
Abstract
Patients with Lynch syndrome have a high risk of colorectal cancer (CRC). In this study, we estimated the age- and sex-specific cumulative risks of CRC in Han Chinese patients with Lynch syndrome caused by the pathogenic germline mutations in MLH1 or MSH2 in Taiwan. Based on 321 mutation carriers and 419 non-mutation carriers from 75 pedigrees collected in an Amsterdam criteria family registry in Taiwan, the age- and sex-specific cumulative risks of CRC in male carriers of mutation in MLH1 and MSH2 at the age of 70 years were 60.3% (95% confidence interval (CI) = 31.1%–89.9%) and 76.7% (95% CI = 37.2%–99.0%), respectively. For females, the cumulative risks of CRC at the age of 70 were estimated to be 30.6% (95% CI = 14.3%–57.7%) and 49.3% (95% CI = 21.9%–84.5%) in the carriers of MLH1 and MSH2 germline mutations, respectively. In conclusion, the cumulative risks of CRC at the age of 70 in the Han Chinese patients is higher in mutation carriers than non-mutation carriers and male mutation carriers have a higher cumulative risk of developing CRC than the female mutation carriers.
Similar content being viewed by others

Introduction
Mismatch repair (MMR) genes maintain genomic stability by repairing insertion-deletion and mismatch base-pair mutations that occur during DNA replication1. Germline mutations in one of the MMR genes, particularly MLH1, MSH2, MSH6, PSM2, and EPCAM, cause Lynch syndrome2. Patients with this syndrome are characterized by an early onset of malignancies with a predilection for the proximal colon3, 4. The median age at colorectal cancer (CRC) diagnosis is younger (< 45 years) in these patients than the general population. Moreover, these patients have a higher risk of CRC and other Lynch syndrome-related cancers than the general population5, 6.
The cumulative risk of CRC in patients with Lynch syndrome at the age of 70 years was estimated to be more than 70%7,8,9,10. In the Han Chinese population, Fu et al. estimated the cumulative risk of more than 80% of developing CRC at the age of 70 years7. However, studies from the Netherlands, Australia, and the United States have reported that the cumulative risks of CRC and other cancers were considerably lower than previously reported estimates after adjustment for ascertainment bias11,12,13. In the Netherlands, Quehenberger et al. reported a cumulative risk of 27% and 23% of CRC in male and female mutation carriers at the age of 70, respectively, after adjustment for ascertainment bias11. Quehenberger et al. also indicated that failure to account for ascertainment bias may result in the overestimation of cancer risk in patients with Lynch syndrome11. A population-based study in Australia reported CRC cumulative risks of 45% and 38% in male and female patients, respectively, at the age of 70 after correct adjustment for ascertainment bias12. Moreover, in the United States, the cumulative risk of CRC at the age of 70 in African American families with Lynch syndrome was estimated to be 30.3% and 25.8% in male and female patients, respectively13.
The cumulative risk of CRC has been widely estimated in the European population (Table S1). However, in the Han Chinese population, only one study estimated the age-specific cumulative risk of CRC7, but this study included only 42 Lynch syndrome families. The objective of the present study was to estimate the age- and sex-specific cumulative risks of CRC in the Han Chinese population in Taiwan by using a relatively large sample size of 75 Lynch syndrome families.
Results
According to mutation analysis of MLH1 and MSH2, the sample used in the current study consisted of 321 proven germline mutation carriers and 419 non-mutation carriers from 75 pedigrees collected in an Amsterdam criteria family registry in Taiwan (Table 1). The 321 mutation carriers included 75 probands and 246 family members and 419 non-mutation carriers were family members of the probands. The study sample consists of 363 males (49%) and 377 females (51%). Among the 321 mutation carriers, 216 (67.2%), 103 (32.1%) and 2 (0.7%) were carriers of germline mutations in MLH1, MSH2, and both MLH1 and MSH2, respectively. Of the 740 study subjects, 565 (76%) were Taiwanese, 145 (20%) were Hakkas, and 30 (4%) were Mainland Chinese or aborigines. Furthermore, 259 of the 740 study subjects (35%) engaged in regular physical activities. The pedigree-level information including the type of MMR gene mutated, proband’s age at CRC diagnosis, number of family members within a pedigree, number of mutation carriers in a pedigree, and number of CRC cases was summarized in Table S2.
During the follow-up period, 162 patients received a diagnosis of CRC. Of these patients, 156 (48.6%) were mutation carriers and 6 (1.4%) were non-mutation carriers (Table 1). The distribution of time to CRC diagnosis in carriers of mutations in MLH1 or MSH2 and non-mutation carriers, stratified by sex, were shown in Fig. 1. The sex-specific Kaplan–Meier survival curves and log-rank tests revealed a significantly earlier onset of CRC in male mutation carriers (P < 0.0001, Fig. 1A) and female mutation carriers (P < 0.0001, Fig. 1B) compared to their respective non-mutation counterparts.

Kaplan–Meier survival of patients with Lynch syndrome compared to non-mutation carriers. (A) Male patients with Lynch syndrome were associated with an early onset of CRC compared to male non-mutation carriers. (B) Female patients with Lynch syndrome were associated with an early onset of CRC compared to the female non-mutation carrier. The figure was produced using the survival package and ggsurvplot from the survminer package in R software (version 3.6.2, R Core Team 2019, https://www.r-project.org/).
Table 2 shows the sex-specific estimates of hazard ratios (HRs) and 95% confidence intervals (CI) for CRC risk in patients with Lynch syndrome compared to their non-mutation counterparts. The male carriers of MLH1 or MSH2, MLH1, and MSH2 germline mutations had a HR of 23.2 (95% CI = 9.2–58.2), 24.2 (95% CI = 9.8–60.1), and 38.2 (95% CI = 12.2–119.9) for CRC compared to male non-mutation carriers, respectively. Similarly, female carriers of MLH1 or MSH2, MLH1, and MSH2 germline mutations had a HR of 13.2 (95% CI = 5.9–29.6), 15.0 (95% CI = 6.4–35.4), and 27.9 (95% CI = 10.1–76.9) for CRC compared to female non-mutation carriers, respectively.
The age- and sex-specific cumulative risk of CRC is presented in Table 3. In the general adult population in Taiwan, the cumulative risks of CRC at the age of 70 years for males and females were 3.82% and 2.43%, respectively. The cumulative risks of CRC at the age of 70 years in male carriers of mutations in MLH1 or MSH2, MLH1, and MSH2 were 58.7% (95% CI = 29.6%–89.2%), 60.3% (95% CI = 31.1%–89.9%), and 76.7% (95% CI = 37.2%–99.0%), respectively. For females, the cumulative risks of CRC at the age of 70 were estimated to be 27.5% (95% CI = 13.4%–51.3%), 30.6% (95% CI = 14.3%–57.7%), and 49.3% (95% CI = 21.9%–84.5%) in the carriers of germline mutations in MLH1 or MSH2, MLH1 and MSH2, respectively.
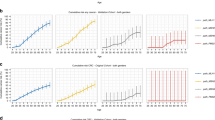
For both male and female, the cumulative risk of CRC at the age of 70 years in carriers of mutations in MSH2 appeared to be higher than that in carriers of mutations in MLH1 (Fig. 2A, B). Furthermore, the cumulative risk of CRC at the age of 70 years appeared to be higher in the male carriers of MLH1 mutation than female carriers of MLH1 mutation (Fig. 2C). A similar result was observed in carriers of MSH2 mutations (Fig. 2D).

Age- and sex-specific cumulative risk of colorectal cancer (CRC) at the age of 70 years in patients with Lynch syndrome (germline mutations in MLH1 or MSH2) in the Han Chinese population in Taiwan. (A) CRC risk in male patients with Lynch syndrome compared with the male general population. (B) CRC risk in female patients with Lynch syndrome compared with the female general population. (C) Comparison of CRC risk between male and female patients with MLH1 mutations. (D) Comparison of CRC risk between male and female patients with MSH2 mutations. The figure was produced using R software (version 3.6.2, R Core Team 2019, https://www.r-project.org/).
Discussion
The cumulative risk of CRC in patients with Lynch syndrome has been widely investigated in individuals of European ancestry. In this analysis, we estimated the cumulative risk of CRC in the Han Chinese patients with Lynch syndrome caused by pathogenic germline mutations in MLH1 or MSH2 in Taiwan. The cumulative risk of CRC at the age of 70 was much higher in mutation carriers than non-mutation carriers. Additionally, we found male mutation carriers to have a higher cumulative risk of CRC than female mutation carriers and carriers of MSH2 mutations have a higher cumulative risk of CRC than carriers of MLH1 mutations. By properly adjusted for ascertainment bias our estimates are in line with previous studies that also adjusted for ascertainment bias and reported a cumulative risk ranging from 25%–50% for female11, 12, 14,15,16 and 50%–80% for male patients12, 15,16,17 at the age of 70.
Previous studies have reported that the carriers of the MSH2 germline mutation had a higher CRC risk than did the carriers of the MLH1 mutation18, 19, which is consistent with our findings. In the present study, the cumulative risk of CRC at 70 years was considerably higher in the MSH2 mutation carriers than in the MLH1 mutation carriers. The biological mechanism underlying the higher CRC risk in the MSH2 mutation carriers may be due to the functional role of MSH2, which is to proofread a newly synthesized DNA strand for mismatch base-pair and insertion-deletion mutations that occur during DNA replication20. The MSH2 is the main protein involved in proofreading newly synthesized DNA strands21. Loss of function in MSH2 adversely affects the MMR system and hinders its recognition and repair of insertion-deletion and mismatch base-pair mutations. This results in the accumulation of mutations in newly synthesized DNA strands, which may eventually cause CRC if left uncorrected by other DNA repair genes. Moreover, our previous study indicated an earlier onset of CRC in patients with the MSH2 mutation than in patients with the MLH1 mutation22, which was consistent with our finding that the cumulative risk of CRC at the age of 70 in the patients with the MSH2 germline mutation was higher than that in those with the MLH1 mutation in the Han Chinese population in Taiwan.
We observed higher cumulative risks of CRC in male mutation carriers than in female mutation carriers. Our findings are consistent with those of other studies, which have also reported high cumulative risks of CRC at the age of 70 in male patients with Lynch syndrome15, 23, 24. A cohort study in Finland reported cumulative risks of 69% and 52% among male and female patients with Lynch syndrome at the age of 70, respectively23. Choi et al. reported a 67% cumulative risk of CRC in male patients with Lynch syndrome compared to 35% in female patients at the age of 7015. Moreover, Barrow et al. reported cumulative CRC risks of 58% and 49% among male and female patients with Lynch syndrome, respectively24. These findings indicated that male mutation carriers develop CRC earlier in life than female mutation carriers. The high cumulative risks of CRC in male patients may be due to hormonal differences between men and women. Besides, male sex is associated with relatively poor health-seeking behaviour25, which may affect the frequency of their colonoscopy screening.
The main strengths of the present study are that all the patients with Lynch syndrome were precisely confirmed by a comprehensive mutation detection strategy and cancer diagnoses were confirmed histologically. Moreover, to date, this study is the largest cohort study of patients with Lynch syndrome in the Han Chinese population. The main limitation of this study is the limited sample size, especially among non-mutation carriers and residual correlation of environmental and lifestyle factors among family members. Nevertheless, in the calculation the HR to estimate the CRC risk in patients with Lynch syndrome, we had adjusted for ethnicity and physical activity which were significantly associated with CRC risk in MLH1 and MSH2 germline mutation carriers in our previous study22. However, we could not rule out the genetic effects outside of MLH1 and MSH2 genes. Another limitation is the failure to test for other MMR genes, such as MSH6, PMS2, and EPCAM. Nevertheless, these genes contribute 10%–20% of the germline mutations in patients with Lynch syndrome26, 27.
In conclusion, we found that the male carriers have a higher cumulative risk of CRC than the female carriers and carriers of mutations in MSH2 have a higher cumulative risk of CRC than carriers of mutations in MLH1. Since the cumulative risk of CRC in the patients with Lynch syndrome is much higher than that in the general population, the patients with Lynch syndrome should continue to undergo intensive cancer screening surveillance by using less invasive and less expensive screening tools. Our estimates have implications in genetic counselling, designing and providing strategies for intensive CRC screening in patients with Lynch syndrome in Taiwan.
Methods
Study sample
The study sample was taken from the Amsterdam criteria (AC) family registry established by the Taiwan Hereditary Nonpolyposis Colorectal Cancer Consortium of the National Health Research Institutes in May 2002. As of February 2012, the AC family registry collected 135 pedigrees comprising 1,014 subjects from seven hospitals and medical centres located across Taiwan. In each pedigree, a single index patient (proband), which is a CRC patient with family history satisfying AC II28, was first recruited into the AC family registry. Then the recruitment was extended to family members of the proband. All probands provided tumor and normal tissues and peripheral blood cells were collected from all participants.
In the current study, the search of germline pathogenic mutations in MLH1 or MSH2 was first applied to all probands of these 135 pedigrees. For a pedigree in which the proband was found to carry pathogenic mutations in MLH1 or MSH2, all the other members in this pedigree were subsequently tested for the same pathogenic mutations carried by the proband. In such a pedigree, the proband and the family members who tested positive for the pathogenic mutations were classified as mutation carriers and the family members who tested negative for the pathogenic mutations were classified as non-mutation carriers. For a pedigree in which the proband did not carry any pathogenic mutation in MLH1 and MSH2, on the other hand, all members in this pedigree were excluded from this study. Finally, our analysis included 321 germline mutations carriers in MLH1 or MSH2 and 419 non-mutation carriers from 75 pedigrees.
Written informed consent was obtained from all study participants. The study was conducted following the 1975 Declaration of Helsinki, and all research protocols were approved by the Taiwan National Health Research Institute and Taipei Medical University Institutional Review Boards.
Search for germline mutation in MLH1 and MSH2
The search of germline mutations in MLH1 or MSH2 was first applied to all probands meeting the AC II. Genomic DNA obtained from blood leukocytes were used to perform the mutation analysis. Point mutations or small deletions/insertions in the exons were examined through denaturing high-performance liquid chromatography (DHPLC) analysis (WAVE DNA Fragment Analysis System, Omaha, NE, USA), followed by confirmatory DNA sequencing. For patients who had no point mutations or small insertions/deletions detected by DHPLC, large genomic deletions of MLH1 and MSH2 genes were examined using the multiplex ligation-dependent probe amplification (MLPA) analysis by SALSA MLPA kit P003 (MRC-Holland, Amsterdam, Netherlands). For patients who carried missense mutations without known deleterious effects on MLH1 or MSH2 proteins, further immunohistochemical (IHC) analysis, microsatellite instability (MSI) analysis, and cosegregation analysis were performed. For a pedigree in which the proband was found to carry pathogenic germline mutations in MLH1 or MSH2, all the other members in this pedigree were subsequently screened for the same pathogenic mutations carried by the proband. In this analysis, we define Lynch syndrome as an individual satisfying the ACII criteria who upon mutational testing is found to be a carrier of the MLH1 or MSH2 mutation The details of the procedures for genetic analyses have been previously described elsewhere29.
Data collection
Nurses from participating hospitals and medical centres across Taiwan were trained to conduct interviews. Interviews were administered uniformly to all patients after obtaining informed consent. Standardized interviews were conducted using structured questionnaires covering sociodemographic variables (age, sex, education, ethnicity, and occupation), lifestyle factors (cigarette smoking, alcohol consumption, and regular physical activity), medical information (cancer diagnosis and age at diagnosis, histological tumor type), and family histories of cancer. All patients were biennially followed from May 2002 to February 2012 to obtain updates about their morbidity and cancer diagnosis statuses. Histopathology reports, medical reports, cancer registry report, and death certificates were used to confirm cancer diagnoses and age at cancer diagnosis.
Statistical analysis
Every categorical characteristic of the study sample was described by showing the count and proportion of each category. The time at risk was considered to begin at birth and end at the first diagnosis of CRC, death, loss to follow-up, or end of February 2012, whichever occurred first. Subjects who did not receive a diagnosis of CRC were censored. For any subset of the study sample, the Kaplan–Meier survival curve was used to show the distribution of time to CRC diagnosis and the log-rank test was used to examine the difference in distributions between different subsets.
In our analysis, based on the data of MLH1/MSH2 mutation carriers and non-mutation carriers identified in the study sample, the Cox’s proportional hazards model was implemented to estimate sex- and mutation-specific hazard ratios (HR) for CRC risk, that is, the CRC incidence rates for sex- and mutation-specific carriers divided by that for sex-specific non-mutation carriers. The Cox’s proportional hazards model was fitted by maximum likelihood method through applying analysis option of penetrance estimation in Mendel 16.0, a comprehensive statistical package oriented to pedigrees in genetic studies30. Since the study sample was ascertained using a family history-based criterion and information of proband’s genotype, the potential bias for risk estimation due to ascertainment was corrected by implementing a retrospective likelihood approach, in which each family’s likelihood was conditioned on the phenotypes of all family members and the proband’s genotype. Data augmentation was used to implement the correction of ascertainment bias31, 32. Furthermore, the estimations of HRs were adjusted for ethnicity and physical activity which were significantly associated with CRC risk in MLH1 and MSH2 germline mutation carriers in our previous study22. When fitting the Cox’s proportional hazards model, Mendel provides estimates of the effect on CRC incidence rates due to pathogenic mutations and the corresponding standard error, denoted by \(\beta\) and \(s\), respectively. Then, compared with non-carriers, the HR for CRC risk in carriers, \(\theta\), was calculated by \({e}^{\beta }\) and the 95% confidence interval (CI) of HR, \(\left({\theta }_{L},{\theta }_{U}\right)\), was calculated by \({\theta }_{L}={e}^{\beta -1.96s}\) and \({\theta }_{U}={e}^{\beta +1.96s}\).
In this study, the risk of CRC in the non-mutation carriers was assumed to resemble that of the general adult Taiwanese population33. The age- and sex-specific CRC incidence rates in the Taiwanese general population were obtained from the Taiwan Ministry of Health and Welfare34. Then the cumulative CRC risk to age t years for sex- and mutation-specific carriers was calculated using the formula:
where \({\lambda }_{0}(\tau )\) denotes the sex-specific CRC incidence rate at age \(\tau\) years in the Taiwanese general population and \(\theta\) denotes the sex- and mutation-specific HR for CRC described above. Furthermore, the corresponding 95%CI of cumulative risk was calculated by \(\left(1-{\mathrm{exp}}\left(-\underset{0}{\overset{t}{\int }}{\theta }_{L}{\lambda }_{0} \left(\tau \right)d\tau \right), 1-{\mathrm{exp}}\left(-\underset{0}{\overset{t}{\int }}{\theta }_{U}{\lambda }_{0} \left(\tau \right)d\tau \right)\right)\) with \({\theta }_{L}\) and \({\theta }_{U}\) described above.
The Kaplan–Meier survival and age- and sex-specific cumulative risks of CRC were plotted using the open-source statistical programming language R (version 3.6.2, R Core Team 201935 in R Studio, version 1.1.383, R Studio Team36). Other statistical analyses were performed using SAS Version 9.4 for Windows (SAS Institute, Inc., Cary, NC, USA). A p-value of < 0.05 was considered to be statistically significant.
Ethics approval
Ethical regulations were followed, and the study was approved by the Taiwan National Health Research Institute and Taipei Medical University.
Data availability
All relevant data including the supplementary material are included in this manuscript.
References
Li, G.-M. Mechanisms and functions of DNA mismatch repair. Cell Res. 18, 85–98 (2008).
Jasperson, K. W., Tuohy, T. M., Neklason, D. W. & Burt, R. W. Hereditary and familial colon cancer. Gastroenterology 138, 2044–2058 (2010).
Boland, C. R. Evaluation and management of Lynch syndrome. Clin. Adv. Hematol. Oncol. 5, 851–873 (2007).
Jang, E. & Chung, D. C. Hereditary colon cancer: Lynch syndrome. Gut Liver 4, 151–160 (2010).
Lynch, H. T. & de la Chapelle, A. Hereditary colorectal cancer. N. Engl. J. Med. 348, 919–932 (2003).
Watson, P. et al. The risk of extra-colonic, extra-endometrial cancer in the Lynch syndrome. Int. J. Cancer 123, 444–449 (2008).
Fu, L. et al. Mismatch repair gene mutation analysis and colonoscopy surveillance in Chinese Lynch syndrome families. Cell Oncol. (Dordr) 36, 225–231 (2013).
Lin, K. M. et al. Cumulative incidence of colorectal and extracolonic cancers in MLH1 and MSH2 mutation carriers of hereditary nonpolyposis colorectal cancer. J. Gastrointest. Surg. 2, 67–71 (1998).
Ramsoekh, D. et al. Cancer risk in MLH1, MSH2 and MSH6 mutation carriers; different risk profiles may influence clinical management. Hered Cancer Clin. Pract. 7, 17 (2009).
Yamaguchi, T. et al. Comparison of clinical features between suspected familial colorectal cancer type X and Lynch syndrome in Japanese patients with colorectal cancer: A cross-sectional study conducted by the Japanese Society for Cancer of the Colon and Rectum. Jpn. J. Clin. Oncol. 45, 153–159 (2015).
Quehenberger, F., Vasen, H. F. A. & van Houwelingen, H. C. Risk of colorectal and endometrial cancer for carriers of mutations of the hMLH1 and hMSH2 gene: Correction for ascertainment. J. Med. Genet. 42, 491–496 (2005).
Jenkins, M. A. et al. Cancer risks for mismatch repair gene mutation carriers: A population-based early onset case-family study. Clin. Gastroenterol. Hepatol. 4, 489–498 (2006).
Guindalini, R. S. C. et al. Mutation spectrum and risk of colorectal cancer in African American families with Lynch syndrome. Gastroenterology 149, 1446–1453 (2015).
Dowty, J. G. et al. Cancer risks for MLH1 and MSH2 mutation carriers. Hum. Mutat. 34, 490–497 (2013).
Choi, Y.-H. et al. Penetrance of colorectal cancer among MLH1/MSH2 carriers participating in the colorectal cancer familial registry in Ontario. Hered. Cancer Clin. Pract 7, 14 (2009).
Stoffel, E. et al. Calculation of risk of colorectal and endometrial cancer among patients with Lynch syndrome. Gastroenterology 137, 1621–1627 (2009).
Borràs, E. et al. MLH1 founder mutations with moderate penetrance in Spanish Lynch syndrome families. Cancer Res. 70, 7379–7391 (2010).
Goecke, T. et al. Genotype-phenotype comparison of German MLH1 and MSH2 mutation carriers clinically affected with Lynch syndrome: A report by the German HNPCC Consortium. J. Clin. Oncol. 24, 4285–4292 (2006).
Kastrinos, F. et al. Phenotype comparison of MLH1 and MSH2 mutation carriers in a cohort of 1,914 individuals undergoing clinical genetic testing in the United States. Cancer Epidemiol. Biomarkers Prev. 17, 2044–2051 (2008).
Acharya, S. et al. hMSH2 forms specific mispair-binding complexes with hMSH3 and hMSH6. Proc. Natl. Acad. Sci. U.S.A. 93, 13629–13634 (1996).
Chang, D., Ricciardiello, L., Goel, A., Chang, C. & Boland, C. Steady-state regulation of the human DNA mismatch repair system. J. Biol. Chem. 275, 29178 (2000).
Kamiza, A. B. et al. Risk factors associated with colorectal cancer in a subset of patients with mutations in MLH1 and MSH2 in Taiwan fulfilling the Amsterdam II criteria for Lynch syndrome. PLoS ONE 10, e0130018 (2015).
Hampel, H. et al. Cancer risk in hereditary nonpolyposis colorectal cancer syndrome: Later age of onset. Gastroenterology 129, 415–421 (2005).
Barrow, E. et al. Colorectal cancer in HNPCC: Cumulative lifetime incidence, survival and tumour distribution. A report of 121 families with proven mutations. Clin. Genet. 74, 233–242 (2008).
Galdas, P. M., Cheater, F. & Marshall, P. Men and health help-seeking behaviour: Literature review. J. Adv. Nurs. 49, 616–623 (2005).
von Salomé, J. et al. Genetic anticipation in Swedish Lynch syndrome families. PLoS Genet. 13, e1007012 (2017).
Cox, V. L. et al. Lynch syndrome: Genomics update and imaging review. Radiographics 38, 483–499 (2018).
Vasen, H. F., Watson, P., Mecklin, J. P. & Lynch, H. T. New clinical criteria for hereditary nonpolyposis colorectal cancer (HNPCC, Lynch syndrome) proposed by the International Collaborative group on HNPCC. Gastroenterology 116, 1453–1456 (1999).
Tang, R. et al. Colorectal cancer without high microsatellite instability and chromosomal instability—an alternative genetic pathway to human colorectal cancer. Carcinogenesis 25, 841–846 (2004).
Lange, K. et al. Mendel: The Swiss army knife of genetic analysis programs. Bioinformatics 29, 1568–1570 (2013).
Clayton, D. Conditional likelihood inference under complex ascertainment using data augmentation. Biometrika 90, 976–981 (2003).
Schaid, D. J., McDonnell, S. K., Riska, S. M., Carlson, E. E. & Thibodeau, S. N. Estimation of genotype relative risks from pedigree data by retrospective likelihoods. Genet. Epidemiol. 34, 287–298 (2010).
Lynch, H. T., Snyder, C. L., Shaw, T. G., Heinen, C. D. & Hitchins, M. P. Milestones of Lynch syndrome: 1895–2015. Nat. Rev. Cancer 15, 181–194 (2015).
National Health Service-Cancer Registration Online Interactive Inquiry System. https://cris.hpa.gov.tw/.
R Core Team R: A language and environment for statistical computing.https://www.R-project.org/ (R Foundation for Statistical Computing, Vienna, 2019).
RStudio Team RStudio: Integrated Development for R. https://www.rstudio.com/ (RStudio, Inc., Boston, 2019).
Acknowledgements
The authors thank all patients and their family members for participating in this study, as well as the help from Mr. Le-Ting Lin and Mr. Wei-Pin Hsiao in statistical analysis.
Funding
This study was supported by the National Science Council, Executive Yuan, Taiwan (NSC 101-2314-B-038-057), the Ministry of Science and Technology, Taiwan (MOST 104-2314-B-038-009), and the Health and Welfare Surcharge of Tobacco Products (MOHW107-TDU-B-212-114020, MOHW108-TDU-B-212-124020 and MOHW109-TDU-B-212-134020).
Author information
Authors and Affiliations
Contributions
R.T., C.A.H., and C.C.Y. conceived and designed the experiments. W.C.W., J.F.Y., H.T.C., C.H.L., L.L.C., and T.P.L. performed the experiments. A.B.K., W.C.W., T.P.L., K.Y.H., C.A.H., and C.C.Y. analyzed the data. W.C.W., R.T., C.A.H., and C.C.Y. contributed reagents, materials, and analytical tools. A.B.K., C.A.H., and C.C.Y. drafted the manuscript. All authors directly participated in the planning, execution, and analysis of the study, and have read and approved the final submitted version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kamiza, A.B., Wang, WC., You, JF. et al. Cumulative risks of colorectal cancer in Han Chinese patients with Lynch syndrome in Taiwan. Sci Rep 11, 8899 (2021). https://doi.org/10.1038/s41598-021-88289-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-021-88289-2
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
