
Abstract
Study design
Double blind randomised controlled trial
Intervention
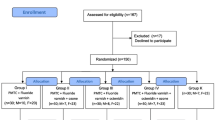
Sixty patients undergoing orthodontic treatment were randomised to receive either MI Paste Plus (GC America, Alsip III) or a placebo paste (Tom's of Main, Salisbury, UK). To be included, the patients had to be 12 years of age or over, in the permanent dentition, and be considered to be compliant with using the paste. Patients were excluded if they; had been undergoing extensive fluoride regimes, had an impacting medical or dental condition, had been receiving fluoride treatment for white spots, be planning to move within 6 months, or have an allergy to IgE casein. The pastes were self-administered in a fluoride tray for 3 to 5 minutes each night after brushing, for a period of 3 months.
Outcome measures
Outcomes were measured at baseline, then at 4, 8, and 12 weeks into treatment) using 2 measures. Standardised photographic records were used to assess WSLs using Banks and Richmond's decalcification index score, from first premolar to first premolar in the maxilla and mandible. Three operators scored the photographs independently. The International Caries Detection and Assessment System (ICDAS) was used for the labial surfaces of the teeth and the scores (0-6) for surfaces were added together to give an overall score.
Results
Five patients refused to participate before the trial began and out of the 60 patients randomised, 50 completed the study (26 MI Paste Plus group 24 in placebo group). There was a 53.5% in the enamel decalcification index score in the MI Paste Plus group but an increase of 91.1% in the placebo group at the end of the 12 week period; ICDAS scores were added together to give an overall score for all teeth; the MI Paste Plus group score was 145 at baseline and 80 after 12 weeks, a 44.8%reduction; in the placebo group, the scores were 116 and 166 respectively, an increase of 43%.
Conclusions
MI Paste Plus prevented and decreased the number of WSLs during orthodontic treatment with the placebo paste group having an increase in the number of WSLs during the trial. These effects were most noticeable on the gingival surfaces. Incisal enamel decalcification index scores were consistently higher than other tooth surfaces, including gingival.
Similar content being viewed by others

Commentary
The incidence of enamel demineralisation in patients undergoing fixed orthodontic treatment ranges from 2-96%.1 A number of investigated preventative measures have been reported in the literature. The title of this article suggests it will explore the use of MI Paste Plus to prevent demineralisation in orthodontic patients. However, the effect on both formation and resolution of white spot lesions are considered. It is difficult to determine whether the results of this paper are clinically relevant owing to lack of important information and some fundamental design flaws.
The type of orthodontic treatment being undertaken is not specified. Furthermore, the photographs in the article show different bracket systems being used, even within the same patient. This lack of standardisation may affect the likelihood of plaque accumulating and influence plaque control and therefore decalcification. In addition, certain ligation methods can be associated with higher levels of bacteria introducing another potential variable.2
Compliance with instructions on paste usage was likely to be greater than would be seen in the general population as only ‘carefully selected’ patients, considered likely to be compliant in use of the MI plus paste, were invited to join. This casts doubt on how transferable the findings are to routine clinical practice. Participants brushed their teeth and applied the tray containing the paste, however, it is not specified whether the participants’ toothpaste was standardised, or what concentration of fluoride it contained as the inclusion criteria simply states patients “who had not extensively used fluoride regimes” were recruited. Clarity on this would again help with applying the results of this study to clinicians’ own patients.
This study was carried out with fixed appliances in situ, which could have made it difficult to identify white spot lesions on the teeth, particularly those closely related to the bracket base. It is not stated whether arch wires and auxiliaries were removed at review appointments to improve visualisation of the teeth.
This article compares the effects of MI Paste Plus, which contains both CPP-ACP and fluoride, to a placebo paste, Tom's of Maine. The authors did not specify which of the Tom's of Maine range was used, however, we found this clarified in a response to a letter about the paper3. This makes it difficult to ascertain whether the effect obtained from using MI Paste Plus in this study is due to the CPP-ACP or fluoride content or both.
In summary, whilst at first appearing to provide compelling evidence, this trial in itself is not sufficiently convincing to advocate the use of MI Paste Plus to prevent or remineralise white spot lesions during orthodontic treatment, due to the limitations discussed and given that there is good evidence for cheaper, easier methods already established. It may be useful however, for the clinician to consider its adjunctive use in very compliant patients (although these are ones who are less likely to need it) and the high caries risk patients with additional needs. Clinicians should also be aware that it is thought to be sufficient to use MI Paste Plus by rubbing it around the brackets rather than using a tray for delivery, and this might improve compliance.
References
Mitchell L : Decalcification during orthodontic treatment with fixed appliances - an overview. Br J Orthod 1992; 19:199–205.
Forsberg CM, Brattstrom V, Malmberg E, Nord CE . Ligature wires and elastomeric rings: two methods of ligation, and their association with microbial colonization of Streptococcus mutans and lactobacilli. Eur J Orthod 1991; 13: 416–420.
Johnson D . MI Paste Plus research. Am J Orthod Dentofacial Orthop 2012; 141: 526.
Author information
Authors and Affiliations
Additional information
Address for correspondence: Chung How Kau, Department of Orthodontics, University of Alabama at Birmingham, 1919 7th Ave S, SDB 305, Birmingham, AL 35294, USA. E-mail:ckau@uab.edu
Robertson MA, Kau CH, English JD, Lee RP, Powers J, Nguyen JT. MI Paste Plus to prevent demineralization in orthodontic patients: A prospective randomized controlled trial. Am J Orthod Dentofacial Orthop 2011; 140: 660–668.
Rights and permissions
About this article
Cite this article
Rollings, S., Greene, L., Borrie, F. et al. Small trial finds beneficial effect for MI Paste in preventing white spot lesions during orthodontic treatment. Evid Based Dent 13, 117–118 (2012). https://doi.org/10.1038/sj.ebd.6400899
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ebd.6400899
