & Tian, Z. NKG2D recognition mediates Toll-like receptor 3 signaling-induced breakdown of epithelial homeostasis in the small intestines of mice. Proc. Natl. Acad. Sci. USA 104, 7512–7515 (2007).
Allard, E.L. et al. Overexpression of IL-21 promotes massive CD8+ memory T cell accumulation. Eur J Immunol 37, 3069–3077 (2007).
Linterman, M.A. et al. IL-21 acts directly on B cells to regulate Bcl-6 expression and germinal center responses. J. Exp. Med. 207, 353–363 (2010).
Marsh, M.N. Gluten, major histocompatibility complex, and the small intestine. A molecular and immunobiologic approach to the spectrum of gluten sensitivity ('celiac sprue'). Gastroenterology 102, 330–354 (1992).
Cerf-Bensussan, N., Guy-Grand, D. & Griscelli, C. Intraepithelial lymphocytes of human gut: isolation, characterisation and study of natural killer activity. Gut 26, 81–88 (1985).
Acknowledgements
We thank L.A. van Berkel and Y. Simons-Oosterhuis for technical assistance, Dr L. de Ridder, Dr J. Hulst, Dr B. de Koning, and M. Landman-de Goeij for their help in patient recruitment, and Professor Dr N. Cerf-Bensussan for providing the protocol for LPL isolation. Professor Dr F. Koning and Dr S. Veenbergen are thanked for critical reading of the manuscript. This research was funded by the Dutch Sophia Research Foundation grant 557 and the Dutch Celiac Disease Consortium (CDC2). The Sponsors had no active role in the study design, data collection, or analysis.
Author contributions
M.A. van Leeuwen: planning, conducting the study, interpreting data, and drafting the manuscript; D.J. Lindenbergh-Kortleve, H.C. Raatgeep, and L.F. de Ruiter: conducting the study; R.R. de Krijger and M. Groeneweg: collecting the data, planning, and interpreting data; J.C. Escher: collecting the data, planning, interpreting the data, and drafting of the manuscript; J.N. Samsom: collecting the data, planning, interpreting the data, drafting of the manuscript, and full responsibility for the study. All authors have approved the final draft submitted.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declared no conflict of interest.
Additional information
SUPPLEMENTARY MATERIAL is linked to the online version of the paper
Rights and permissions
About this article
Cite this article
van Leeuwen, M., Lindenbergh-Kortleve, D., Raatgeep, H. et al. Increased production of interleukin-21, but not interleukin-17A, in the small intestine characterizes pediatric celiac disease. Mucosal Immunol 6, 1202–1213 (2013). https://doi.org/10.1038/mi.2013.19
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/mi.2013.19
This article is cited by
-
IL-10 signaling prevents gluten-dependent intraepithelial CD4+ cytotoxic T lymphocyte infiltration and epithelial damage in the small intestine
Mucosal Immunology (2019)
-
Macrophage-mediated gliadin degradation and concomitant IL-27 production drive IL-10- and IFN-γ-secreting Tr1-like-cell differentiation in a murine model for gluten tolerance
Mucosal Immunology (2017)
-
In the Intestinal Mucosa of Children With Potential Celiac Disease IL-21 and IL-17A are Less Expressed than in the Active Disease
American Journal of Gastroenterology (2016)
-
Coeliac disease and rheumatoid arthritis: similar mechanisms, different antigens
Nature Reviews Rheumatology (2015)
-
Interleukin-21: a double-edged sword with therapeutic potential
Nature Reviews Drug Discovery (2014)
