
Abstract
Hepatocellular carcinoma (HCC) occurs mainly in the liver associated with chronic hepatitis and hepatic cirrhosis as a result of prolonged viral infection. Transforming growth factor-β (TGF-β) induces the fibrosis in hepatic cirrhosis, although it is also an inhibitor of hepatocyte proliferation. To understand the role of TGF-β signaling in HCC progression, we analyzed gene expression in HCC cells in relation to TGF-β signaling using a two-way clustering algorithm. By the analysis, five HCC cell lines were classified into two groups according to their metastatic capacity. TGF-β receptor II (TGFBR2) was downregulated in metastatic cells, which did not show a response to TGF-β. Immunohistochemistry demonstrated clear membrane distribution of TGFBR2 in noncancerous hepatocytes, whereas reduced TGFBR2 expression was observed in 34 of 136 HCCs. In clinical cases, reduced TGFBR2 expression correlated with larger tumor size (P<0.001), poor differentiation (P<0.001), portal vein invasion (P=0.002), intrahepatic metastasis (IM) (P<0.001), and shorter recurrence-free survival (P=0.022). In conclusion, reduced TGFBR2 expression was associated with aggressive features of HCC such as IM, and may represent an immunohistochemical biomarker to detect aggressive HCC.
Similar content being viewed by others

Main
Hepatocellular carcinoma (HCC) is a common cause of death from cancer worldwide.1 Prolonged infection with hepatitis virus often causes chronic hepatitis, followed by liver cirrhosis.2 During the development of these liver diseases, transforming growth factor-β (TGF-β) has an important role in fibrosis of the lesions.3 HCCs mainly occur in those injured livers with activated TGF-β signaling, although TGF-β inhibits hepatocyte cell growth in the normal liver.4, 5
TGF-β signaling is activated when a TGF-β ligand binds to its receptor on the cell membrane. The downstream effectors, SMAD2 and SMAD3, together with SMAD4, translocate to the nucleus and regulate the expression of various genes, including cyclin-dependent kinase inhibitor 1A (CDKN1A), which is involved in cell growth arrest.6, 7 TGF-β signaling is also suggested to be involved in the malignant progression of tumors. TGF-β can induce epithelial–mesenchymal transition and promote tumor cell invasion, and may also have angiogenic and immunosuppressive effects on the tumor microenvironment, all of which promote metastasis.8
Mutations in the TGF-β superfamily genes have been found in various cancers. The TGF-β receptor II (TGFBR2) gene is frequently mutated in colon cancers,9, 10 gastric cancers,10, 11 and in gliomas12 with microsatellite instability. SMAD4 mutations occur mainly in pancreatic cancers, in which the SMAD4 gene was first identified as a tumor-suppressor gene.13 In HCCs, however, mutations in TGF-β superfamily genes are rare,14, 15 and alteration of TGF-β signaling is still unclear and controversial. To investigate alterations of TGF-β signaling in HCC progression, we compared the expression profiles of TGF-β signaling-related genes in HCC cells exhibiting different metastatic potential. We also investigated TGFBR2 expression in HCC cells.
MATERIALS AND METHODS
Clinical Specimens of HCC
HCCs and corresponding, noncancerous liver tissue were obtained from patients who underwent surgical resection at the Keio University Hospital, Japan. We analyzed 136 nodules resected from 92 patients, including 12 patients with multicentric HCC. A histological diagnosis of HCC was made according to the WHO criteria.16 The diagnosis of tumor recurrence was based on radiological findings and tumor markers in the serum. Time to recurrence was calculated as the period from the date of surgery until recurrence. This study was approved by the Ethics Committee of Keio University.
Cell Culture and TGF-β Treatment
The human HCC cell lines, PLC/PRF/5 and Hep G2, were obtained from the American Type Culture Collection (Manassas, VA, USA). KIM-1, KYN-2, and Li7 were established as previously reported.17, 18, 19 All the cells were grown in RPMI 1640 (Sigma-Aldrich, St Louis, MO, USA) medium supplemented with 10% fetal bovine serum (FBS), 100 U/ml penicillin, and 100 μg/ml streptomycin. For treatment of PLC/PRF/5 and Li7 cells with TGF-β, the cells were cultured in RPMI 1640 medium supplemented with 5 ng/ml TGF-β1 (PeproTech EC, London, UK) and 0.5% FBS.
Hierarchical Clustering
Gene-expression profiles of TGF-β-related genes in PLC/PRF/5, Hep G2, KIM-1, KYN-2, and Li7 cells were clustered using established algorithms implemented in the software program, Cluster.20 Centroid linkage clustering with uncentered correlation was used. TreeView software (http://rana.lbl.gov/EisenSoftware.htm) generated a visual representation of clusters. Microarray data are available at Genome Medicine Database of Japan (https://gemdbj.nibio.go.jp/dgdb/).
Western Blot
PLC/PRF/5, Hep G2, KIM-1, KYN-2, and Li7 cells were lysed in lysis buffer (0.1% SDS, 1% Nonidet P-40, 150 mM NaCl, 50 mM Tris–HCl (pH 7.5), 5 mM EDTA) supplemented with Complete Protease Inhibitor Cocktail (Roche Molecular Biochemicals, Mannheim, Germany). The lysates were separated by electrophoresis on NuPAGE 4–12% Bis–Tris gels (Invitrogen, Carlsbad, CA, USA), and transferred to PVDF membrane according to the manufacturer's instructions. The blotted membrane was probed with a rabbit TGFBR2 antibody (Upstate, Lake Placid, NY, USA) and bound antibody was detected with ECL Western blotting detection reagents (GE Healthcare, Uppsala, Sweden).
Semiquantitative RT-PCR
Total RNA was purified using the RNeasy Mini Kit (Qiagen, Valencia, CA, USA). Single-stranded cDNA was synthesized from 1 μg of total RNA using the oligo (dT) primer and M-MLV reverse transcriptase (Promega, Madison, WI, USA) at 42°C for 1 h. Primers and PCR cycles were as follows: SERPINE1 (sense, 5′-TCCTGGTTCTGCCCAAGTTCTC-3′; antisense, 5′-CACAAAGAGGAAGGGTCTGTCCA-3′, 30 cycles), and GAPDH (sense, 5′-AAGGTCATCCCTGAGCTGAACG-3′; antisense, 5′-CAAAGGTGGAGGAGTGGGTGTC-3′, 23 cycles). PCR products were separated by agarose gel electrophoresis and detected by staining with ethidium bromide.
Cell Proliferation Assay
In 24-well plates, three wells each of PLC/PRF/5 and Li7 cells were treated with, or without, TGF-β for 3 days. After 0, 1, 2, and 3 days of treatment, the culture medium was replaced with 10% WST-1 reagent (Roche Molecular Biochemicals) in 10% FBS/RPMI 1640, and incubated for 30 min at 37°C. The absorbance of the converted dye was measured at a wavelength of 450 nm, with background subtraction at 630 nm, using a Bio-Rad Model 550 microplate reader (Bio-Rad Laboratories, Hercules, CA, USA). Results were expressed as the ratio of viable cells relative to those on day 0.
IHC
Formalin-fixed, paraffin-embedded tissue sections were boiled for 30 min in 10 mmol/l Tris–HCl (pH 9.0), 150 mM NaCl for antigen retrieval, and labeled with rabbit polyclonal antibody against TGFBR2 (1:200) (Upstate) overnight at 4°C. Bound antibody was visualized using a peroxidase-conjugated secondary antibody (ImmPRESS, Vector Laboratories, Burlingame, CA, USA), and color developed with diaminobenzidine. After counterstaining with hematoxylin, sections were mounted on coverslips.
Statistical Analysis
The χ2-test was used when appropriate to determine the correlations between clinicopathological variables and TGFBR2 expression. Cumulative recurrence rate was calculated with the Kaplan–Meier method, and the log-rank test was applied to compare survival between different groups. In 92 consecutive patients who underwent surgery for HCC from 2003 through 2006, 12 patients of the liver transplantation were excluded from the analysis of recurrence-free analysis. All statistical analyses were carried out using SPSS statistical software (SPSS, Chicago, IL, USA).
RESULTS
TGF-β Superfamily Genes in HCC Cells
To understand the expression levels of TGF-β signaling-related genes, expression profiles of HCC cells were examined by two-way clustering analysis. In 12 625 probes on a GeneChip HG-U95A array, 93 probes targeting 56 genes were selected based on Gene Ontology annotation terms, including ‘transforming growth factor beta.’ Five HCC cell lines were roughly classified into two clusters, one of which involved PLC/PRF/5, Hep G2, and KIM-1 cells, and another, KYN-2 and Li7 cells (Figure 1). These cells have been previously classified into two groups on the basis of metastatic potential in a mouse intrahepatic metastasis (IM) model, in which orthotopically implanted KYN-2 and Li7 cells formed secondary foci in the mouse liver, whereas others did not.21 Thus, the classification by the clustering analysis in this study reflected the classification based on metastatic potential in the mouse model. In the central transducers of TGF-β signaling pathway (ligands–receptors–SMADs), TGFBR2 showed markedly different expression between the two groups. Mutations of the TGFBR2 gene frequently found in some cancers have not been identified in HCC; therefore, we speculated whether the reduced expression level of TGFBR2 causes suppression of TGF-β signaling without mutations, and selected it for further analyses. Although TGFBR2 expression was downregulated in metastatic (KYN-2 and Li7) cells, not all the TGF-β-responsive gene expression correlated with TGFBR2 expression levels. This suggests that heterogeneous TGF-β responses may be reflected in the expression signature.

Two-way clustering of TGF-β signaling-related genes in five HCC cell lines. The vertical axis corresponds to cells, and the horizontal axis to genes. Gene expression levels are presented by log(2) ratio to mean intensity, and depicted as color variation from red (high expression) to green (low expression).
The differential expression of TGFBR2 in the HCC cell lines was confirmed by RT-PCR (Supplementary Figure 1a) and Western blot analyses (Figure 2a). Compared with the nonmetastatic cells, TGFBR2 expression was reduced in the metastatic cells. Thus, TGFBR2 was downregulated at both the mRNA and protein level. Expression levels of TGF-β receptor I (TGFBR1), a binding partner of TGFBR2, were almost same in these cell lines (Supplementary Figure 1a).

TGFBR2 expression and response of hepatocellular carcinoma cells to TGF-β. (a) Western blot analysis shows a reduction of TGFBR2 expression in the KYN-2 and Li7 cells, compared with the others. Equal protein loading was confirmed by staining the blot with amido black (data not shown). (b) RT-PCR shows no response of KYN-2 and Li7 cells to TGF-β. Following treatment with (+), or without (−), TGF-β, expression of SERPINE1 was upregulated in PLC/PRF/5, Hep G2, and KIM-1 cells. (c) Cell proliferation assays in PLC/PRF/5 and Li7 cells treated with, or without, TGF-β, for 3 days. The growth ratio indicates the relative cell number compared with that of day 0 in each series.
Response to TGF-β in HCC Cells
To examine the functional role of the differential expression of TGFBR2, the response to TGF-β in HCC cells was assayed by semiquantitative RT-PCR (Figure 2b). After 3 h of treatment with 5 ng/ml TGF-β1, there was elevated expression of a TGF-β-inducible gene, SERPINE1 (plasminogen activator inhibitor type 1), in the nonmetastatic cells. In contrast, SERPINE1 expression was not detected in either the KYN-2 or the Li7 cells, before and after treatment. Similarly, another TGF-β-responsive gene, SMAD7, was upregulated in PLC/PRF/5 cells by TGF-β stimulation, but not in the Li7 cells (Supplementary Figure 1b).
We also evaluated the proliferative response of PLC/PRF/5 and Li7 cells to TGF-β. As shown in Figure 2c, proliferation of PLC/PRF/5 cells was reduced by treatment with TGF-β, whereas Li7 cells showed no significant difference. Upregulated expression of CDKN1A was observed in PLC/PRF/5 cells after TGF-β addition, but not in the Li7 cells (Supplementary Figure 1b). These results suggest that the growth arrest mediated by CDKN1A through TGF-β signaling is dependent on the expression level of TGFBR2.
TGFBR2 Expression in HCCs
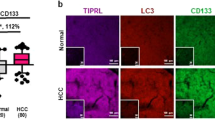
Expression levels of TGFBR2 in clinical cases of HCC were examined by immunohistochemistry (IHC). To optimize the conditions for IHC, sections of tumors formed in immunodeficient mice by subcutaneous inoculation of PLC/PRF/5 or Li7 cells were prepared. By boiling the sections for 30 min in 10 mmol/l Tris–HCl buffer (pH 9.0), TGFBR2 could be successfully detected in the cell membrane of PLC/PRF/5 cells, but not in the Li7 cells (Supplementary Figure 2). We performed IHC on 136 nodules of human HCC specimens using these optimal conditions. TGFBR2 was detected in noncancerous hepatocytes, especially on the cell membrane and corresponding to the expected localization for a membrane receptor (Figure 3). Bile duct cells and vascular endothelial cells also expressed TGFBR2 (Figure 3a; an asterisk and arrowheads, respectively). Staining levels in each cell type were basically homogenous. On the other hand, the expression level of TGFBR2 in cancer cells varied among nodules. Compared with noncancerous hepatocytes, unchanged expression of TGFBR2 was found in some nodules (Figure 3b), whereas reduced expression was seen in others (Figure 3c). From the total of 136 nodules examined, reduced expression (≥10% of tumor cells showing no membranous staining of TGFBR2) was observed in 34 nodules, and expression levels similar to that observed in the noncancerous hepatocytes was observed in 102 nodules (Table 1). Poorly differentiated cells frequently showed reduced expression of TGFBR2. In the cells that formed a tumor embolus (Figure 3d), TGFBR2 expression was significantly reduced compared with adjacent hepatocytes, and there was no membrane localization of TGFBR2. The results of IHC analyses from clinical patient samples demonstrate that reduced expression of TGFBR2 correlated with poor differentiation, portal vein invasion, and IM.

Immunolabeling of TGFBR2 in clinical specimens of HCC. (a) Nonneoplastic hepatocytes (N), bile duct epithelial cells (asterisk), and vascular endothelial cells (arrowheads) showed TGFBR2 immunoreactivity on the cell membrane. Unchanged (b), or reduced (c) expression of TGFBR2 was shown in tumor cells (T), compared with hepatocytes (N). (d) Tumor cells forming an embolus showed reduced TGFBR2 expression (arrow) compared with adjacent hepatocytes (N).
During a median follow-up of 26 months (range, 0–67 months), the time-to-recurrence was analyzed in 80 cases with HCC. Log-rank analysis showed that patients with reduced TGFBR2 expression had a significantly shorter time-to-recurrence (P=0.022), compared with patients with TGFBR2 expression level similar to the adjacent hepatocyte (Figure 4). Expression levels of TGFBR2 were different among foci of multicentric HCCs. Therefore, patients with at least one focus showing reduced TGFBR2 expression were classified into the reduced TGFBR2 group.

Kaplan–Meier curves for time to recurrence. Cumulative recurrence rates (%) of patients with unchanged and reduced TGFBR2 expression are indicated by solid and dotted lines, respectively.
DISCUSSION
TGFBR2 is a major TGF-β signaling molecule often found to be one of the genes altered in cancer. Its expression levels in HCC have been controversial and its biological role in HCC remains unclarified. Some reports show unchanged TGFBR2 expression in HCC compared with adjacent liver tissue,22 whereas others show downregulation in 5023 and 60%24 of HCCs. We found differential expression of TGFBR2 between metastatic and nonmetastatic HCC cells, and, with IHC, demonstrated reduced expression of TGFBR2 in 25% of HCC cases. TGFBR2 shows a clear membrane distribution in noncancerous hepatocytes and this can be useful when using IHC to assess specific downregulation in HCC. Although the mechanism of TGFBR2 downregulation in HCC remains unknown, microarray and RT-PCR analyses show that TGFBR2 gene expression is reduced at the mRNA level. Epigenetic silencing of TGFBR2 by promoter methylation occurs in stomach, lung, and prostate cancers.25, 26, 27 Considering that mutations or loss of the TGFBR2 gene are rare in HCCs, epigenetic silencing may be involved in reduced TGFBR2 expression in HCC.
Progression of HCC often leads to vascular invasion and IM, which correlate with recurrence after treatment, and poor prognosis.28, 29 IM is thought to develop through tumor cell dissemination through the portal vein.30 Previous studies using the mouse IM model indicate activation of RhoA21 and AKT,31 and overexpression of cortactin32 in metastatic HCC cells. We showed that the expression signature of TGF-β signaling-related genes classified the HCC cells into two groups according to their metastatic potential. Reduced TGFBR2 expression significantly correlated with the aggressive features of HCC. The results suggest that TGF-β signaling has a suppressive role in HCC progression, as downregulated TGFBR2 appears to result in impaired TGF-β signaling. However, TGF-β signaling in HCC is complicated. Giannelli and coworkers33, 34, 35 demonstrated the involvement of TGF-β signaling in promoting HCC growth, progression, and metastasis, and Coulouarn et al36 showed that the expression signature of the late TGF-β response predicts liver metastasis and poor outcome in HCC patients. Considering these findings, TGF-β signaling may not be completely abolished in the cell with reduced TGFBR2 expression.
Reduced TGFBR2 expression correlated with portal vain invasion in HCC cases, and poorly differentiated HCC cells showed lower TGFBR2 expression compared with well-differentiated cells. This suggests that HCC cells, with reduced TGFBR2 expression, seem to be more invasive and may promote IM. Recently, Matsuzaki et al38 showed the involvement of the TGF-β receptor-independent, JNK–SMAD3 pathway in HCC progression.38 The receptor activates SMAD3 by phosphorylation at the C-terminal region, whereas JNK phosphorylates the linker region of SMAD3, which is involved in tumor progression. In HCC cells with reduced TGFBR2 expression, it seems likely that the JNK–SMAD3 pathway may have a dominant role in cancer progression. Further studies are needed to elucidate the function of TGF-β signaling in HCCs with reduced TGFBR2 expression.
Although the role of TGF-β signaling in HCC progression remains controversial, we have shown that the reduced expression of TGFBR2 in HCC correlates significantly with aggressive features, such as IM and short time-to-recurrence. We suggest that reduced TGFBR2 expression may not only be a biomarker for IM, but also a predictive factor for recurrence of HCC.
References
El-Serag HB . Hepatocellular carcinoma: an epidemiologic view. J Clin Gastroenterol 2002;35:S72–S78.
Arakawa M, Kage M, Sugihara S, et al. Emergence of malignant lesions within an adenomatous hyperplastic nodule in a cirrhotic liver. Observations in five cases. Gastroenterology 1986;91:198–208.
Gressner AM, Weiskirchen R, Breitkopf K, et al. Roles of TGF-beta in hepatic fibrosis. Front Biosci 2002;7:d793–d807.
Nakamura T, Tomita Y, Hirai R, et al. Inhibitory effect of transforming growth factor-beta on DNA synthesis of adult rat hepatocytes in primary culture. Biochem Biophys Res Commun 1985;133:1042–1050.
Carr BI, Hayashi I, Branum EL, et al. Inhibition of DNA synthesis in rat hepatocytes by platelet-derived type beta transforming growth factor. Cancer Res 1986;46:2330–2334.
Massague J, Blain SW, Lo RS . TGFβ signaling in growth control, cancer, and heritable disorders. Cell 2000;103:295–309.
Derynck R, Akhurst RJ, Balmain A . TGF-β signaling in tumor suppression and cancer progression. Nat Genet 2001;29:117–129.
Siegel PM, Massague J . Cytostatic and apoptotic actions of TGF-β in homeostasis and cancer. Nat Rev Cancer 2003;3:807–821.
Markowitz S, Wang J, Myeroff L, et al. Inactivation of the type II TGF-beta receptor in colon cancer cells with microsatellite instability. Science 1995;268:1336–1338.
Myeroff LL, Parsons R, Kim SJ, et al. A transforming growth factor beta receptor type II gene mutation common in colon and gastric but rare in endometrial cancers with microsatellite instability. Cancer Res 1995;55:5545–5547.
Park K, Kim SJ, Bang YJ, et al. Genetic changes in the transforming growth factor beta (TGF-beta) type II receptor gene in human gastric cancer cells: correlation with sensitivity to growth inhibition by TGF-beta. Proc Natl Acad Sci USA 1994;91:8772–8776.
Izumoto S, Arita N, Ohnishi T, et al. Microsatellite instability and mutated type II transforming growth factor-beta receptor gene in gliomas. Cancer Lett 1997;112:251–256.
Hahn SA, Schutte M, Hoque AT, et al. DPC4, a candidate tumor suppressor gene at human chromosome 18q21.1. Science 1996;271:350–353.
Kawate S, Takenoshita S, Ohwada S, et al. Mutation analysis of transforming growth factor beta type II receptor, Smad2, and Smad4 in hepatocellular carcinoma. Int J Oncol 1999;14:127–131.
Yakicier MC, Irmak MB, Romano A, et al. Smad2 and Smad4 gene mutations in hepatocellular carcinoma. Oncogene 1999;18:4879–4883.
Hirohashi S, Ishak KG, Kojiro M, et al. Hepatocellular carcinoma. In: Hamilton SR, Aaltonen LA (eds). Tumours of the Digestive System. IARC Press: Lyon, 2000, pp 159–172.
Murakami T . Establishment and characterization of human hepatocellular carcinoma cell line (KIM-1). Acta Hepatol Jpn 1984;25:532–539.
Yano H, Maruiwa M, Murakami T, et al. A new human pleomorphic hepatocellular carcinoma cell line, KYN-2. Acta Pathol Jpn 1988;38:953–966.
Osada T, Sakamoto M, Ino Y, et al. E-cadherin is involved in the intrahepatic metastasis of hepatocellular carcinoma. Hepatology 1996;24:1460–1467.
Eisen MB, Spellman PT, Brown PO, et al. Cluster analysis and display of genome-wide expression patterns. Proc Natl Acad Sci USA 1998;95:14863–14868.
Genda T, Sakamoto M, Ichida T, et al. Cell motility mediated by rho and rho-associated protein kinase plays a critical role in intrahepatic metastasis of human hepatocellular carcinoma. Hepatology 1999;30:1027–1036.
Abou-Shady M, Baer HU, Friess H, et al. Transforming growth factor betas and their signaling receptors in human hepatocellular carcinoma. Am J Surg 1999;177:209–215.
Kiss A, Wang NJ, Xie JP, et al. Analysis of transforming growth factor (TGF)-alpha/epidermal growth factor receptor, hepatocyte growth Factor/c-met, TGF-beta receptor type II, and p53 expression in human hepatocellular carcinomas. Clin Cancer Res 1997;3:1059–1066.
Musch A, Rabe C, Paik M, et al. Altered expression of TGF-beta receptors in hepatocellular carcinoma—effects of a constitutively active TGF-beta type I receptor mutant. Digestion 2005;71:78–91.
Pinto M, Oliveira C, Cirnes L, et al. Promoter methylation of TGFbeta receptor I and mutation of TGFbeta receptor II are frequent events in MSI sporadic gastric carcinomas. J Pathol 2003;200:32–38.
Zhang HT, Chen XF, Wang MH, et al. Defective expression of transforming growth factor beta receptor type II is associated with CpG methylated promoter in primary non-small cell lung cancer. Clin Cancer Res 2004;10:2359–2367.
Zhao H, Shiina H, Greene KL, et al. CpG methylation at promoter site -140 inactivates TGFbeta2 receptor gene in prostate cancer. Cancer 2005;104:44–52.
Nagao T, Inoue S, Goto S, et al. Hepatic resection for hepatocellular carcinoma. Clinical features and long-term prognosis. Ann Surg 1987;205:33–40.
Nagao T, Inoue S, Yoshimi F, et al. Postoperative recurrence of hepatocellular carcinoma. Ann Surg 1990;211:28–33.
Yamanaka N, Okamoto E, Fujihara S, et al. Do the tumor cells of hepatocellular carcinomas dislodge into the portal venous stream during hepatic resection? Cancer 1992;70:2263–2267.
Nakanishi K, Sakamoto M, Yasuda J, et al. Critical involvement of the phosphatidylinositol 3-kinase/Akt pathway in anchorage-independent growth and hematogeneous intrahepatic metastasis of liver cancer. Cancer Res 2002;62:2971–2975.
Chuma M, Sakamoto M, Yasuda J, et al. Overexpression of cortactin is involved in motility and metastasis of hepatocellular carcinoma. J Hepatol 2004;41:629–636.
Mazzocca A, Fransvea E, Lavezzari G, et al. Inhibition of transforming growth factor beta receptor I kinase blocks hepatocellular carcinoma growth through neo-angiogenesis regulation. Hepatology 2009;50:1140–1151.
Mazzocca A, Fransvea E, Dituri F, et al. Down-regulation of connective tissue growth factor by inhibition of transforming growth factor beta blocks the tumor-stroma cross-talk and tumor progression in hepatocellular carcinoma. Hepatology 2010;51:523–534.
Fransvea E, Angelotti U, Antonaci S, et al. Blocking transforming growth factor-beta up-regulates E-cadherin and reduces migration and invasion of hepatocellular carcinoma cells. Hepatology 2008;47:1557–1566.
Coulouarn C, Factor VM, Thorgeirsson SS . Transforming growth factor-beta gene expression signature in mouse hepatocytes predicts clinical outcome in human cancer. Hepatology 2008;47:2059–2067.
Matsuzaki K, Murata M, Yoshida K, et al. Chronic inflammation associated with hepatitis C virus infection perturbs hepatic transforming growth factor beta signaling, promoting cirrhosis and hepatocellular carcinoma. Hepatology 2007;46:48–57.
Murata M, Matsuzaki K, Yoshida K, et al. Hepatitis B virus X protein shifts human hepatic transforming growth factor (TGF)-beta signaling from tumor suppression to oncogenesis in early chronic hepatitis B. Hepatology 2008;49:1203–1217.
Acknowledgements
This study was supported by Grant-in-aid for Scientific Research on Priority Areas from the Ministry of Education, Culture, Sports, Science, and Technology (MEXT); grants for the Health and Labor Sciences Research and the Third Term Comprehensive 10-Year Strategy for Cancer Control from the Ministry of Health, Labor, and Welfare of Japan; and Research Grants for Life Sciences and Medicine from the Keio University Medical Science Fund.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on the Laboratory Investigation website
Rights and permissions
About this article
Cite this article
Mamiya, T., Yamazaki, K., Masugi, Y. et al. Reduced transforming growth factor-β receptor II expression in hepatocellular carcinoma correlates with intrahepatic metastasis. Lab Invest 90, 1339–1345 (2010). https://doi.org/10.1038/labinvest.2010.105
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/labinvest.2010.105
Keywords
This article is cited by
-
Comparative study of the effects of PEGylated interferon-α2a versus 5-fluorouracil on cancer stem cells in a rat model of hepatocellular carcinoma
Tumor Biology (2016)
-
Upregulation of integrin β4 promotes epithelial–mesenchymal transition and is a novel prognostic marker in pancreatic ductal adenocarcinoma
Laboratory Investigation (2015)
-
TGFβR2 is a major target of miR-93 in nasopharyngeal carcinoma aggressiveness
Molecular Cancer (2014)
-
Inflammation and liver tumorigenesis
Frontiers of Medicine (2013)
-
TGF-β – an excellent servant but a bad master
Journal of Translational Medicine (2012)

{kind=link}
{kind=link}