
Abstract
Critical analysis of recent research suggesting that light pollution causes Parkinson's disease (PD) reveals that such a hypothesis is unsustainable in the context of therapeutic use of light in treating various neuropsychiatric conditions. Reinterpretation of their findings suggests that retinal damage caused by prolonged light exposure may have contributed to the observed enhancement of experimental PD. To test this hypothesis further, forty-two Sprague Dawley rats received microinjections of 6-hydroxydopamine (6-OHDA), 1-methyl-4-phenyl-2, 4, 6-tetrahydropyridine (MPTP), paraquat or rotenone into the vitreal mass in doses so minute that the effects could not be attributed to diffusion into brain. Significant changes in five motor parameters consistent with symptoms of experimental PD were observed. These findings support the interpretation that the retina is involved in the control of motor function and in the aetiology of PD.
Similar content being viewed by others
Introduction
A recent study proposes that light pollution plays a major role in the epidemiology of Parkinson's disease (PD)1. This claim was based on three types of data: First, an empirical study was undertaken whereby the exposure of albino rats to 3000 Lux (Lx) bright light for 20 to 90 days produced an Increase in melanin in the nigro-striatal dopamine (NSD) system and a concomitant tyrosine hydroxylase (TH) and dopamine (DA) deficiency. This was compared to a control group whereby light exposure combined with transection of the optic tract led to the conclusion that the observed changes were due to light penetration through tissue and bone damaged the NSD system. The second line of evidence was based on a qualitative revaluation of a study assessing the amount of nigral pigmentation in several mammalian species2, correlating their behavioural repertoire with environmental light exposure. It was selectively assumed that the pigment neuromelanin was toxic and from this was drawn the conclusion that increased light exposure increased toxic, NSD pigmentation. Finally, epidemiological data was presented linking light pollution with the incidence of PD in the continental United States.
While this work provides a novel and bold hypothesis (the light pollution hypothesis; LPH), it does so on the basis of crucial citation omission, compromised methodology and what appears to be a paucity of key concepts that would have otherwise dissuaded such an interpretation. On this basis, the present critique serves a twofold purpose: first to prevent the potential damage to ongoing scientific work, consequential to a dearth of adequate citation and robust methodology. Second, to prevent the generation of unfounded criticism toward a potential therapeutic approach that could provide critical relief to PD sufferers. It would be imprudent for this to go unchallenged.
The first of the crucial concepts not adequately addressed pertains to the significance of neuromelanin in PD. The substantia nigra (SN) contains the cell bodies of the NSD and is so named because it appears as the largest area of black substance in the central nervous system (CNS). In the first post-mortem studies undertaken in PD patients it was reported that this midbrain area appeared blanched and was totally devoid of its dark pigment3,4, a finding reported consistently over the past 40 years5,6,7 and now deemed a reliable biomarker for the disease8. Not only does the underlying data supporting the LPH fail to account for this, but increased neuromelanin after light exposure in their aetiological model of PD is reported, which does not typify Parkinsonian brain3,5. While we acknowledge the high degree of controversy as to whether neuromelanin maintains a protective or a detrimental role in the disease9,10,11, the LPH is based on a lean historical background which fails to address this issue and is tenable only by omitting reference to this crucial phenomenon. Attributing the observed deficit in TH and striatal DA deficiency to increased neuromelanin is a contentious issue. Furthermore, it fails to account for important functions of neuromelanin in three critical areas of the CNS containing melanocytes12: that is, the retina, the pineal and the SN where neuromelanin can serve a homeostatic9 and possibly a protective role4,13,14. Reference to any homeostatic role of melanin pertains to well documented concepts such as DA and melatonin existing in functional opposition15, whereby DA production and release increases in light and decreases in darkness16,17, while melatonin does the opposite. Within melanocytes, melatonin and melanin also function in opposition across the diurnal cycle18 whereby melatonin production is slowed in the presence of light19 and pigments disperse and aggregate in the presence of light and dark, respectively. While the Parkinsonian brain is characterised by DA deficiency and absence of neuromelanin, the LPH does not address DA deficiency in the presence of increased neuromelanin and offers no explanation for this vital discrepancy. The LPH overlooks the essential biological processes that these substances subserve and by doing so is rendered ineffectual.
The second major deficiency of the LPH is the failure to address formal studies describing improvement in PD symptoms after short or long term, strategic exposure to light. Several accounts of improvement in PD symptoms after increased exposure to ambient light or therapeutic application of bright light have been overlooked in formulating the LPH. These include a case series study20, an open label study21, a retrospective study22, a double blind trial23 and PD and depression studies implementing REM sleep deprivation24,25,26 as well as preclinical studies27,28,29,30. Furthermore, while one study reports sustained improvement in PD following bright light therapy for up to 8 years with no adverse effects on PD reported22 there is an increasing interest in exploring such non-invasive therapeutic avenues for PD12,22,31.
Equally problematic is a third example whereby the omission of citations regarding the effects of light exposure on the functional integrity of the retina also compromises the impact of the LPH. Retinal damage due to light exposure has been studied extensively in animals and man for more than 4 decades and it is clear that polychromatic light can induce retinal damage at intensities which are only a fraction of that presumed to occur as described in the LPH (1200 to 2500 Lx32; ≈800 Lx33; 2260 Lx34; ≈1615 Lx40; cf. Romeo et al (2013)1, 3000 Lx). Furthermore, the severity of retinal destruction is related to other variables such as species tested, duration of exposure, temperature and wavelength32,35,36,37,38,39,40, with the Sprague Dawley Albino strain rats being particularly sensitive to retinal destruction at low intensities and for short durations of exposure41. Consequently, the LPH was formulated on the basis of implementing bright light exposure as the independent variable. However, while it was intended as a source of chronic photic stimulation, it would have caused functional retinal damage which, in all probability, would produce the same level of circadian and visual incapacitation as that produced by enucleation; the latter of which has been shown to enhance the severity of experimental PD42. While it is acknowledged that enucleation may appear to be more anatomically severe than bright light exposure, both procedures have been reported to cause photoreceptor damage43,44, retinal thinning45,46 and retinal ganglion cell (RGC) loss47. The resulting functional changes include impaired vision and blindness48 as well as compromised circadian function12,49,50. Given that the paradigm underlying the LPH did not control for retinal damage, significant limitations on the interpretability of the results emerge.
Notwithstanding the methodological and interpretive problem of retinal damage resulting from the implementation of 3000 Lx as the independent variable, there are several other methodological problems with the empirical support for the LPH. The most obvious example of compromised methodology involves the assessment of nigral neuromelanin after bright light exposure versus optic nerve transection. In the bright light exposure group stereological counting was implemented revealing an increase in the number of melanin positively stained cells. This was more than 11.5 times higher in the light exposed group compared to the low light exposed counterparts. However, in the control preparation of optic nerve transection, melanin stereological counting was not performed but only two representative pictomicrographs were shown. This presents the obvious sampling problem that two pictomicrographs, without parallel stereological counting, may not be a comparable form of assessment of nigral melanin in the control group. The volume of tissue assessed in the pictomicrographs represents only a minute fraction (.0059 mm3) of the total volume of assessable nigral tissue and does not provide an equivalent comparison for the experimental group. On this basis, it is inappropriate to draw any definitive inference about the hypothesized route of light pollution and the toxicity of neuromelanin: the key issues that this study was meant to address.
Equally perplexing is the experimental design employed to study the effects of light exposure on neuromelanin and TH activity. In the first part of the study rats were exposed to their respective light schedules for 90 days with TH and neuromelanin histochemistry being performed at 111 days after birth. However the control group receiving the optic tract transection were operated at 90 days after birth, given 21 days to recover from surgery with exposure to light for 120 days. Consequently, the age of the control rats receiving transection at the time of sacrifice was 217 days, almost twice as long as in the non-transected group. In consideration of abundant reports describing increases in neuromelanin with age2,51,52 while TH decreases53,54 the observed changes in both of these variables in the transected group could well have been due to age difference rather than light entering the brain via direct penetration. This methodological oversight further obscures the interpretability of their findings.
There also remains a major drawback in the conclusions drawn from findings emerging from the application of 3,000 Lx of light exposure as the independent variable representing the theoretical construct of “light pollution”. The parallel between 3000 Lx tested in their experimental model and the frequencies of light suggested to be detrimental in their epidemiological study remains highly speculative. Furthermore, how their model using polychromatic light relates specifically to the proposed toxicity of infrared (IR) or near-infrared (NIR) radiation emission is also an enigma. The article cited for the purpose of demonstrating that IR and NIR light penetrates the skull and tissue55 was, in fact, the core work underlying the development of IR and NIR radiospectometry. This, as a non-invasive technique, is considered to be in early phase development as the light frequencies employed only penetrate into approximately10 mm of white matter56. In general, IR radiospectometry is used for evaluating heamodynamics in cortical studies and not for assessing deep brain areas57,58,59,60,61. In fact, when IR or NIR light is applied to damaged cells, in particular NSD cells, functional repair ensues62. Calculation of the quantity of light reaching deep brain structures adjacent to SN tissue after 3000 Lx of “light pollution”, was in the range of 1.5 × 10−6 to 1.5 × 10−7 Lx, based on the findings reported in (Van Brunt et al. (1964)63 as cited in Romeo et al. (2013)1. This minute amount of NIR light contrasts dramatically to the amount applied to NSD neurones to induce repair (0.06 Lx)62.
By suggesting that light pollution causes degeneration of the NSD system, the LPH does not take the life style features of PD patients into account. First they are depressed64,65,66 and depressed patients can be photophobic67,68 thereby purposely avoiding light exposure. Furthermore, many Parkinson's patients live in nursing homes which are characteristically lacking in adequate ambient light69,70,71,72. On this basis, PD patients are not routinely living in situations where they are exposed to light pollution, particularly since many are institutionalised as the disease progresses. To our knowledge no evidence exists suggesting that admission into poorly lit nursing homes is associated with slowing the progression of the disease.
In summary, the first part of this review disputes the LPH in two ways: First, it demonstrates a substantial omission in citation of the existing background evidence which limits their interpretations and fails to support the existence of the proposed mechanisms. Second, it reveals encumbering methodological errors which not only weaken the empirical grounding but open the way for re-examination of the role of the visual system in the aetiology of neurological disorders.
In particular, we were interested in the oversight regarding the method of retinal stimulation whereby albino rats were exposed to 3,000 Lx of bright light. Rather than stimulating visual and non- visual pathways from the retina to the brain, such exposure can produce severe retinal pathology, photoreceptor death, retinal thinning and retinal ganglion cell (RGC) loss43,44,45,46,47,105 with functional consequences extending to include blindness and impaired circadian function48,49,50. This is an important distinction not only because enucleation can enhance recovery from experimental PD42 but also because localized, intravitreal (IVIT) L-dopa can facilitate recovery from this condition72. Such findings are consistent with the suggestion that the retina plays an important role in the aetiology and treatment of PD12. To test the role of the retina in the control of motor function we injected four different neurotoxins into the vitreous humour of Sprague-Dawley rats in minute doses to determine if any signs of experimental PD ensued. The substances injected included the Parkinsonian Neurotoxins 6-hydroxydopamine (6-OHDA) and 1-Methyl-4-Phenyl,-1, 2, 3, 6-tetrahydropyridine (MPTP) and the insecticide rotenone (ROTE) and herbicide paraquat (PARA). It is interesting to note that while these toxins have also been shown to produce retinal damage which is anatomically and pathologically similar to the effects of bright light exposure and enucleation73,74,75,76, the effects of IVIT injections on motor performance is unknown. With the IVIT administration of these toxins limiting their diffusion by i) minute dosing regimens ii) restrictive mechanisms of action and iii) distinct bodily compartmentalization (i.e. retina vs. brain), any observed effects would not be attributable to direct involvement of traditional motor systems such as the NSD system. We therefore hypothesize that if localised IVIT injections produce Parkinsonian-like responses in a pre-clinical model of PD then this suggests that the retina may be importantly involved in the control of motor function.
Results
6-OHDA and PARA Study
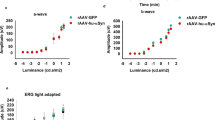
As shown in Fig. 1 (left trace) chronic, IVIT injection of 6-OHDA or PARA into the vitreous caused decrements in horizontal movement during the light (L) and dark (D) phases of the LD cycle. Analysis using ANOVA reveals a significant main effect (F = 3.293; p = 0.017) during the L phase with pair-wise comparisons (LSD) revealing highly significant differences in animals injected with IVIT 6-OHDA and PARA when compared to their pre-injection performance (p = 0.000 and p = 0.019, respectively).

The effect of intravitreal (IVIT) injection of 4 neurotoxins on horizontal movement.
Injections were made with 2 μl of isotonic saline (open bars; left traces), 2 μl of 1 μg/μl of 6-OHDA (solid bars), 2 μl of 2.57 μg/μl of paraquat (diagonal bars), 2 μl DMSO as vehicle (open bars; right traces), 2 μl of 25 μg/μl of MPTP (black bars with white mottling) or 2 μl of 2 μg/μl rotenone (open bars with black mottling), in Sprague Dawley Rats injected once weekly for 6 weeks. Control measurements were made prior to commencing the injection regimen then injections were made weekly for six weeks with all rats tested 2 weeks after the last injection during the eighth week. All rats were tested during the light (L) and dark (D) phases of the L/D cycle. ANOVA revealed significant differences between each treatment group and their control condition with post hoc comparison and p values stated as + = 0.05 to 0.01, ++ = 0.001 to 0.005 and +++ = 0.005 to .000. Significant between group comparisons are represented as actual p values. T-bars represent the S.E.M.
During the D phase horizontal movement was significantly altered in the 6-OHDA and PARA groups compared to controls (ANOVA main effects F = 6.096; p = 0.001). Pair wise comparisons revealed significant differences for the pre-6-OHDA and PARA groups when each was compared with their pre-injection control performance (p = 0.010 and p = 0.000, respectively).
In Fig. 2 the effects of the four neurotoxins, when administered by the IVIT route, produced minor effects upon vertical movement during the L phase. A significant trend was seen for the main effect with a tendency toward impaired vertical movement in those injected with 6-OHDA or PARA (left trace; F = 2.435; p = 0.058). Pair wise comparisons revealed that only those rats injected with IVIT PARA showed a strong trend toward impaired vertical movement when pre-injection performance was compared to that occurring after IVIT injection (p = 0.053).

The effect of intravitreal (IVIT) injection of 4 neurotoxins on vertical movement.
Injections were made with 2 μl of isotonic saline (open bars; left traces), 2 μl/of 2 μg of 6-OHDA (solid bars), 2 μl of 2.57 μg/μl of paraquat (diagonal bars), 2 μl DMSO as vehicle (open bars; right traces), 2 μl of 25 μg/μl of MPTP (black bars with white mottling) or 2 μl of 2 μg/μl rotenone (open bars with black mottling), in Sprague Dawley Rats injected once weekly for 6 weeks. Control measurements were made prior to commencing the injection regimen then injections were made weekly for six weeks with all rats tested 2 weeks after the last injection during the eighth week. All rats were tested during the light (L) and dark (D) phases of the L/D cycle. ANOVA revealed significant differences between each treatment group and their control condition with post hoc comparison and p values stated as + = 0.05 to 0.01, ++ = 0.001 to 0.005 and +++ = 0.005 to 0.000. Significant between group comparisons are represented as actual p values while the asterisk (*) indicates significant trends. T-bars represent the S.E.M.
There were no statistical differences in vertical movement between 6-OHDA and PARA (F = 1.190; p = 0.340), injected rats when tested during the D phase (Fig. 2). However, it is noted that the mean difference in vertical movement in pre versus post-injection performance in 6-OHDA injected rats was opposite to that seen in vehicle injected controls.
As shown in Table 1, the ability to retract an extended limb during the L phase was impaired by the chronic IVIT injection of 6-OHDA and PARA and was highly significant (Main Effect F = 4.754; p = 0.006). Post hoc analysis revealed that when the latency to retract in 6-OHDA and PARA injected animals was compared with their pre-injection performance, a significant difference was observed that was not seen in vehicle injected controls (p = 0.022 and p = 0.003, respectively).
The ability to retract an elevated limb was more seriously impaired in 6-OHDA and PARA injected animals, when tested during the D phase (Fig. 2) than during the L phase (Main Effect: F = 2.468; p = 0.000). Post hoc pair wise compassion using LSD revealed that both 6-OHDA and PARA injected animals were significantly impaired compared to their pre-injection control performance (p = 0.002 in both cases) as well as in relation to their vehicle-injected controls (p = 0.001 and .004, respectively).
The effect of 6-OHDA on the ability to step during the L phase when compared to pre-injection performance was significant impaired as revealed by Wilcoxon analysis (p = 0.008) as were rats after PARA when compare to their own control performance (p = 0.008). During the D phase of the L/D cycle only the 6-OHDA treated rats were significantly impaired when compared to their post-injection performance as revealed by LSD post-hoc comparisons (p = 0.010).
Table 1 illustrates the effect that IVIT injection had on the VHT scores during the L phase test in all rats treated with 6-OHDA and PARA. With a significant Main effect observed after these two toxins were administered chronically (F = 6.038, p = 0.008) only those treated with 6-OHDA or PARA displayed an elevated VHT ratio when compared to their pre-injection performance (p = 0.024; p = 0.000, respectively). During the D phase there was again a robust main effect on VHT scores due the various treatment (Table 1: F = 9.209; p = 0.000). When the pre-injection performance was compared to that occurring after the IVIT injection, vehicle, 6-OHDA and PARA injected animals all were significantly different as revealed by post-hoc tests (p = 0.039; p = 0.004 and p = 0.000, respectively). Only those injected with PARA showed a strong trend toward a higher VHT score when compared to vehicle controls (p = 0.056).
MPTP and ROTE Study
The effects of IVIT MPTP or ROTE on horizontal movement are expressed in Figure 1 (right trace). After the IVIT administration of MPTP or ROTE ANOVA revealed a significant main effect on horizontal movement during the L phase (F = 3.562; p = 0.012). Pair-wise comparisons revealed a significant decrease in horizontal movement between pre- and post- MPTP injected by the IVIT route (p = 0.013), while those receiving IVIT ROTE showed a decrement in motor performance which was also highly significant (p = 0.009). During the D phase horizontal movement was not significantly altered after MPTP and ROTE (ANOVA Main effect F = 2.013; p = 0.105) and Pair wise comparisons in the MPTP and ROTE groups were not performed.
Analysis of the D phase vertical movement in rats injected with IVIT MPTP or ROTE (Fig. 2; right trace) revealed a significant Main effect (F = 5.692; p = 0.001) with post hoc paired comparisons revealing a significant change in MPTP treated rats (p = 0.039) when compared with their pre-injection control performance. A significant change in vehicle injected rats was also seen before versus after injection (p = 0.000).
There were no significant treatment effects for vertical movement in MPTP and ROTE injected rats when tested during the D phase (F = 1.381; p = 0.289). However, Mauchley's test revealed a significant difference in sphericity between the groups (p = 0.011) which permitted nonparametric analysis revealing a significant trend between the vehicle and ROTE treated groups (Table 2; Wilcoxon Signed Rank, exact significance; 1 tailed, p = 0.055). Similarly, the same analysis performed between the vehicle and ROTE difference scores for this parameter revealed a significant difference between the two groups (exact significance; 1 tailed p = 0.039). There were no other significant differences seen with other comparisons.
There was no significant main effect for limb retraction during the L phase of the L/D cycle (F = 2.082; p = 0.077) for the group comparison but further analysis was carried out with Wilcoxon Signed Rank Test after Machley's test again revealed a significant difference between the pre-MPTP performance compared to post- MPTP treatment and this difference was highly significant (exact significance; 1 tailed p = 0.000). Similar analysis performed on the vehicle and MPTP treated rats after injection revealed a significant impairment in this parameter (exact significance; 1 tailed p = 0.016) while no other comparisons were significantly different at this time.
Similarly, while a main effect was not observed between the groups for retraction during the D phase (F = 2.468; p = 0.120), the presence of a significant difference in sphericity permitted further non-parametric testing between the pre-MPTP and MPTP treated groups, the pre-ROTE and ROTE treated groups and the ROTE vs vehicle treated groups with all comparisons revealing a significant difference (Wilcoxon Signed Rank, exact significance; 1 tailed p = 0.039, 0.005 and 0.004, respectively).
While no significant treatment effect was observed in the ability to step up or down from an elevated platform during the L phase (Main Effect: F = 2.742; p = 0.107) a significant difference in sphericity between the groups on this parameter again permitted analysis with the Wilcoxon Signed Rank Test. There was a severe impairment in the ability to step in the pre-MPTP vs the post MPTP group (exact significance; 1 tailed p = 0.008) and in the vehicle versus the MPTP comparison (Wilcoxon Signed Rank Test, exact significance; 1 tailed p = 0.008). In addition, the Vehicle versus the MPTP treated groups were significantly different when tested after the completion of the injection regime (Wilcoxon Signed Rank Test, exact significance; 1 tailed p = 0.031).
A similar effect on sphericity (0.008) in the presence of a non-significant treatment effect (F = 1.381; p = 0.289) revealed a significant difference between the pre-vehicle vs the vehicle treated group for latency to step during the D phase (Wilcoxon Signed Rank Test, exact significance; 1 tailed p = 0.039). A significant effect was also observed for the non-parametric comparison between the pre-MPTP and MPTP injected animals (Wilcoxon Signed Rank Test, exact significance; 1 tailed p = 0.031).
There was no significant effect of MPTP or ROTE on the VHT score during the L phase (Main Effect: F = 0.660; p = 0.656) or D phase (Main Effect: F = 1.797; p = 0.144) of the L/D cycle. Similarly, there was no significant effect of 6-OHDA and PARA or MPTP and ROTE on body weight for the duration of the 8 week period of observation of the study. (ANOVA: F = 0.109, p = 0.897 and F = 0.136, p = 0.0873, respectively).
Discussion
The present results demonstrate that symptoms of experimental PD can be observed after the IVIT injection of minute doses of 6-OHDA, MPTP, PARA and ROTE. These results, taken together with previous research42,72,78,79 suggest that the retina is intimately involved with the onset and progression of PD. However, it is important to bear in mind that the present study examines only a limited number of symptoms and, as is the case with modelling any disease, extrapolation to the aetiology, progression and treatment of PD itself awaits further experimental and clinical confirmation. In addition, given that the precise pathological and/or neurochemical changes underlying the observed behavioural effects were not measured in the present study, several testable hypotheses can now emerge to determine the underlying links between the retina and brain which may mediate the observed effects. The first testable hypothesis as to whether enucleation42, optic nerve transection1, exposure to high intensities of light1,44,45,46,47 or contact with toxins including insecticides and herbicides73,74,75,76, share the same critical factor by producing retinal damage is an important one. This is based on the observation that retinal degeneration, photoreceptor damage, RGC loss, retinal thinning as well as visual impairment and impaired circadian function, are all reported after these treatments and conditions are applied and are routinely observed in PD and its models77,78. A further example of this may be inferred from the sequelae after methyl alcohol poisoning. Medical intervention serves to prevent the formation of formic acid which can damage the retina and basal ganglia79, with the order of events being critical: blindness, the development of extrapyramidal symptoms and destruction of the NSD system80 with impaired motor function commencing with the onset of retinal damage. Moreover, the risk factors in some professions associated with PD may follow a similar pattern. For example, epidemiological studies have shown welding and boxing are associated with increased incidence of PD81,82 with the critical events being heavy metal vapor exposure and cerebral trauma as the proposed mechanisms, respectively. However, given that welding flash can cause retinal damage83 and that eye trauma is common in boxers84, it is reasonable to conclude that retinal involvement may be a precipitating factor12,42,72.
It is interesting that the different neurotoxins employed in the present study exerted different effects on motor function after IVIT injection. While 6-OHDA and PARA treated rats showed the most severe impairment, MPTP and ROTE treated rats displayed less severe motor symptoms in regard to the number of parameters affected. In addition, while the number of motor parameters affected during the L versus the D phase of the L/D cycle was similar in the 6-OHDA/PARA treated groups those treated with MPTP showed more impairment during the L phase while those treated with ROTE were more seriously affected during the D phase. Such differences could serve to define which toxins affect motor versus circadian function12. This is an important finding in view of reports describing DA neurotransmission as being under circadian control85,86,87.
While reevaluation of the data underlying the LPH does not provide strong empirical support suggesting that events in the retina can alter normal processes downstream in deep brain the retina does share functional similarities with the NSD system. That retina and nigral cells are derived from the same portion of the neural crest12 resulting in the formation of melanocytes, intimates that such cells in these different locations may be light sensitive and thereby increase melanin synthesis and induce pigment dispersion in the presence of photic stimulation: such is the case with more superficial structures such as the retina and the pineal88,89. However, without demonstration of an anatomical link between the NSD system and the retina the role of the retina in the control of motor performance and in the development of PD remains hypothetical and awaits further empirical grounding.
It is interesting to note that while there are several routes of exposure that have been hypothesized to explain how toxins such as PARA and ROTE enter the brain and potentially damage the NSD system there are limitations to this interpretation. For example, while there is speculation on the peripheral route by which PARA may induce its toxic effects90,91, it has been demonstrated that it does not pass the blood-brain barrier92 and has an affinity for the retina93, providing an alternative to more traditional routes such as the gut or skin. Given that the eye provides a medium by which the environment has direct contact with brain tissue (i.e. the retina), the present work supports the contention that very minute doses of toxin may have a most profound effect on deep brain function and may even participate in the induction of the disease. In the present study, even though motor impairment was seen after several minute doses of toxin were administered there was little change in body weight. This is an important observation in that one of the major weaknesses with existing PD animal models is that the acute induction by intracerebral 6-OHDA or systemic MPTP causes abrupt body weight loss and premature death94. While, in most animal models of PD, the effect of direct intervention into NSD system function is characterized by acute, life threatening conditions which wane over time, the human clinical state develops gradually over several decades with body weight loss characteristically occurring only after long term exposure to DA replacement therapy. Therefore, we suggest that the induction of experimental PD through the retina is an approach more closely resembling the clinical state than any other model. The authors further recognize the immensity of the implications of these findings on occupational health and safety parameters governing the use of insecticides, herbicides and other toxins in domestic and agricultural use and in other applications.
It will be important to establish whether the dose of drug introduced into the retina renders its effect upon other brain areas due to diffusion from the site of injection. In the case of 6-OHDA, the effects of this toxin are known to be very localized since it blocks its own reuptake and has a very limited “spread of effect” when injected into the CNS95. Similarly, the injection of toxins such as PARA and ROTE are so small that when injected locally, within the brain, variation in location by only a few micrometers, adjacent to the NSD system, are without effect (compared to those that hit directly on target). This demonstrates the anatomical specificity of our findings and rules out an explanation that these compounds are diffusing from the retina into the brain, more than 20 mm away at a site in another body compartment to render its effect96. That the effects we observed are site specific is consistent with earlier reports demonstrating that minute IVIT doses of the therapeutic drug, L-dopa, can induce recovery from DA depleting lesions of the NSD system in the 6-OHDA rat model of PD72. Although interpretation of results from the rat model of PD cannot always be directly translatable to PD itself, previous work supporting the hypothesis12 suggesting that the anatomy of PD may be extended to include the retina awaits clinical confirmation. If proven to be the case, our understanding of the aetiology of PD and the development of new treatments would change dramatically.
In conclusion, the present work suggests that the eye is the site of exposure from which Parkinsonian symptoms can be produced which closely mimics and the natural course of experimental forms of the disease. It is interesting to note further that not only do PD patients suffer visual deficits, many of which remain occult in routine ophthalmologic practice, but experimental models of PD have been reported to display impaired visual function78,97. Whether it is cerebroventricular or intracerebral injections of 6-OHDA, systemic MPTP or exposure to toxins such as PARA, all have been reported to produce visual impairment in parallel with motor deficits. It is of further interest to note that, while PD has been described traditionally as a disease of DA deficiency of the NSD system, deficits in retinal DA are now accepted as part of the syndrome77. What has escaped critical examination is the absence of a viable explanation as to how the parallel development of retinal DA deficiency is tied to the degenerative process, in the mesencephalon many centimeters away. If retinal DA degeneration is part of the disorder then the key questions become, “…What process causes the retina to become depleted of DA in PD? Is it a humoral process or are the two systems functionally connected so that the degeneration of one is precipitated by its anatomical link to the other?” The present results confirm the importance of elucidating answers to these questions and further exploring the role of the retina in the control of motor performance, particularly in disease states such as PD. Whether the proposed link between the retina and deep brain structures be anatomical12, neurochemical42,72 or neuroendocrinological30 the present findings require further validation in other models and in the clinical syndrome itself. Future research on this theme is driven by the hope of providing better treatment options for a most debilitating disease.
Methods
42 male and female, Sprague Dawley rats were obtained from the Bronowski Institute colony and were housed individually in wire mesh cages with standard food pellets (Clarke King/Barastock) made available ad lib from a feeding grid. Tap water was made available from bottles attached to the front of each cage. Animals ranged in weight from 250 to 350 grams at the commencement of the experiment. Room temperature was maintained at 22°C ± 2° with a 12 hr L/D cycle with lights on at 0700 hrs. The room was illuminated with 2 fluorescent tubes with the intensity of light within each cage averaging 250 Lx during the L phase of the L/D cycle. No light was detected during the D phase. All experiments were approved by the Animal Experimentation Ethics Committee of the Bronowski Institute of Behavioural Neuroscience and monitored implementing protocols conforming to the NH & MRC Guidelines for the Care and Use of Animals for Scientific Purposes.
Study design
After habituation into the colony for at least 7 days all animals were handled by the experimenters involved in the work prior to commencing the formal part of the study.
There were six groups employing 7 animals per group with the animals in each group being body weight match so that they were similar between all three groups at the commencement of the study. Each rat in each of the 3 groups received either an IVIT injection of 6-OHDA, PARA, MPTP ROTE or vehicle (2). The performance of all rats on the tests described below was determined at least 1 week prior to the first IVIT injection and this served as the pre-control values. Rats received an IVIT injection once a week for 6 weeks and then were tested 2 weeks after the last IVIT injection during both the L and D phase of the LD cycle. All animals were injected after the onset of the L phase. Further details of the IVIT injections are described subsequently and the 5 tests of motor function are described below with body weight measured intermittently prior to and during the course of the chronic study.
Drugs and solutions for IVIT injections
6-OHDA was acquired from Sigma-Aldrich, (St. Louis MO. USA) and was mixed in a concentration of 1 μg/μl. 6-OHDA was dissolved in a 1 mg/ml solution of ascorbic solution to prevent rapid oxidation of the drug30,94. This solution was brought to isotonicity by adding NaCl. PARA (methyl viologen dichloride hydrate-95%-Sigma-Aldrich Chemicals, St. Louis. MO., U.S.A.) was dissolved into a concentration of 2.57 μg/μl. MPTP and ROTE were obtained from Sigma Chemical and mixed in the concentrations of 25 μg/μl and 2 μg/μl, respectively. Vehicle injections were made with 2 μl of an isotonic saline/ascorbic acid solution for the 6-OHDA/PARA study while DMSO served as the vehicle in the MPTP/ROTE study. New solutions of drug were prepared immediately prior to injection with stock solutions kept refrigerated or on ice until used. All solutions were kept shielded from light and then discarded immediately at the end of each injection session. All concentrations of drug employed in both studies were chosen on the basis or previous work describing a localised effect of these compounds when injected by the intracerebral route98,99,100,101,102,103 thereby suggesting that the observed effect does not merely represent leakage of test substances into sensitive brain areas.
IVIT injections
Injections into the vitreous humour were made with the aid of a 10 μl syringe fitted with a 26 g needle that was 75 mm in length. The needle was fitted with a coloured plastic sleeve exposing 3 mm of the tip to allow the experimenter to gauge the depth of needle insertion into the centre of the vitreal mass. Rats were first placed in a clear Perspex induction chamber 200 × 300 × 400 mm fitted with a base constructed from heavy gauge plastic netting overlying a 125 mm layer of cotton baton that served to absorb and hold the anaesthetic. Isofluorane inhalation anaesthetic (Attane-Bomac: 1 ml/ml) was employed by placing approximately 2–3 mls onto the absorbable cotton surface just prior to placing the animal into the induction chamber. Exposure of the animal for 60 to 100 seconds induced a state of deep anaesthesia that lasted ≈60–80 seconds thereby permitting the injection of the test substances and vehicle into the vitreous. As a matter of procedure the fur was swabbed with 70% ETOH for cleansing the surrounding area prior to injection. To facilitate injection into the lateral aspect of the eye, light pressure was placed on the medial surface of the eye using a sterile, gloved, tip of the index finger to cause it to become a manoeuvrable exophthalmic mass and thereby permit the surgeon to gently apply counter pressure when the needle was inserted. All substances injected were administered bilaterally in a volume of 2 μl always commencing with the left eye receiving the first injection, as a matter of orderly procedure. When injections were complete, the area was gently swabbed with sterile, isotonic saline and a drop of antibiotic ointment (Amacin eye and ear ointment), was placed on the cornea as a prophylactic. Rats were held and kept warm until they were able to ambulate on their own and then each returned to their individual cage.
Behavioural measures
Independent variables were measured during the L and the D phase of the L/D cycle commencing between the hours of 10:00–1500 h and again at 20:00–01:00 h, respectively, with at least 18 hours allowed between consecutive measurements.
Locomotion and rearing were measured with the aid of a 900 mm (length) × 500 mm (width) × 300 mm (Height) PVC box fitted with machine vision having motion detection capabilities. The total number of movements within the horizontal plane and the number of rearing associated movements in the vertical plane during each 10 min test session were measured and recorded with the aid of specialized software. A series of three motor reflex tests were performed immediately at the conclusion of the open field test30. These tests included the latency to retract the left and right front limbs when they were elevated 25 mm from the table surface, the latency to step up or down from a raised platform when the rear torso was elevated 25 mm and the latency to ambulate outside of a 90 × 170 mm rectangle. These tests are derivations of those described originally by Balagura et al (1969)104 and have been used extensively to characterize experimental PD30,42,94. The test chamber and all surfaces and apparati were thoroughly washed between the testing of each animal to avoid contamination which may cause distraction during testing.
Testing during the D phase of the L/D cycle was performed under low intensity red light with all sources of illumination masked by implementing red barrier filters.
Body weight was measured intermittently commencing at least 5 days prior to the first of the six injections employed for the chronic studies and on day's 7, 14, 21, 28, 35 and 42 during the course of the study. Weights were taken at times usually commencing at about 1000 hrs in both experiments.
Statistical analysis
Data was analyzed with an Omnibus ANOVA for repeated measures design with pair wise post-hoc comparison using LSD. Mauchley's Test of Sphericity was performed and if significant then the more conservative Greenhouse-Geisser coefficient was used for determining the F-value and significance level. If Mauchley's Test of Sphericity was not significant then the F-Value and level of significance were calculated on the basis that Sphericity was assumed. The main effect for within group effects compared pre-IVIT control measures with their own post-IVIT performance while between group effects were determined with post-hoc, paired comparisons made between each toxin and their independent vehicle injected controls. If Mauchley's Test was significant and no significant main effect was observed for any parameter then further post hoc comparisons were carried out between pre and post drug treatment values for each group and for vehicle versus drug treatment groups using The Wilcoxon Signed Rank Test. Exact significance for a 1-tailed test was employed. Significance levels were chosen at 0.05 with a significant trend set at .05 to .06.
References
Romeo, S. et al. Bright light exposure reduces TH-positive dopamine neurons: Implications of light pollution in Parkinson disease epidemiology. Sci. Rep. 3, 1395 (2013).
Marsden, C. D. Pigmentation in the nucleus substantia nigra of mammals. J. Anat. 95, 256–261 (1961).
Issidorides, M. R. Neuronal vascular relationships in the zona compacta from normal and Parkinsonian substantia nigra. Brain Res. 25, 289–299 (1971).
Barbeau, A. Manganese and extrapyramidal disorders: a critical review and tribute to Dr. George C. Cotzias. Neurotoxicology. 5, 13–35 (1984).
Forno, L. S. & Alvord, E. C. Depigmentation in the nerve cells of the substantia nigra and locus coeruleus in Parkinsonism. Adv. Neurol. 5, 195–202 (1974).
Marsden, C. D. Neuromelanin and Parkinson's disease. J. Neural. Transm. 19, 121–141 (1983).
Brooks, D. J. Parkinson's disease: diagnosis. Park. Rel. Disord. 1, 531–533 (2012).
Kashihara, K., Shinya, T. & Higaki, F. Neuromelanin magnetic resonance imagery of nigral volume loss in patients with Parkinson's disease. J. Clin. Neurosci. 18, 1093–1096 (2011).
Lacy, M. E. Neuromelanin: A hypothetical component of bioelectric mechanisms in brain function. Physiol. Chem. & Physics. 3, 319–324 (1981).
Rapp, L. M. & Smith, S. C. Evidence against melanin as the mediator of retinal photo-toxicity by short wavelength Light. Exp. Eye Res. 54, 55–62 (1992).
Fasano, M., Giraudo, S., Coha, S., Berganasco, B. & Lopiano, L. Residual substantia nigra neuromelanin in Parkinson's disease is cross-linked to alpha-synuclein. Neurochem. Int. 42, 603–606 (2003).
Willis, G. L. Parkinson disease as a neuroendocrine disorder of circadian function: dopamine-melatonin imbalance and the visual system in the genesis and progression of the degenerative process. Rev. Neurosci. 19, 245–316 (2008).
Zucca, F. A. et al. The neuromelanin of human substantia nigra: physiological and pathological aspects. Pigment Cell Res. 17, 610–617 (2004).
Double, K. L. Functional effects of neuromelanin in model systems. J. Neurochem. Transm. 113, 751–776 (2006).
Dubocovich, M. L. Melatonin as a potent modulator of dopamine release in the retina. Nature (Lond.) 306, 782 (1983).
Megan, P. L., Boelen, M. G., Morgan, I. G. & Boelen, M. K. Diurnal patterns of dopamine release in the chicken retina. Neurochem. Int. 48, 17–23 (2006).
Pozdeyen, N. V. & Laurikova, E. V. Diurnal changes of tyrosine, dopamine and dopamine metabolite content in the retina of rats maintained at different lighting conditions. J. Mol. Neurosci. 15, 1–9 (2000).
Lerner, A. B., Case, J. D., Takahaski, K., Lee, T. H. & Mori, W. Isolation of melatonin, The pineal gland factor that lightens melanocytes. J. Am. Chem. Soc. 80, 2587 (1958).
Dubocovich, M. L. Role of melatonin in the retina. Prog. Ret. Res. 8, 129–151 (1989).
Willis, G. L. & Turner, E. J. D. Primary and secondary features in Parkinson's disease improves with strategic exposure to bright light: a case series study. Chronobiol. Int. 24, 521–537 (2007).
Artemenko, A. R. & Levin, Y. I. The phototherapy of patients with Parkinsonism. Zh. Neuropatol. Psikhiatr. Int. S. S. Korsakova. 96, 63–66 (1996).
Willis, G. L., Moore, C. & Armstrong, S. M. A historical Justification for and retrospective analysis of the systematic application of light therapy in Parkinson's disease. Rev. Neurosci. 23, 199–226 (2012).
Paus, S. et al. Bright light therapy in Parkinson disease: a pilot study. Mov. Disord. 22, 1495–1498 (2007).
Bertolucci, P. H., Andrade, L. A., Lima, J. G. & Carlini, E. A. Total sleep deprivation and Parkinson's disease. Arg. Neuropsiquiatr. 45, 224–230 (1987).
Reist, C., Sokolski, K. N., Chen, C. C., Coskinas, E. & Demet, E. M. The effects of sleep deprivation on motor impairment and retinal adaptation in Parkinson's disease. Prog. Neuro-Psychopharmacol. Biol. Psychiatr. 19, 445–454 (1995).
Demet, E. M., Chicz-Demet, A., Fallon, J. H. & Sokolski, K. N. Sleep deprivation Therapy in depressive illnesses and Parkinson's disease. Prog. Neuropsychopharmacol. Biol. Psych. 23, 753–784 (1999).
Larsen, J. K., Lindberg, M. L. & Skovgarrd, B. Sleep deprivation as a treatment for endogenous depression. Acta. Psychiatr. Scand. 54, 167–173 (1976).
Danguir, J. & Nicolaidis, S. Cortical activity and sleep in the rat lateral hypothalamic syndrome. Brain Res. 185, 305–321 (1980).
Burton, S., Daya, S. & Potgeiter, B. Melatonin modulates apomorphine- induced rotational behaviour. Experientia. 47, 466–469 (1991).
Willis, G. L. & Armstrong, S. M. A Therapeutic role for melatonin antagonism in experimental models of Parkinson's disease. Physiol. Behav. 66, 785–789 (1999).
Rutten, S. et al. Bright Light Therapy in Parkinson's disease: an overview of the background and evidence. Parkinson's disease. 2012: 767105, 1–9 (2012).
Noell, W. K., Walker, V. S., Kang, B. S. & Bernan, S. Retinal damage by light in rodents. Invest. Ophthalmol. 5, 450–473 (1966).
Olafson, R. P. & O'Steen, W. K. Hormonal influences on photoreceptor damage: The pituitary gland and ovaries. Invest. Opthalmol. 15, 869–872 (1976).
Duncan, T. E. & O'Steen, W. K. The diurnal susceptibility of rat retinal photoreceptors to light- induced damage. Exp. Eye Res. 41, 497–507 (1985).
Grignulo, A., Orzalesi, N., Costrllazzo, R. & Vittone, P. Retinal damage by visible light in albino rats: an electron microscopy study. Ophthalmologica. 157, 43 (1969).
O'Steen, W. K. & Donnelly, J. E. Chronic analysis and variations in retinal damage in two strain of rats after short term illumination. Invest. Ophthalmol. 22, 252–255 (1982).
Ham, W. T., Jr, Mueller, H. A., Ruffalo, J. J. & Clarke, A. M. Sensitivity of the retina to radiation damage as a function of wavelength. Photochem. Photobiol. 29, 735–743 (1979).
Hochheimer, B. F., D'Anna, S. A. & Calkins, J. L. Retinal damage from light. Am. J. Ophthalmol. 88, 1039–1044 (1979).
Oraedu, A. C., Voaden, M. J. & Marshall, J. Photochemical damage in the albino rat retina: morphological changes and endogenous amino acids. J. Neurochem. 35, 1361–1369 (1980).
Rapp, L. M. & Williams, T. P. Damage to the albino rat retina produced by low intensity light. Photochem. Photobiol. 29, 731–733 (1979).
Rapp, L. M. & Williams, T. P. The role of ocular pigmentation in protecting against retinal light damage. Vis. Res. 20, 1127–1131 (1980).
Willis, G. L., Kelly, A. M. A. & Kennedy, G. A. Compromised circadian function in Parkinson's disease: enucleation augments disease sensitivity in the unilateral model. Behav. Brain. Res. 193, 37–47 (2008).
Humpel, C. et al. Effects of bright, artificial light on monoamines and neuropeptides in eight different brain regions compared in a pigmented and non-pigmented rat strain. J. Neurosci. Res. 32, 605–612 (1997).
White, M. P. & Fisher, L. J. Degree of light damage to the retina varies with time of day of bright light exposure. Physiol. Behav. 39, 607–13 (1997).
Tanito, M., Kaidzu, S., Ohira, A. & Anderson, R. E. Topography of retinal damage in light exposed albino rats. Exp. Eye Res. 87, 292–295 (2008).
Sanyal, S. & Hawkins, R. K. Development and degeneration of retina in rds mutant mice: effects of light on the rate of degeneration albino and pigmented homozygous and heterozygous mutant and normal mice. Vision Res. 28, 1177–1185 (1986).
Sang, A. et al. Light-induced retinal ganglion cell damage in vivo involves Dexras1. Mol. Vis. 17, 134–143 (2011).
Roberts, J. E. Screening for ocular photoxicity. Int. J. Toxicol. 21, 491–500 (2002).
Scwwartz, M. D. et al. Dissociation of circadian and light inhibition of melatonin release through forced desynchronization in the rat. Proc. Nat. Acad. Sci. (U.S.A.) 106, 17540–5 (2009).
Chen, R., Seo, D. O., Bell, E., von Gall, C. & Lee, C. Strong resetting of the mammalian clock by constant light followed by constant darkness. J. Neurosci. 28, 11839–47 (2008).
Foley, j. M. & Baxter, D. On the nature of pigment granules in the cells of the locus coeruleus and substantia nigra. J. Neuropath. Exp. Neural. 17, 586–598 (1958).
Graham, D. G. On the origin and significance of neuromelanin. Arch. Pathol. Lab. Med. 103, 359–362 (1979).
McGeer, P. L., McGeer, E. G. & Suzuki, J. S. Aging and extrapyramidal function. Arch. Neurol. 34, 33–35 (1977).
McGeer, P. L. & McGeer, E. G. Aging and neurotransmitter systems. Adv. Exp. Med. Biol. 113, 41–57 (1978).
Jobsis, F. F. Non-invasive infrared monitoring of cerebral and myocardial oxygen sufficiency and circulatory parameters. Science. 198, 1264–1267 (1977).
Haeussinger, F. B. et al. Simulation of near-infrared light absorption considering individual head and prefrontal cortex anatomy: implications for optical neuroimaging. Plos. One. 6, 1–12 (2011).
Wernsperger, N., Sylvia, A. L. & Jobsis, F. F. Incomplete transient Ischemia: a non-destructive evaluation of in vivo cerebral metabolism and hemodynamics in rat brain. Stroke. 12, 864–868 (1981).
Wolf, M., Ferrari, M. & Quaresima, V. Progress of near-infrared spectroscopy and topography for brain and muscle clinical applications. J. Biomed. Opt. 12, 062104 (2007).
Piantadosi, C. A. Early development of near-infrared Spectroscopy at Duke University. J. Biomed. Opt. 12, 062102 (2007).
Colier, W. N., Van Haaren, N. J. & Oeseberg, B. A comparative study of two near-infrared spectrophotometers for the assessment of cerebral hemodynamics. Acta. Anaesthesiol. Scand. Suppl. 102, 101–105 (1995).
Obrig, H. & Villringer . Beyond the visible- imaging the human brain with light. J. Cereb. Blood Flow Metab. 23, 1–18 (2003).
Trimmer, P. A. et al. Reduced Axonal Transport in Parkinson's disease cybrid neurites is restored by light therapy. Mol. Neurodegen. 4, 1750–1751 (2009).
Van Brunt, E. E., Shepard, M. D., Wall, J. R., Ganong, W. F. & Clegg, M. T. Penetration of light into the brain of mammals. Ann. N. Y. Acad. Sci. 117, 217–224 (1964).
Rocha, F. L., Murad, M. G., Stumpf, B. P., Hara, C. & Fuzikawa, C. Antidepressants for depression in Parkinson's disease: systematic review and meta-analysis. J. Psychopharmacol. 27, 417–423 (2013).
Yamamshi, T. et al. Anxiety and depression in patients with Parkinson's disease. Int. Med. 52, 539–545 (2013).
Mass, A. & Reichmann, H. Sleep and non-motor symptoms in Parkinson's disease. J. Neurol. Transm. 4, 565–569 (2013).
Gerbaldo, H., Cassady, S., Mauver, K. & Pleschl, D. The assessment of light Intensity preference in psychiatric patients: A questionnaire. Acta. Psychiatr. Scand. 95, 236–241 (1997).
Wink, B. & Harris, J. A model of the Parkinsonian visual system: support for the dark adaptation hypothesis. Vision Res. 40, 1937–46 (2000).
Kayser-Jones, K. The environment and quality of care in long-term care institutions. WLN Publ. 20–2292, 87–107 (1982).
Hiatt, L. G. Is poor Light dimming the sight of nursing home patients? Nurs. Homes. 29, 32–41 (1980).
Ouslander, J. G. et al. A non-pharmacological intervention to improve sleep in nursing home patients: results of a controlled clinical trial. J. Am. Geriatr. Soc. 54, 38–47 (2006).
Willis, G. L. Intraocular microinjections repair experimental Parkinson's disease. Brain Res. 1217, 119–131 (2008).
Shinde, V. M., Sizova, O. S., Lin, J. H., La Vail, M. M. & Gorbatyuk, M. S. ER Stress in retinal degeneration in S334ter Rho rats. PloS One. 7, e33266 (2012).
Cingulani, C. et al. Retinal degeneration from oxidative damage. Free Radic. Bio. Med. 40, 660–669 (2006).
Rojas, J. C., John, J. M., Lee, J. & Gonzalez-Lima, F. Methyl blue provides behavioural and metabolic neuroprotection against optic neuropathy. Neurotox. Res. 15, 260–273 (1988).
Yew, D. T., Li, W. W., Zhang, D. R. & Luo, Z. B. Metabolic and phagocytic activities of the mouse retina after 6-hydroxydopamine treatment. Acta Anat. (Basal) 133, 27–29 (1988).
Adam, C. R., Shrier, E., Ding, Y., Glazman, S. & Bodis-Wollner, I. Correlation of inner retinal thickness evaluated by spectral-domain optical coherence tomography and contrast sensitivity in Parkinson's disease. J. Neuroopthalmol. 33, 137–142 (2013).
Bodis-Wollner, I. & Tzelepi, A. The push-pull action of dopamine and spatial tuning of the monkey retina: the effects of dopaminergic deficiencies and selective D1 and D2 receptor ligands in the pattern electroencephalogram. Vision Res. 38, 1479–1481 (1998).
Bodis-Wollner, I. The visual system in Parkinson's disease. IN: Vision and the brain. Chohen, B. & Bodis-Wollner, I. eds. 299–314 (Raven Press, New York, 1990).
Archibald, N. K., Clarke, M. P., Mosimann, V. P. & Burn, D. J. The retina in Parkinson's disease. Brain. 132, 1128–1145 (2009).
Willis, G. L. The therapeutic effects of dopamine replacement therapy and it's psychiatric side effects are mediated by the pineal function. Behav. Brain Res. 160, 148–160 (2005).
Djamgoz, M. B. A., Hankins, M. W., Hirano, J. & Archer, S. N. Neurobiology of retinal dopamine in relation to degenerative states of the tissue. Vis. Res. 37, 3509–3529 (1991).
Nicolaus, B. J. A critical review of the function of neuromelanin in an attempt to provide a unified theory. Med. Hypoth. 65, 791–796 (2005).
Tapias, V., Cannan, J. R. & Greenamyre, J. T. Melatonin treatment potentiates neurodegeneration in a rat rotenone Parkinson's disease model. J. Neurosci. Res. 88, 420–427 (2010).
Sleipness, E. P., Sorg, B. A. & Jansen, H. T. Diurnal differences in dopamine transporter and tyrosine hydroxylase levels in rat brain: dependence on the superchiasmatic nucleus. Brain Res. 1129, 34–42 (2007).
Hampp, G. & Ulbrecht, U. The circadian clock and mood-related behaviour. Commun. Integr. Biol. 1, 1–3 (2008).
Boulamery, A., Simon, N., Vidal, J. & Brugerolle, B. Effects of L-dopa on circadian rhythms of 6-OHDA striatal lesioned rats: a radiotelemetric study. Chronobiol. Int. 27, 251–264 (2010).
Djeridane, Y. Pineal systems of the desert rodents and its relationship to the epithalamus. Anat. Histo. Embryol. 37, 323–23 (2008).
Hu, D. N., Simon, J. D. & Sarna, J. Role of ocular melanin in ophthalmic physiology and pathology. Photochem. Photobiol. 84, 639–44 (2008).
Ari, S., Caca, I. & Kayabasi, H. Bilateral complete optic atrophy and haemorrhagic infarction of the putamen caused by methanol intoxication. Ann. Opthalmol. 39, 249–252 (1971).
Airas, L., Paaviloinen, T., Marttila, R. J. & Rinne, J. Methanol intoxication induced nigrostriatal dysfunction detected using – [18F] Floro-L-Dopa-Pet. Neurotoxicol. 4, 671–674 (2008).
Racette, B. A. et al. Increased risk of Parkinsonism associated with welding exposure. Neurotoxicol. 33, 1356–1361 (2012).
Lolekha, P., Phanthumchinda, K. & Bhidayasiri, R. Prevalence and risk factors of Parkinson's disease in retired Thai traditional boxers. Mov. Disord. 25, 1895–1901 (2010).
Areno, O., Aral, H., Reim, M. & Wenzel, M. Welders maculopathy despite using protective lenses. Retina. 16, 257–259 (1996).
Corrales, G. & Curreri, A. Eye trauma in boxing. Clin. Sports Med. 28, 591–607 (2009).
McCormac, A. L. et al. Environmental risk factors and Parkinson's disease: Selective degeneration of nigral dopaminergic neurons caused by the herbicide paraquat. Neurobiol. Dis. 10, 119–122 (2002).
Pojma, S. M. & Brus, R. The effect of central chemical sympathectomy on the oxygen uptake, anaerobic glycolysis and lactic acid dehydrogenase activity in the retina of white rats. Albrecht von Graef Arch. Klin. Exp. Opthalmol. 200, 223–226 (1976).
Chui, Y. C., Poon, G. & Law, F. Toxicokinetics and bioavailability of paraquat in rats following different rates of administration. Toxicol. Ind. Health. 4, 203–219 (1988).
Bartlett, R. M. et al. Paraquat is excluded by the blood brain barrier in rhesus macaque: an in vivo pet study. Brain Res. 1259, 74–79 (2009).
Nagao, M. et al. Immunohistochemical localization of paraquat in skin and eye of the rat. Nihon Hoigaku Zasshi. 47, 202–206 (1993).
Willis, G. L. The role of ML-23 and other melatonin analogues in the treatment and management of Parkinson's disease. Drug News Perspect. 18, 437–444 (2005).
Willis, G. L., Singer, G. & Evans, B. K. Intracranial injections of 6-OHDA: comparison of catecholamine-depleting effects of different volumes and concentrations. Pharmac. Biochem. Behav. 15, 207–213 (1976).
Saravanan, K. S., Sindhu, K. M. & Mohanakumar, K. P. Acute intranigral infusion of rotenone in rats causes progressive biochemical lesions in the striatum similar to Parkinson's disease. Brain Res. 1049, 147–155 (2005).
Balagura, S., Wilcox, R. H. & Coscina, D. V. The effects of diencephalic lesions on food intake and motor activity. Physiol. Behav. 4, 629–633 (1969).
Hattar, S. et al. Central projections of melanopsin-expressing retinal ganglion cells in the mouse. J. Comp. Neurol. 497, 326–349 (2006).
Acknowledgements
The authors would like to acknowledge the technical assistance of Mrs. Monica Dumitrescu and to Mr. Alan Williams.
Author information
Authors and Affiliations
Contributions
G.L.W. and S.M.A. wrote the main manuscript and C.M. prepared figures and tables, provided technical support and assisted in manuscript preparation.
Ethics declarations
Competing interests
The authors declare no competing financial interests.
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/3.0/
About this article
Cite this article
Willis, G., Moore, C. & Armstrong, S. Parkinson's Disease, Lights and Melanocytes: Looking Beyond the Retina. Sci Rep 4, 3921 (2014). https://doi.org/10.1038/srep03921
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep03921
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
