
Abstract
Study design:
A 2 × 2 cross-over design.
Objectives:
To compare immediate effects of obstacle crossing training and conventional overground walking training on functional ability among independent ambulatory patients with spinal cord injury (SCI).
Setting:
A tertiary rehabilitation center, Thailand.
Methods:
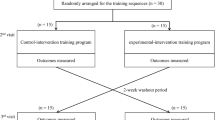
Twenty independent ambulatory participants with SCI received a 1-day overground walking training and a 1-day obstacle crossing training program in a randomized cross-over design with a 2-day washout period. Immediately prior and after each training program, the functional ability of all participants was measured using the timed up and go test (TUGT), five times sit-to-stand test (FTSST) and 10-m walk test (10MWT).
Results:
The TUGT, FTSST and 10MWT data were significantly better after obstacle crossing training (P<0.001) but not after the overground walking training (P>0.05). The improvement following obstacle crossing training was also significantly different from that of the overground walking training (P<0.05).
Conclusion:
Obstacle crossing training immediately enhanced functional ability related to walking of ambulatory participants with SCI. However, a further longitudinal study using a randomized controlled trial is needed to support benefits of incorporation of obstacle crossing training into rehabilitation practice.
Similar content being viewed by others


Introduction
Independent walking is an optimal goal that patients with spinal cord injury (SCI) want to achieve.1, 2 Although the patients can improve walking ability after participation in a rehabilitation program, the majority of them do not recover functional walking.3, 4 The ability of their walking is likely to be limited to within the house, over a short distance or with the support of a walking device.4 This may significantly relate to the impairments following SCI and effectiveness of rehabilitative strategies.
Currently, the methods of gait rehabilitation are likely to take place in an empty room in order to increase the confidence of patients while they practice walking.5 Such training conditions are different from those that the patients have to encounter at home and in the community, and may significantly impact on the applicability of the treatment outcomes. In an everyday environment, obstacle crossing such as over uneven paths, electric cords and branches is one of many complex tasks associated with ambulation.2, 6 To successfully accomplish obstacle crossing by both limbs and walking devices, patients have to modify their movement kinetics, kinematics and spatiotemporal parameters to conform with the sizes of obstacles on the floor, that is, lengthen a step length (for a wide obstacle) or use a flexor strategy to increase foot clearance (for a high obstacle) on a smaller base of support during a single support phase. Therefore, the task poses greater demands on the balance control, lower extremity motor strength and walking ability than unobstructed walking.6, 7, 8, 9 Currently, there is rare evidence on the incorporation of obstacle crossing training into rehabilitation practice for patients with SCI. Musselman et al.10 reported the benefit of an intensive and variable skill walking training program (including obstacle crossing) to improve walking ability in four participants with SCI. However, the program comprised many walking tasks, not only obstacle crossing training exclusively. Therefore, the findings may not truly indicate effects of obstacle training on walking ability of the patients. Based on the challenges occurring during obstacle crossing, the researchers hypothesized that the incorporation of obstacles into the process of walking training might enhance rehabilitation outcomes. Therefore, this study compared immediate effects of obstacle crossing training and conventional overground walking training on functional ability related to walking among independent ambulatory patients with SCI. The findings may provide important clues for modifying rehabilitation strategies for these patients.
Participants and methods
Participants, study design and setting
The study was a 2 × 2 cross-over design in which participants were given a sequence of interventions (cross-over from one intervention to another intervention during the course of study), which allows individual participants to serve as their own control to reduce effects of participants’ variation and the number of sample size required for the investigation.11 Based on the data from a pilot study in 12 independent ambulatory participants with SCI, the research required 20 participants and a 2-day washout period showed no significant carryover effects because of sequences of training (Table 1).
Participants were recruited from a tertiary rehabilitation center in Thailand. The inclusion criteria were age of at least 18 years, ability of walking independently with or without walking devices for at least 50 m (functional independent measurement locomotor (FIM-L) scores 6–7),12 and ability to rise from a chair independently with or without the use of hands. Participants were excluded if they had an SCI from a progressive disease, and presented any signs and symptoms that might affect participation in the study such as pain in the musculoskeletal system (at rest and with movement) with an intensity of pain of >5 out of 10 on a visual analog scale,13 deformity of the spine and lower extremities, and other neurological or medical disorders that could have negative impacts on ambulatory ability. Participants needed to sign a written informed consent document approved by the local ethics committee before participation in the study.
Apparatus
The setting required a 10-m walkway and four wooden obstacles (each of them had 60 cm long × 0.8 cm thick) of four sizes, including 4 cm high, 8 cm high, 4 cm wide and 8 cm wide (Figure 1a) in order to represent obstacles likely to be found in homes and communities.8

Obstacle crossing training. (a) Four wooden obstacles (60 cm long × 0.8 cm thick) with the width of 4 and 8 cm, and the height of 4 and 8 cm. (b) Training setting. (c) Obstacle crossing training (lead limb crossing). (d) Obstacle crossing training (trail limb crossing). A full color version of this figure is available at the Spinal Cord journal online.
Experimental procedure
Each participant was involved in the study for 5 days. On the first day, participants were assessed for their baseline demographics and neurological deficits, that is, motor and sensory scores, levels of injury and severity of SCI using the criteria from the American Spinal Injury Association (ASIA) Impairment Scale (AIS).14 Then, on the second day, participants were randomly allocated to participate in an obstacle crossing training program (A) or overground walking training program (B) using stages of SCI (subacute (post-injury time or PIT <12 months) and chronic (PIT ⩾12 months) stages),15 level of injury (tetraplegia or paraplegia) and FIM-L scores (FIM-L 6 or 7) as criteria for the training arrangement. After 2 days washout period, participants were trained using the other program. Therefore, 10 participants were trained using AB sequence and the other 10 participants were trained using the BA sequence. Each training program lasted 30 min (excluding rest periods). Details of the training programs are as follows:
Overground walking training
Participants were instructed to walk at a self-determined walking speed along a 10-m walkway with or without a walking device continuously as good and as long as they could.
Obstacle crossing training
The four obstacles were randomly placed on the floor at 2-m intervals (Figure 1b). The wide obstacles were placed flat on the floor and the high obstacles were attached vertically to the floor with a small amount of adhesive gum. Thus, if any obstacle was contacted by a foot or walking device, it fell flat on the floor to minimize the risk of tripping or injury to the participants. During training, participants were instructed to walk continuously over every obstacle at their self-determined walking speed with or without a walking device (Figures 1c and d), and not to attempt any obstacle that might pose a risk of injury for them.
The total training time lasted about 1 h. During training, participants did not wear shoes but needed to wear a lightweight safety belt around the waist with a therapist walking or being aside the participant to ensure safety. They were able to take a period of rest as required or with the modified Borg Scale more than 5 (range 0–10; 0: no dyspnea; 10: worst possible dyspnea).16 During taking part in the study, participants still received routine treatments from other rehabilitation professionals as needed.
Functional mobility tests
Immediately before and after each training program, participants were assessed for their functional ability using the timed up and go test (TUGT), five times sit-to-stand test (FTSST) and 10-m walk test (10MWT) in a random order using the Latin square. Details of the tests are as follows:
Timed up and go test: Participants sat on a standard armchair with their back against the backrest of the chair and their arms on the armrests of the chair or the walking device. They were instructed to stand up from the chair, walk at a fast and safe speed for 3 m, turn around a traffic cone, walk back and sit down on the chair with or without a walking device. Then the average time required for the three trials was recorded.17, 18
Five times sit-to-stand test: Participants sat on an armless chair with their back upright at 90° against the backrest of the chair, placing their feet flat on the floor with the heels about 10 cm behind the knees, while their arms were at their sides or on the walking devices. The test measured the time taken to complete five repetitions of the sit-to-stand maneuver. The average time for the three trials was used for data analysis.18, 19
10-m walk test: Participants were instructed to walk at a self-selected speed along a 10-m walkway with or without a walking device. To minimize acceleration and deceleration effects, the time required over the middle 4 m of the walkway was recorded.18, 20 The average time required for the three trials was converted to walking speed.
Statistical analyses
The descriptive statistics were applied to explain baseline demographics and findings of the study. The carryover (or residual) effects of the first intervention that might persist and distort the second intervention were assessed using the method proposed by Grizzle.21 The method proceeds in two steps, the first involving the intra-participant sums (S) of the training sequences in which SAB=X1,AB+X2,AB and SBA=X1,BA+X2,BA (where Xi,AB denotes the post-test outcomes of the measurement made in period i (1 or 2) on the participants who received the interventions in the order AB, and Xi,BA denotes the same for participants who received interventions in the order BA). Then the null hypothesis that γA=γB (where γA denotes carryover effects of intervention A and γB denotes the same for intervention B) was tested by comparing the mean sums  using the independent samples t-test. Grizzle21 recommended that the test should be performed at a significant level greater than the traditional value of 0.05, such as 0.10 or 0.15, and the study used a level of significance for carryover effects at P<0.10. If it is significant, only data for period 1 are used for data analyses. However, if it is not significant, the data of both periods are applied for analyses.11, 22 Then the differences between pre- and post-training in each intervention were compared using the Wilcoxon signed-rank test. Subsequently, the changes of both interventions were compared using the Mann–Whitney U-test. A P-value<0.05 was considered as a level of statistical significance for the training outcomes.
using the independent samples t-test. Grizzle21 recommended that the test should be performed at a significant level greater than the traditional value of 0.05, such as 0.10 or 0.15, and the study used a level of significance for carryover effects at P<0.10. If it is significant, only data for period 1 are used for data analyses. However, if it is not significant, the data of both periods are applied for analyses.11, 22 Then the differences between pre- and post-training in each intervention were compared using the Wilcoxon signed-rank test. Subsequently, the changes of both interventions were compared using the Mann–Whitney U-test. A P-value<0.05 was considered as a level of statistical significance for the training outcomes.
Results
Table 2 presents baseline demographics for 20 participants (15 men and 5 women) who completed the study (average age=40.9±16.5 years). All of them had mild severe SCI (AIS D) in which 5 participants were at a subacute stage of injury (average PIT=5±2.7 months) and 15 participants were at a chronic stage of SCI (average PIT=53.4±42.2 months).
As there were no significant carryover effects because of sequences of training (P>0.10, Table 1), the study reported data of all participants for each variable. Table 3 demonstrates the findings for the functional tests using the TUGT, FTSST and 10MWT. The results showed that, after obstacle crossing training, participants showed significant improvement in all variables (P<0.001). However, the post-training data for overground walking training showed significant difference from the pre-training data only for the FTSST (Table 3). Moreover, the changed data following obstacle crossing training were significantly different from those for overground walking training (P<0.01 for the TUGT and FTSST, and P<0.001 for the 10MWT, Table 3). In addition, the data were analyzed according to stages of injury in order to ensure effects of the training methods (Tables 4 and 5). The findings demonstrated that obstacle crossing training facilitated the significant improvement of functional ability of the participants, particularly at a chronic stage of injury (P⩽0.001, Table 4).
Discussion
The study investigated immediate effects of obstacle crossing training as compared with the conventional overground walking training on functional ability among independent ambulatory patients with SCI using a cross-over design. The findings suggested that, after obstacle crossing training, participants showed significant improvement of functional ability as measured using the TUGT, FTSST and 10MWT. The improvement was also significantly different from that for overground walking training (Table 3). Moreover, the improvement was clearly demonstrated in participants at a chronic stage of SCI (Table 4).
The TUGT, FTSST and 10MWT have been verified for their validity and reliability to assess functional ability of participants with SCI who walked with and without a walking device.18, 23 The TUGT is a timed walking test that is designed to measure mobility and balance control.24 The FTSST has been used to quantify balance control, risk of fall, levels of disability and lower extremity motor strength.19, 25 The 10MWT measures walking capacity that the results relate to overall quality of walking in patients with SCI.18, 26 Thus, the findings suggested that obstacle crossing training significantly improved functional ability relating to walking of the participants, and the improvement was significantly greater than that of overground walking training (Table 3).
The significant improvement following obstacle crossing training may relate to the task demands. Walking over an obstacle required participants to precisely swing the foot while maintaining body balance through coordinated joint movements of the stance limb.27 Thus, the task poses high demands on balance control and the ability to modify movement kinetics, kinematics and spatiotemporal parameters to conform with the size of obstacles on the floor.7, 8, 9, 27 Then repetitive practice of the obstacle crossing task facilitated the improvement of functional ability as measured using the TUGT, FTSST and 10MWT. Importantly, the improvement was clearly seen in participants with chronic SCI. At a chronic stage, the movement systems become less plastic and are limited in the patterns that are difficult to make any changes.15, 28 Therefore, the findings suggest beneficial effects of the incorporation of obstacle crossing into rehabilitation strategies in order to improve functional ability relating to walking of patients with SCI.
Nonetheless, there are some noteworthy limitations of the findings. The training effects were immediately measured; thus the findings might not truly indicate the learning effects. Moreover, every participant had mild severe SCI (AIS D) and there were only five participants at a subacute stage of SCI. Therefore, a further study in participants with different severity of SCI (AIS C and D) using a longitudinal randomized controlled trial with the assessments in a retention period is needed to strengthen the findings.
Data archiving
There were no data to deposit.
References
van der Salm A, Nene AV, Maxwell DJ, Veltink PH, Hermens HJ, IJzerman MJ . Gait impairments in a group of patients with incomplete spinal cord injury and their relevance regarding therapeutic approaches using functional electrical stimulation. Artif Organs 2005; 29: 8–14.
Amatachaya S, Thaweewannakij T, Adirek-udomrat J, Siritaratiwat W . Factors related to obstacle crossing in independent ambulatory patients with spinal cord injury. J Spinal Cord Med 2010; 33: 144–149.
Behrman A, Harkema S . Locomotor training after human spinal cord injury: a series of case studies. Phys Ther 2000; 80: 688–700.
Brotherton SS, Krause JS, Nietert PJ . Falls in individuals with incomplete spinal cord injury. Spinal Cord 2007; 45: 37–40.
Amatachaya S, Kaewsutthi M . Gait rehabilitation for patients with incomplete spinal cord injury (iSCI): conventional and treadmill training. J Med Tech Phys Ther 2007; 19: 100–107.
Said CM, Goldie PA, Patla AE, Sparrow WA . Effect of stroke on step characteristics of obstacle crossing. Arch Phys Med Rehabil 2001; 82: 1712–1719.
Chou LS, Kaufman KR, Brey RH, Draganich LF . Motion of the whole body's center of mass when stepping over obstacles of different heights. Gait Posture 2001; 13: 17–26.
Said C, Goldie P, Patla A, Sparrow W, Martin K . Obstacle crossing in subjects with stroke. Arch Phys Med Rehabil 1999; 80: 1054–1059.
Huang SC, Lu TW, Chen HL, Wang TM, Chou LS . Age and height effects on the center of mass and center of pressure inclination angles during obstacle-crossing. Med Eng Phys 2008; 30: 968–975.
Musselman KE, Fouad K, Misiaszek JE, Yang JF . Training of walking skills overground and on the treadmill: case series on individuals with incomplete spinal cord injury. Phys Ther 2009; 89: 601–611.
Senn S . Cross-Over Trials in Clinical Research 2nd edn. John Wiley & Sons: Chichester. 2002.
Jackson AB, Carnel CT, Ditunno JF, Read MS, Boninger ML, Schmeler MR et al Outcome measures for gait and ambulation in the spinal cord injury population. J Spinal Cord Med 2008; 31: 487–499.
Victorian Quality Council Acute pain management toolkit. Victoria: rural and regional health and aged care services division, 2007.
Kirshblum SC, Waring W, Biering-Sorensen F, Burns SP, Johansen M, Schmidt-Read M et al Reference for the 2011 revision of the International Standards for Neurological Classification of Spinal Cord Injury. J Spinal Cord Med 2011; 34: 547–554.
Wirth B, van Hedel HJ, Kometer B, Dietz V, Curt A . Changes in activity after a complete spinal cord injury as measured by the Spinal Cord Independence Measure II (SCIM II). Neurorehabil Neural Repair 2008; 22: 145–153.
Prigent H, Roche N, Laffont I, Lejaille M, Falaize L, Barbot F et al Relation between corset use and lung function postural variation in spinal cord injury. Eur Respir J 2010; 35: 1126–1129.
Lam T, Noonan V, Eng J . A systematic review of functional ambulation outcome measures in spinal cord injury. Spinal Cord 2008; 46: 246–254.
Poncumhak P, Saengsuwan J, Kumruecha W, Amatachaya S . Reliability and validity of three functional tests in ambulatory patients with spinal cord injury. Spinal Cord 2013; 51: 214–217.
Whitney SL, Wrisley DM, Marchetti GF, Gee MA, Redfern MS, Furman JM . Clinical measurement of sit-to-stand performance in people with balance disorders: validity of data for the Five-Times-Sit-to-Stand Test. Phys Ther 2005; 85: 1034–1045.
Finch E, Brooks D, Stratford P, Mayo N . Physical Rehabilitation Outcome Measures: A Guide to Enhanced Clinical Decision Making. BC Decker: Hamilton. 2002.
Grizzle J . The two-period change-over design and its use in clinical trials. Biometrics 1965; 21: 467–481.
Fleiss JL . A critique of recent research on the two-treatment crossover design. Control Clin Trials 1989; 10: 237–243.
van Hedel HJ, Wirz M, Dietz V . Assessing walking ability in subjects with spinal cord injury: validity and reliability of 3 walking tests. Arch Phys Med Rehabil 2005; 86: 190–196.
Podsiadlo D, Richardson S . The timed ‘up & go’: a test of basic functional mobility for frail elderly persons. J Am Geriatr Soc 1991; 39: 142–148.
Mong Y, Teo TW, Ng SS . 5-Repetition sit-to-stand test in subjects with chronic stroke: reliability and validity. Arch Phys Med Rehabil 2010; 91: 407–413.
van Hedel HJ, Dietz V, Curt A . Assessment of walking speed and distance in subjects with an incomplete spinal cord injury. Neurorehabil Neural Repair 2007; 21: 295–301.
Lu TW, Yen HC, Chen HL, Hsu WC, Chen SC, Hong SW et al Symmetrical kinematic changes in highly functioning older patients post-stroke during obstacle-crossing. Gait Posture 2010; 31: 511–516.
Kamm K, Thelen E, Jensen JL . A dynamical systems approach to motor development. Phys Ther 1990; 70: 763–775.
Acknowledgements
The study was supported by funding from the Improvement of Physical Performance and Quality of Life (IPQ) research group, Faculty of Associated Medical Science and the Graduate School, Khon Kaen University, Khon Kaen, Thailand.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Pramodhyakul, W., Wattanapan, P., Siritaratiwat, W. et al. Immediate effects of obstacle crossing training in independent ambulatory patients with spinal cord injury. Spinal Cord 51, 379–383 (2013). https://doi.org/10.1038/sc.2012.178
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2012.178
