
Abstract
Study design
Retrospective chart review.
Objectives
The objective of this study was to characterize opioid administration in people with acute SCI and examine the association between opioid dose and (1) changes in motor/functional scores from hospital to rehabilitation discharge, and (2) pain, depression, and quality of life (QOL) scores 1-year post injury.
Setting
Spinal Cord Injury Model System (SCIMS) inpatient acute rehabilitation facility.
Methods
Patients included in the SCIMS from 2008 to 2011 were linked to the National Trauma Registry and the electronic medical record. Three opioid dose groups (low, medium, and high) were defined based on the total morphine equivalence in milligrams at 24 h. The associations between opioid dose groups and functional/motor outcomes were assessed, as well as 1-year follow-up pain and QOL surveys.
Results
In all, 85/180 patients had complete medication records. By 24 h, all patients had received opioids. Patients receiving higher amounts of opioids had higher pain scores 1 year later compared with medium- and low-dose groups (pain levels 5.5 vs. 4 vs. 1, respectively, p = 0.018). There was also an 8× greater risk of depression 1 year later in the high-dose group compared with the low-dose group (OR: 8.1, 95% CI: 1.2–53.7). In analyses of motor scores, we did not find a significant interaction between opioid dose and duration of injury.
Conclusions
These preliminary findings suggest that higher doses of opioids administered within 24 h of injury are associated with increased pain in the chronic phase of people with SCI.
Similar content being viewed by others

Introduction
It is estimated that there are nearly 800,000 new cases of traumatic SCI annually worldwide [1]. After the primary damage to the spinal cord, a phase of secondary damage begins with ischemia, excitotoxicity, and disruption of ionic homeostasis engaging multiple, complex cell death cascades. Ongoing research seeks to mitigate this secondary injury and improve functional outcomes by interrupting these cascades. Currently, there are at least 17 active clinical trials that are focused on the acute period of SCI to improve neurologic repair and/or mitigate secondary injury [2]. Surprisingly, as part of these investigations, the consequences of medications that are routinely applied in the emergency setting have been largely overlooked. Through animal studies, it has been postulated that opioids, administered as analgesics in the emergency setting, may enhance the excitotoxic state and glial cell activation in acute spinal cord injury [3]. Yet, there have been no studies examining whether these conventional interventions affect long-term recovery in the human population.
In animal models of acute SCI, opioid use leads to poor functional outcomes, attenuating locomotor recovery and worsening neuropathic pain [3,4,5,6,7,8]. Hook et al. have repeatedly shown that irrespective of the route of administration (intrathecal or intravenous (IV)), morphine administered in the acute phase of SCI significantly attenuates locomotor recovery, increases lesion size, and increases chronic pain symptoms in a rodent model. They showed that morphine increases inflammation and spinal pro-inflammatory cytokine expression [5, 9], which would not only increase cell death but would also instigate a cycle that exacerbates symptoms of pain [7,8,9], and perhaps depression and anxiety, as has been seen in the general population [7, 10,11,12,13]. This is concerning for people with SCI, as there is a three-times greater risk of depression and associated suicide compared with those without SCI [14, 15]. These data suggest that opioids may be contraindicated after SCI.
Nonetheless, opioids are among the most effective medications for the treatment of pain in the acute and subacute phases of injury. Although there have been no empirical reports on the emergency room use of opioids for the SCI population specifically, it has been reported that nearly 50% of trauma patients receive IV opioid analgesia within 3 h of emergency department (ED) arrival [16]. Effective pain management in the acute phase of spinal injury is essential, and under-medication during the acute management of trauma has been linked to development of chronic pain, as well as affective disorders and cognitive impairment [17,18,19]. Given the animal data, however, we need to know whether early opioid treatment is also detrimental in humans. Understanding the effects of opioids, and the molecular mechanisms mediating these effects, will have significant implications for the development of safe and effective strategies for the management of pain in the acute phase of SCI.
To address this gap in knowledge, the current study aimed to: (1) describe the pattern of opioid administration in acute SCI; (2) evaluate changes in motor function related to acute opioid administration; and (3) examine associations between acute opioid administration and pain, quality of life (QOL) and mobility measures at 1-year post injury. We hypothesized that: (1) opioid use would increase with increased injury severity scores (ISS), (2) there would be a negative interaction between opioid dose and functional recovery, and (3) QOL and mobility measures at 1 year would decrease as early opioid use increased.
Methods
Subjects
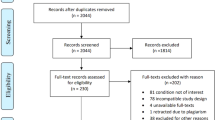
To test these hypotheses, we collected data on all traumatic SCI patients that were admitted to TIRR Memorial Hermann from 2008 to 2011 for inpatient rehabilitation (IR), and that had consented to participate in the Spinal Cord Injury Model Systems (SCIMS) database (Fig. 1). The SCIMS are institutions that are national leaders in medical research and patient care in SCI from the point of injury and beyond, supported through government-sponsored grants awarded every 5 years through a competitive application process. Criteria for SCIMS participation include: (1) minimum of 18 years old, (2) SCI was caused by external traumatic event, (3) temporary or permanent loss of sensory and/or motor function as a result of the event, and (4) a US citizen residing in the geographic catchment area at the time of injury. Excluded from SCIMS are patients that had: (1) previous treatment at Model System for the SCI or (2) completed previous rehabilitation admission for this SCI. The TIRR SCIMS data were linked to the Memorial Hermann National Trauma registry database and the electronic medical record (EMR). The time points of data collection are shown in Table 1.

SCIMS Spinal Cord Injury Model Systems, QOL quality of life.
Only patients admitted within 3 days of injury were included in the analyses to improve the chances of having complete medication records, including medications administered by emergency responders. Opioid types and quantities were collected and converted to milligrams of morphine equivalents (MEmg) using a conversion calculator [20].
Motor scores, pain and QOL outcomes
Motor scores from the International Standards for the Neurological Classification of SCI (ISNCSCI) were collected at three time points: (1) upon admission to the model system, (2) upon admission to acute IR, and (3) at discharge from IR. Total motor score (TMS) is scored out of 100 points, 50 points for five upper extremity joint movements bilaterally and the other half from five lower extremity joint movements bilaterally (LEMS) using the Medical Research Council scale for muscle strength.
Pain scores were also collected upon admission to the model system, and as part of the 1-year QOL survey. The first three pain scores were collected within 1 h of arriving in the emergency room, and entered into the EMR. These scores were averaged to derive baseline pain measures. The 1-year QOL survey outcomes are part of the SCIMS inventory. All pain scores collected were based on the Numerical Pain Rating Scale, 0 (no pain) to 10 (worst imaginable pain). Only those patients that answered the “Severity of Pain” question at 1 year were included in the analyses of QOL outcomes. In addition to the Severity of Pain question, other survey questions selected to correlate to opioid administration can be found in Table 2. Risk for depression was considered a sum of the Patient Health Questionnaire 2 (PHQ-2) scores of 3 or greater [21].
Statistical analyses
Description of opioids used in SCI within 24 h
Three opioid dose groups (low, medium, and high) were defined, by dividing the patient group into thirds based on the total MEmg at 24 h. Baseline demographics, clinical, or trauma characteristics were compared among opioid dose groups using ANOVA or Kruskal–Wallis rank test for continuous variables and Fisher’s exact test for categorical variables. A t-test was used to compare initial pain scores among SCI phenotypes (neurologic level and completeness/severity of SCI). Use of each type of opioid administered across three time points (within 4, 12, and 24 h of injury) were compared using multilevel mixed-effects logistic regression. Associations between opioid types administered and (1) representative SCI groups (paraplegia vs. tetraplegia, complete vs. incomplete injury) and (2) categories of opioid doses (low, medium, and high) were evaluated at each of the three time points using two-sided Fisher’s exact test. Generalized estimating equation modeling of the opioid types used adjusted for the opioid dose category (low, medium, and high), and administration times (within 4, 12, and 24 h) were performed. Finally, linear and logistic regression analyses were performed to evaluate the association of ISS and initial pain scores to the type of opioid administered. Due to controversy regarding the effects of opioids on blood pressure and low blood pressure in acute SCI from neurogenic shock, we considered whether hypotension in the ED influenced opioid administration [22].
Motor recovery association with acute opioid use
Multilevel mixed-effects linear regression models were used to evaluate the association between each longitudinal outcome, collected upon admission to the model system, upon admission to IR, and at discharge from IR (total-, UE-, and LE-motor, and Functional Independence Measure (FIM) scores) and duration of injury, log-transformed opioid dose (MEmg), and their interaction. The ISNCSCI is the source of the motor scores. We hypothesized that a significant negative interaction would exist with time and increased opioid dose, indicating that patients who received greater opioid doses would have reduced recovery. All models included patient random intercepts to account for within-patient correlation and were adjusted for potential confounders of age, sex, initial pain score, tetraplegia/paraplegia, complete injury, and days until surgery. Days until surgical decompression were included because of the literature suggesting that early decompression improves outcomes [22]. Subgroup analyses using similar models were performed in motor incomplete SCI due to the increased potential for motor recovery which might allow to detect an effect, if any, from opioid administration.
Pain and QOL at 1 year correlated to acute opioid use
Chi-squared tests and t-tests were used to evaluate differences between patients that answered the 1-year survey and those that did not answer. Those that answered the 1-year survey were organized based on their 24-h opioid dose classification. Their characteristics were compared with Kruskal–Wallis rank sum tests and Fisher’s exact tests. Linear and logistic regression analyses, or ordinal logistic models, were used to evaluate the association between outcomes of 1-year pain, depression, and QOL scores and the 24-h opioid dose category, adjusting for age, sex, and initial pain scores. Stata 14.0 (StataCorp, 2015) was used for the analyses, with p < 0.05 set for significance. The STROBE statement was followed in the reporting of these findings [23].
Results
Opioid categories and administration
There were 180 patients enrolled in the SCIMS database at Memorial Hermann from 2008 to 2011. Of these, 140 were admitted within 3 days of injury and 90 patients had complete medication records, including data from emergency response teams at the scene of the injury. Eighty-five patients had sufficient physical exam records to include in the analysis of opioid type use (Table 3).
All patients were given opioids within 24 h of injury. Of the 85 patients, 21 did not receive any opioid medications within the first 4 h post injury, only 6 had not been administered opioids at 12 h, and all had received some form of opioid treatment by 24 h. Patients were most commonly treated with morphine (82%), followed by fentanyl (52%), hydromorphone (33%), and oxycodone (6%). Twenty-nine percent of the patients were treated with a combination of opioids.
The 24-h dose categories had significantly different morphine equivalents administered: low dose with a median total of 6.3 MEmg (IQR: 4–10); medium dose median total 23.3 MEmg (IQR 18.3–26.67); high dose median total 60.1 MEmg (IQR: 43.2–140.8) (group difference p < 0.001) (Table 3). Differences in opioid totals in these categories were also seen at 4 and 12 h (group differences p < 0.001 for both 4 and 12 h). Initial numerical pain scores were also different between the three opioid dose categories [mean (SD)]: low, 4.6 (3.3); medium, 5 (3.2); and high, 6.5 (2.7); p = 0.048. Otherwise, there were no significant differences in baseline demographics, clinical, or trauma variables. Similarly, initial motor scores, SCI phenotypes, and severity of SCI [American Spinal Injury Association Impairment Scale] did not differ between groups. There was no difference between opioid dose categories and the etiology of the trauma.
There was no significant association between ED hypotension and the type of opioid used within any time interval. As ISS increased, however, the odds of receiving fentanyl increased by 8% [OR: 1.08, 95% CI: 1.01–1.15] at 12 h and 7% at 24 h [OR: 1.07, 95% CI: 1–1.13]. As initial pain score increased, the OR of receiving fentanyl was 1.23 (95% CI: 1.05–1.45) at 4 h, 1.24 (95% CI: 1.06–1.44) at 12 h, and 1.21 (95% CI: 1.04–1.4) at 24 h. Alternatively, the odds of morphine administration decreased by 22% at 24 h [OR: 0.78, 95% CI: 0.63–0.98] as initial pain scores increased.
There were several differences in opioid type administration based on patient SCI phenotypes. There was more fentanyl administration for patients with motor incomplete injuries (48%) compared with motor complete injuries (20%) at 4 h (p = 0.011) and 12 h (58% vs. 33%, respectively, p = 0.031). Oxycodone was also prescribed more to patients with motor incomplete (13%) compared with motor complete injuries (0%, p = 0.02). Conversely, morphine was administered more in patients with motor complete injuries (53%) compared with motor incomplete injuries (28%, p = 0.027). The administration of opioid types did not significantly differ based on dose groups.
Motor score association to opioid dose administration
Table 4 presents the results of the motor scores and FIM changes controlling for demographics, injury and SCI characteristics, and opioid medication variables, from the multivariable mixed-effects models. Controlling for the independent variables, TMS was reduced in patients with tetraplegia compared with paraplegia by 23.4 points (95% CI: −29.2, −17.6) over the three assessment times from the initial ISNCSCI exam to rehabilitation discharge [mean: 130 days (range: 15–734 days)]. Similarly, compared with patients with motor incomplete injury, motor complete injury had a reduced TMS by 28.5 (95% CI: −37, −20), and LEMS by 24.2 (95% CI: −29.3, −19.1) as duration of injury increased. FIM scores were also reduced in patients with tetraplegia compared with paraplegia by 17.2 (95% CI: −25.6, −8.9) and patients with motor complete compared with incomplete injury by 16.1 (95% CI: −28.5, −3.7). Subgroup analysis in patients with motor incomplete injuries indicated similar reductions in total and FIM motor score in tetraplegia. In this subgroup, as days until surgery increased, LEMS also decreased by 0.7 (95% CI: −1.5, 0). In all analyses of motor scores, the interaction of opioid doses (MEmg) with duration of injury was not statistically significant.
Opioid administration correlations to 1-year outcomes
Of the 85 patients included in the analyses, 46 responded to the pain question at the 1-year survey. There were no differences in demographics, ISS, FIM, and discharge motor scores between responders and nonresponders. Those that responded had a significantly greater 24-h opioid subtotal (30.6 MEmg, IQR: 10–68) compared with those that did not answer the pain question (18.8 MEmg, IQR: 7.6–25.7, p = 0.024), despite similar mean initial pain scores [5.4 (2.9) vs. 5.3 (3.4), respectively, p = 0.816]. Also, there were more survey responders in the high-dose group (44%) compared with those that did not answer (20%, dose category difference p = 0.019) and more patients with tetraplegia (36 vs. 15%, p = 0.019) and incomplete injury (44 vs. 17%, p = 0.026).
Among the survey responders, there was a significant dose group difference between opioid totals at 4, 12, and 24 h (Fig. 2a). Those in the high-dose category also had higher median pain scores at 1 year compared with medium- and low-dose groups (5.5 vs. 4 vs. 1, p = 0.018; Fig. 2b). However, initial mean pain scores were not significantly different between the three groups (Fig. 2b). There were no other differences across groups based on demographics, SCI phenotypes, and QOL measures.

a Opioid totals within 4, 12, and 24 h by 24-h opioid categories low-, medium-, and high-dose groups. Opioid dose categories significantly different at 4 h (*p = 0.008), 12, and 24 h (^p < 0.001 for both). b Line bars indicate mean initial pain (grey) and 1-year pain scores (black). Pain score at 1 year is significantly different between opioid dose categories (~p = 0.018). Initial pain scores are not significantly different between dose categories (p = 0.568).
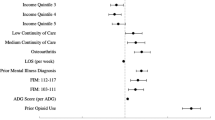
Table 5 presents independent variables (rows) and 1-year pain and QOL outcomes (columns) with beta coefficients (or OR) and 95% CI of the regression models. Focusing on the survey responders only, as initial pain score increased, pain interfering with work increased by 0.5 (95% CI: 0.2–0.8). Pain at 1 year also increased by 0.05 (95% CI: 0.003–0.9) as age increased. Alarmingly, compared with the low-dose group, the high-dose opioid group also had increased numerical pain scores at 1 year by 3.1 (95% CI: 1.4–4.8) adjusting for sex, age, and initial pain score. Self-perceived health score was also higher in the high-dose opioid group compared with the low-dose group (1.4, 95% CI: 0–2.7). The PHQ No. 1 score was increased in the high-dose opioid group compared with the low dose (1.8, 95% CI: 0.4–3.2) and increased with increasing age (0.04, 95% CI: 0–0.08). A positive screen for depression based on the PHQ-2 scores of ≥3 was associated with an 8× greater risk in the high-dose group compared with the low-dose group, adjusting for age, sex, and initial pain score (OR: 8.1, 95% CI: 1.2–53.7, Fig. 3).

*OR: 8.1, 95% CI: 1.2– 53.7.
Discussion
These data provide the first description of patients with acute SCI opioid administration and correlations to neurologic outcomes. Prior research reported that half of all patients with traumatic injuries received opioids within 3 h of ED arrival [16]. For patients with SCI, we report an increase in treatment, with nearly 70% receiving opioids within 4 h of injury, and every patient administered opioids within 24 h of injury.
Increased opioid doses were associated with increasing initial pain scores, although not in a linear relationship. For example, at 12 h, average initial pain scores of those in the low-dose group were 4.6 and they received about 4 MEmg. Those in the medium-dose group with a mean initial pain score of 5.0 (0.4 points higher) were administered about 4× more opioid (16 MEmg). The variation in opioid dosage was significant, with the low-dose group receiving nearly four and ten times less opioids than the medium- and high-dose categories, respectively. We also hypothesized that SCI characteristics would be associated with opioid dose administration, for example, patients with tetraplegia would have increased doses compared with paraplegia. However, there were no SCI differences across opioid dose groups. With similar patient demographics, ISS, and vital signs, it is unclear as to why such variation existed within the first 24 h.
Although opioid dose was not associated with decreased motor recovery, we did observe that patients in the high-dose opioid category had 3 point higher pain scores at 1 year compared with those in the low-dose group. This supports the animal evidence of increased chronic pain with acute opioid administration [4]. Moreover, the dose of opioids administered, and not initial pain scores, appeared to predict the development of chronic pain. Indeed, the initial pain scores of patients that answered the 1-year survey were similar across opioid dose groups. The only significant measured difference associated with increased pain scores at 1 year was the opioid dose administered in the first 24 h. This preliminary data suggest that, as in animal models, opioids may be modulating the molecular response to SCI, increasing inflammation, for example [9], and leading to adverse long-term consequences in the patient population.
In addition to pain, we also observed an 8× increased risk of depression at 1 year with higher doses of acutely administered opioids. Although the average PHQ scores appear similar across the opioid groups, the sum of three or higher is greater in the high-dose group, and regression modeling demonstrated an 8× higher risk of depression associated with the high doses of opioids compared with low doses. While scores from the PHQ-2 do not define depression, this tool has been validated as a depression screener after SCI [21]. Our data, therefore, suggest that the acute administration of high doses of opioids may further compound the increased risk of depression in patients after SCI.
There are several limitations in this observational study. Primarily, conclusions cannot be made given the small sample size with heterogenous injury characteristics, and the data provided from a single institution limits generalizability. While our analyses adjusted for measured potential confounders, the risk of residual confounding remains. Exclusion of patients that were not part of our healthcare system within 3 days of injury, as well as lacking information on those that did not consent to the SCIMS study, may have introduced selection bias. The evaluation of the pattern of opioid administration was also limited, lacking recordings of BP and pain scores immediately prior to administration of medication. Other trauma variables of interest were also incomplete in the EMR including vital signs at the scene of the injury, ISS, and GCS. For depression, although past medical history of depression prior to SCI was collected by interview, most patients responded that they did not know. It is possible that patients with undiagnosed depression may have been administered higher doses of opioids acutely and had higher pain scores at 1 year. Future studies should incorporate reliable and validated predictors of depression after trauma. Finally, an overall lack of response to the 1-year survey questions limits the ability to draw conclusions on pain, depression, and QOL measures.
Future studies may be able to address these issues by first carefully considering whether a randomized trial is warranted. If a trial is not feasible, a prospective cohort study with prespecified and limited data collection would mitigate some of the limitations of the current study. Directed acyclic graph could aid in visualizing the causal chain between opioid exposure and important clinical outcomes and help identify all of the potential confounders [24, 25]. These steps would help ensure that all needed data are properly collected and missing data is minimized. A detailed statistical analysis plan that includes appropriate methods for reducing confounding and sampling bias, handling missing data, and obtaining estimates of causal effects would further mitigate known problems with observational studies while providing needed evidence of benefit or harm from opioids.
Nonetheless, in this cohort of patients we found an association between the dosage of opioid administration within 24 h of SCI and increased 1-year pain scores, as well as an increased risk of depression, despite similar initial pain scores. Further investigation of these associations is warranted with a prospective, multicenter study.
Data availability
The datasets generated and/or analyzed during the current study are not publicly available due to large datasets without a comprehensive legend, but are available from the corresponding author on reasonable request.
References
Kumar R, Lim J, Mekary RA, Rattani A, Dewan MC, Sharif SY, et al. Traumatic spinal injury: global epidemiology and worldwide volume. World Neurosurg. 2018;113:e345–63.
Klingler HC, Pycha A, Schmidbauer J, Marberger M. Use of peripheral neuromodulation of the S3 region for treatment of detrusor overactivity: a urodynamic-based study. Urology. 2000;56:766–71.
Hook MA, Liu GT, Washburn SN, Ferguson AR, Bopp AC, Huie JR, et al. The impact of morphine after a spinal cord injury. Behav Brain Res. 2007;179:281–93.
Hook MA, Moreno G, Woller S, Puga D, Hoy K Jr., Balden R, et al. Intrathecal morphine attenuates recovery of function after a spinal cord injury. J Neurotrauma. 2009;26:741–52.
Hook MA, Washburn SN, Moreno G, Woller SA, Puga D, Lee KH, et al. An IL-1 receptor antagonist blocks a morphine-induced attenuation of locomotor recovery after spinal cord injury. Brain Behav Immun. 2011;25:349–59.
Woller SA, Moreno GL, Hart N, Wellman PJ, Grau JW, Hook MA. Analgesia or addiction?: implications for morphine use after spinal cord injury. J Neurotrauma. 2012;29:1650–62.
Woller SA, Malik JS, Aceves M, Hook MA. Morphine self-administration following spinal cord injury. J Neurotrauma. 2014;31:1570–83.
Hook MA, Woller SA, Bancroft E, Aceves M, Funk MK, Hartman J, et al. Neurobiological effects of morphine after spinal cord injury. J Neurotrauma. 2017;34:632–44.
Aceves M, Terminel MN, Okoreeh A, Aceves AR, Gong YM, Polanco A, et al. Morphine increases macrophages at the lesion site following spinal cord injury: protective effects of minocycline. Brain Behav Immun. 2019;79:125–38.
Scherrer JF, Salas J, Lustman PJ, Burge S, Schneider FD.Residency Research Network of Texas, et al. Change in opioid dose and change in depression in a longitudinal primary care patient cohort. Pain. 2015;156:348–55.
Scherrer JF, Svrakic DM, Freedland KE, Chrusciel T, Balasubramanian S, Bucholz KK, et al. Prescription opioid analgesics increase the risk of depression. J Gen Intern Med. 2014;29:491–9.
Ilgen MA, Bohnert AS, Ganoczy D, Bair MJ, McCarthy JF, Blow FC. Opioid dose and risk of suicide. Pain. 2016;157:1079–84.
Salas J, Scherrer JF, Schneider FD, Sullivan MD, Bucholz KK, Burroughs T, et al. New-onset depression following stable, slow, and rapid rate of prescription opioid dose escalation. Pain. 2017;158:306–12.
Hoffman JM, Bombardier CH, Graves DE, Kalpakjian CZ, Krause JS. A longitudinal study of depression from 1 to 5 years after spinal cord injury. Arch Phys Med Rehabil. 2011;92:411–8.
Cao Y, Massaro JF, Krause JS, Chen Y, Devivo MJ. Suicide mortality after spinal cord injury in the United States: injury cohorts analysis. Arch Phys Med Rehabil. 2014;95:230–5.
Neighbor ML, Honner S, Kohn MA. Factors affecting emergency department opioid administration to severely injured patients. Acad Emerg Med. 2004;11:1290–6.
Archer KR, Heins SE, Abraham CM, Obremskey WT, Wegener ST, Castillo RC. Clinical significance of pain at hospital discharge following traumatic orthopedic injury: general health, depression, and PTSD outcomes at 1 year. Clin J Pain. 2016;32:196–202.
Katz J, Seltzer Z. Transition from acute to chronic postsurgical pain: risk factors and protective factors. Expert Rev Neurother. 2009;9:723–44.
Kyranou M, Puntillo K. The transition from acute to chronic pain: might intensive care unit patients be at risk? Ann Intensive Care. 2012;2:36.
Opioid Coversion Calculator. 2016. https://www.practicalpainmanagement.com.
Poritz JMP, Mignogna J, Christie AJ, Holmes SA, Ames H. The Patient Health Questionnaire depression screener in spinal cord injury. J Spinal Cord Med. 2018;41:238–44.
Chen A, Ashburn MA. Cardiac effects of opioid therapy. Pain Med. 2015;16:S27–31.
von Elm E, Altman DG, Egger M, Pocock SJ, Gotzsche PC, Vandenbroucke JP, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. 2007;370:1453–7.
Chamberlain JD, Brinkhof MWG. Using strong inference to answer causal questions in spinal cord injury research. Spinal Cord. 2019;57:907–8.
Harvey LA. Relationships, associations, risk factors and correlations: nebulous phrases without obvious clinical implications. Spinal Cord. 2020;58:1–2.
Acknowledgements
We would like to acknowledge the Memorial Hermann—The Woodlands Trauma Services (Trauma Registry) for their assistance.
Funding
The research efforts of AS are supported by Mission Connect, a project of the TIRR Foundation. Further support was provided to AS and MH by Mission Connect Grants 016-104 and 016-115.
Author information
Authors and Affiliations
Contributions
AS was responsible for designing the study, linking the databases, extracting and analyzing data, interpreting results, writing the paper, and respondinging to revisions. CP was responsible for analyzing the data, interpreting results, writing the paper, and responding to revisions. JNB was responsible for extracting data and writing the paper. ARF and JLKK were responsible for guidance in statistical analyses and paper edits. MH was responsible for interpreting results, writing the paper, and respondinging to revisions.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
AS received approval for this study from the Institutional Review Board.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Stampas, A., Pedroza, C., Bush, J.N. et al. The first 24 h: opioid administration in people with spinal cord injury and neurologic recovery. Spinal Cord 58, 1080–1089 (2020). https://doi.org/10.1038/s41393-020-0483-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-020-0483-x
This article is cited by
-
Pharmacological management of acute spinal cord injury: a longitudinal multi-cohort observational study
Scientific Reports (2023)
-
Morphine-induced changes in the function of microglia and macrophages after acute spinal cord injury
BMC Neuroscience (2022)
