
Abstract
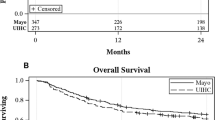
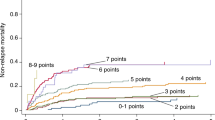
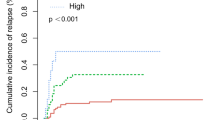
The refined disease risk index (DRI) is a powerful prognostic model based solely on the disease type and stage for predicting survival outcomes of various hematological malignancies after allogeneic transplant. Here, we analyzed our series of 690 patients transplanted over the past 15 years, and showed that besides overall survival (OS), the refined DRI is also able to segregate event-free survival and relapse mortality in our cohort of largely Southeast Asian patients with a long and complete follow-up. Stratification by refined DRI remains statistically significant even when broken down by specific diseases each with a smaller number of patients, as well as for a small subset of patients younger than 18 years old, providing a robust model for prognostication. Multivariable analysis shows that refined DRI, age, year of transplant and donor type are independent risk factors for OS. We further demonstrated here that prognostication for a given patient with a specific disease can be made more discriminating by integrating independent risk factors such as age and donor type with the refined DRI. The future development of prognostic system incorporating the refined DRI with patient- and transplant-related risk factors will provide a more precise estimate of transplant outcome.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others
References
Sorror ML, Maris MB, Storb R, Baron F, Sandmaier BM, Maloney DG et al. Hematopoietic cell transplantation (HCT)-specific comorbidity index: a new tool for risk assessment before allogeneic HCT. Blood 2005; 106: 2912–2919.
Sorror ML, Storb RF, Sandmaier BM, Maziarz RT, Pulsipher MA, Maris MB et al. Comorbidity-age index: a clinical measure of biologic age before allogeneic hematopoietic cell transplantation. J Clin Oncol 2014; 32: 3249–3256.
Gratwohl A, Stern M, Brand R, Apperley J, Baldomero H, de Witte T et al. Risk score for outcome after allogeneic hematopoietic stem cell transplantation: a retrospective analysis. Cancer 2009; 115: 4715–4726.
Armand P, Gibson CJ, Cutler C, Ho VT, Koreth J, Alyea EP et al. A disease risk index for patients undergoing allogeneic stem cell transplantation. Blood 2012; 120: 905–913.
Armand P, Kim HT, Logan BR, Wang Z, Alyea EP, Kalaycio ME et al. Validation and refinement of the Disease Risk Index for allogeneic stem cell transplantation. Blood 2014; 123: 3664–3671.
European Group for Blood and Marrow Transplantation. Definitions and evaluation of endpoints following stem cells transplantation - recommendation from the European Group for Blood and Marrow transplantation (EBMT). Available at https://portal.ebmt.org/sites/clint2/clint/Documents/Statistical%20Endpoints_CLINT%20Project_final%20version.pdf. Accessed on 19 June 2016.
Bacigalupo A, Ballen K, Rizzo D, Giralt S, Lazarus H, Ho V et al. Defining the intensity of conditioning regimens: working definitions. Biol Blood Marrow Transplant 2009; 15: 1628–1633.
Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia. Blood 2016; 127: 2391–2405.
Beauverd Y, Roosnek E, Tirefort Y, Nagy-Hulliger M, Bernimoulin M, Tsopra O et al. Validation of the disease risk index for outcome of patients undergoing allogeneic hematopoietic stem cell transplantation after T cell depletion. Biol Blood Marrow Transplant 2014; 20: 1322–1328.
Lim AB, Roberts AW, Mason K, Bajel A, Szer J, Ritchie DS et al. Validating the allogeneic stem cell transplantation disease risk index: sample size, follow-up, and local data are important. Transplantation 2015; 99: 128–132.
McCurdy SR, Kanakry JA, Showel MM, Tsai HL, Bolaños-Meade J, Rosner GL et al. Risk-stratified outcomes of nonmyeloablative HLA-haploidentical BMT with high-dose posttransplantation cyclophosphamide. Blood 2015; 125: 3024–3031.
Lupo-Stanghellini MR, Sala E, Piemontese S, Morelli M, Greco R, Marcatti M et al. Refined Disease Risk Index (DRI) and Hematopoietic Cell Transplantation Comorbidity Index (HCT-CI) predict survival after haploidentical stem cell transplantation: a comparative study with EBMT risk score in 220 consecutive patients. Blood 2015; 126: 4400.
Aoki J, Yamamoto E, Fujii E, Tanaka M, Kanamori H . Validation of the Refined Disease Risk Index in Patients Receiving Allogeneic Stem Cell Transplantation at a Single Center in Japan. Biol Blood Marrow Transplant 2016; 22: S302–S303.
Acknowledgements
VVM thanks the Singapore General Hospital Post Graduate Medical Institute for funding and the MS Ramaiah Medical college for clinical fellowship attachment in the Department of Haematology at the Singapore General Hospital.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies this paper on Bone Marrow Transplantation website
Supplementary information
Rights and permissions
About this article

Cite this article
Maka, V., Koh, LP., Diong, C. et al. An exploration of the applicability of the refined disease risk index and its integration with other independent risk factors for individualized prognostication. Bone Marrow Transplant 52, 363–371 (2017). https://doi.org/10.1038/bmt.2016.286
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bmt.2016.286
