
Abstract
Despite the success of monotherapies based on blockade of programmed cell death 1 (PD-1) in human melanoma, most patients do not experience durable clinical benefit. Pre-existing T-cell infiltration and/or the presence of PD-L1 in tumours may be used as indicators of clinical response; however, blood-based profiling to understand the mechanisms of PD-1 blockade has not been widely explored. Here we use immune profiling of peripheral blood from patients with stage IV melanoma before and after treatment with the PD-1-targeting antibody pembrolizumab and identify pharmacodynamic changes in circulating exhausted-phenotype CD8 T cells (Tex cells). Most of the patients demonstrated an immunological response to pembrolizumab. Clinical failure in many patients was not solely due to an inability to induce immune reinvigoration, but rather resulted from an imbalance between T-cell reinvigoration and tumour burden. The magnitude of reinvigoration of circulating Tex cells determined in relation to pretreatment tumour burden correlated with clinical response. By focused profiling of a mechanistically relevant circulating T-cell subpopulation calibrated to pretreatment disease burden, we identify a clinically accessible potential on-treatment predictor of response to PD-1 blockade.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$29.99 / 30 days
cancel any time
Subscribe to this journal
Receive 51 print issues and online access
$199.00 per year
only $3.90 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout




Similar content being viewed by others


Change history
27 April 2017
In Fig. 1c the x-axis label for the bottom bar graph was corrected.
References
Topalian, S. L., Taube, J. M., Anders, R. A. & Pardoll, D. M. Mechanism-driven biomarkers to guide immune checkpoint blockade in cancer therapy. Nat. Rev. Cancer 16, 275–287 (2016)
Fridman, W. H., Pagès, F., Sautès-Fridman, C. & Galon, J. The immune contexture in human tumours: impact on clinical outcome. Nat. Rev. Cancer 12, 298–306 (2012)
Herbst, R. S. et al. Predictive correlates of response to the anti-PD-L1 antibody MPDL3280A in cancer patients. Nature 515, 563–567 (2014)
Tumeh, P. C. et al. PD-1 blockade induces responses by inhibiting adaptive immune resistance. Nature 515, 568–571 (2014)
Pauken, K. E. & Wherry, E. J. Overcoming T cell exhaustion in infection and cancer. Trends Immunol. 36, 265–276 (2015)
Barber, D. L. et al. Restoring function in exhausted CD8 T cells during chronic viral infection. Nature 439, 682–687 (2006)
Topalian, S. L., Drake, C. G. & Pardoll, D. M. Immune checkpoint blockade: a common denominator approach to cancer therapy. Cancer Cell 27, 450–461 (2015)
Robert, C. et al. Pembrolizumab versus ipilimumab in advanced melanoma. N. Engl. J. Med. 372, 2521–2532 (2015)
Ribas, A. et al. Pembrolizumab versus investigator-choice chemotherapy for ipilimumab-refractory melanoma (KEYNOTE-002): a randomised, controlled, phase 2 trial. Lancet Oncol. 16, 908–918 (2015)
Blackburn, S. D. et al. Coregulation of CD8+ T cell exhaustion by multiple inhibitory receptors during chronic viral infection. Nat. Immunol. 10, 29–37 (2009)
Twyman-Saint Victor, C. et al. Radiation and dual checkpoint blockade activate non-redundant immune mechanisms in cancer. Nature 520, 373–377 (2015)
Brahmer, J. R. et al. Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: safety, clinical activity, pharmacodynamics, and immunologic correlates. J. Clin. Oncol. 28, 3167–3175 (2010)
Paley, M. A. et al. Progenitor and terminal subsets of CD8+ T cells cooperate to contain chronic viral infection. Science 338, 1220–1225 (2012)
Im, S. J. et al. Defining CD8+ T cells that provide the proliferative burst after PD-1 therapy. Nature 537, 417–421 (2016)
He, R. et al. Follicular CXCR5-expressing CD8+ T cells curtail chronic viral infection. Nature 537, 412–416 (2016)
Bengsch, B. et al. Coexpression of PD-1, 2B4, CD160 and KLRG1 on exhausted HCV-specific CD8+ T cells is linked to antigen recognition and T cell differentiation. PLoS Pathog. 6, e1000947 (2010)
Duraiswamy, J. et al. Phenotype, function, and gene expression profiles of programmed death-1hi CD8 T cells in healthy human adults. J. Immunol. 186, 4200–4212 (2011)
Gupta, P. K. et al. CD39 expression identifies terminally exhausted CD8+ T cells. PLoS Pathog. 11, e1005177 (2015)
Pauken, K. E. et al. Epigenetic stability of exhausted T cells limits durability of reinvigoration by PD-1 blockade. Science 354, 1160–1165 (2016)
Gros, A. et al. Prospective identification of neoantigen-specific lymphocytes in the peripheral blood of melanoma patients. Nat. Med. 22, 433–438 (2016)
Miller, J. D. et al. Human effector and memory CD8+ T cell responses to smallpox and yellow fever vaccines. Immunity 28, 710–722 (2008)
Wherry, E. J., Blattman, J. N., Murali-Krishna, K., van der Most, R. & Ahmed, R. Viral persistence alters CD8 T-cell immunodominance and tissue distribution and results in distinct stages of functional impairment. J. Virol. 77, 4911–4927 (2003)
Wilmott, J. S. et al. Selective BRAF inhibitors induce marked T-cell infiltration into human metastatic melanoma. Clin. Cancer Res. 18, 1386–1394 (2012)
Knight, D. A. et al. Host immunity contributes to the anti-melanoma activity of BRAF inhibitors. J. Clin. Invest. 123, 1371–1381 (2013)
Balch, C. M. et al. Final version of 2009 AJCC melanoma staging and classification. J. Clin. Oncol. 27, 6199–6206 (2009)
Rizvi, N. A. et al. Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science 348, 124–128 (2015)
Sharma, P. & Allison, J. P. Immune checkpoint targeting in cancer therapy: toward combination strategies with curative potential. Cell 161, 205–214 (2015)
Smyth, M. J., Ngiow, S. F., Ribas, A. & Teng, M. W. Combination cancer immunotherapies tailored to the tumour microenvironment. Nat. Rev. Clin. Oncol. 13, 143–158 (2016)
Nishino, M. et al. Developing a common language for tumor response to immunotherapy: immune-related response criteria using unidimensional measurements. Clin. Cancer Res. 19, 3936–3943 (2013)
Wolchok, J. D. et al. Guidelines for the evaluation of immune therapy activity in solid tumors: immune-related response criteria. Clin. Cancer Res. 15, 7412–7420 (2009)
Breiman, L. Random Forests. Mach. Learn. 45, 5–32 (2001)
Qiu, P. et al. Extracting a cellular hierarchy from high-dimensional cytometry data with SPADE. Nat. Biotechnol. 29, 886–891 (2011)
Acknowledgements
We thank all the patients who contributed to this study. We thank all of the members of the Wherry laboratory for their contributions. This study was funded in part by NIH Grants R01 AI105343, P01 AI108545, U19 AI082630, and U19 AI117950 (E.J.W.); T32 2T32CA009615-26 (A.C.H.), P30-CA016520 (R.M.), P50-CA174523 (L.M.S., T.C.G, R.K.A., G.C.K., X.X., K.L.N., R.M., R.H.V.), P01CA114046 (X.X., R.K.A.), P30 CA008748 (K.S.P., D.K., J.D.W.), P01 CA114046 (K.L.N.), K08 AI114852 (R.S.H.), T32CA009140 (J.R.G.), Tara Miller Foundation (L.M.S., R.K.A., G.C.K., T.C.G., R.H.V., X.X.), German Research Foundation fellowship BE5496/1-1 (B.B.), Penn Department of Medicine Measey Research Fellowship Award (A.C.H.), NCATS KL2TR001879 (R.J.O.), Melanoma Research Alliance (K.L.N.), Robertson Foundation/Cancer Research Institute Irvington Fellowship (K.E.P.), Ludwig Center for Cancer Immunotherapy (P.W., M.A., J.D.W.), Swim Across America (J.D.W.), Conquer Cancer Foundation (M.A.P.), and funding from the Parker Institute for Cancer Immunotherapy (R.M., J.D.W., R.H.V., E.J.W.).
Author information
Authors and Affiliations
Contributions
A.C.H. and E.J.W. conceived and designed the overall studies. A.C.H. and T.C.G. designed and implemented the clinical trial at Penn and T.C.G. was principal investigator of this clinical trial. M.A.P., M.A., D.K., C.C., P.W. and J.D.W. designed, executed and performed immune assessment on the MSKCC trial and M.A.P. was principal investigator of this clinical trial. A.C.H. performed immune assessment assays with R.J.O., B.B., J.R.G., F.Q., K.E.P., R.S.H., R.P.S., S.K., J.M.S., and S.M.G. R.M. and K.S.P. performed biostatistical analyses. S.M. and J.R.G. performed computational analyses of immune profiling and RNA-seq. B.We., B.Wu., K.D’A. and K.L.N. performed mutational analysis and neoepitope prediction. W.X., S.H., and S.M. assisted in the Penn clinical trial. R.K.A., G.C.K. and L.M.S. were investigators on the trial. X.X. evaluated pathological biomarkers. A.C.H., R.H.V., T.C.G. and E.J.W. interpreted the data. A.C.H. and E.J.W. wrote the manuscript, and M.A.P., R.M., T.C.G. edited the manuscript. E.J.W. designed, interpreted, and oversaw the study.
Corresponding authors
Ethics declarations
Competing interests
M.A.P. receives honoraria and/or research support from BMS, Merck, Novartis, Array, Infinity, and RGenix. J.D.W. receives honoraria and/or research support from Merck, BMS, and Genentech. T.C.G. receives honoraria and/or research support from BMS, Novartis, Merck, Incyte, and Roche. R.J.O. has anticipated employment at Merck. E.J.W. receives honoraria and/or research support from BMS, Merck, MedImmune, Surface Oncology, Takeda, and KyMab. E.J.W. has a patent licensing agreement for the PD-1 pathway.
Additional information
Reviewer Information Nature thanks A. Alizadeh, V. Boussiotis and T. Tueting for their contribution to the peer review of this work.
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data figures and tables
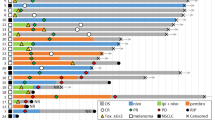
Extended Data Figure 1 Clinical characteristics, response data, and immune data for cohorts analysed.
a, Penn pembro Expanded Access Program (left) and MSKCC Keynote-001 trial (right) that were included in analysis. b, Immune and clinical data from analysed patients in Penn cohort stratified by fold change Ki67 greater or less than 2.2 (blue, responder; red, non-responder).
Extended Data Figure 2 CD4+FOXP3−, CD4+FOXP3+ and CD8 T cells from patients with melanoma have increased Ki67 expression compared to healthy donors.
a, Frequency and Ki67 expression in FOXP3+ CD4 T cells in healthy donors and melanoma patients. Student’s t-test. b, Ki67 expression in CD8 T cells between healthy donors and melanoma patients. Mann–Whitney U-test. c, Ki67 expression in PD-1+ and PD-1− CD8 T cells in healthy donors and patients with melanoma. Healthy donors versus patients, Mann–Whitney U-test; PD-1+ versus PD-1− CD8 T cells in patients with melanoma, Wilcoxon matched-pairs test. d, Ki67 expression in FOXP3− CD4 T cells and FOXP3+ CD4 cells over time. Wilcoxon matched-pairs test. e, Scatter plot of Ki67 expression in PD-1+CD4+FOXP3− T cells versus tumour burden by PFS. f, Ki67 expression in PD-1+CD4+FOXP3+ cells versus tumour burden by PFS (pretreatment, n = 29; post-treatment, n = 27 (e, f)). For all panels, **P < 0.01, ****P < 0.0001. Error bars denote s.d. Flow cytometry data in all panels are representative of 1–4 independent technical replicates of the stain indicated.
Extended Data Figure 3 PD-1 detected after therapy using anti-human IgG4 and proliferating CD8 T cells in healthy donors.
a, Healthy donor PBMCs were incubated with anti-PD-1 clone EH12 BV421 and/or pembro—alone, together or sequentially followed by anti-human IgG4–phycoerythrin. b, Plots of Eomes, T-bet, CD45RA, and CD27 expression in Ki67+ CD8 T cells from a representative healthy donor. c, Comparison of Eomes versus T-bet and CD45RA versus CD27 phenotypes in patients with melanoma and healthy donors (melanoma, n = 25; healthy donor, n = 10). **P < 0.01, Student’s t-test. d, Mean fold change of Ki67 on PD-1+ CD8 T cells over 3 weeks in healthy donors (n = 7). Error bars denote s.d.; centre line denotes mean; dotted line denotes fold change of 2.21, which is equal to the mean + 3 s.d. Flow cytometry data in all panels are representative of 1–2 independent technical replicates of the stain indicated.
Extended Data Figure 4 Effect of anti-CTLA-4 therapy on Ki67 expression is restricted to the pretreatment time point.
a, Correlation of the percentage of PD-1+ CD8 T cells expressing Ki67 to months since last dose of anti-CTLA-4 (pretreatment, n = 26; week 3, n = 25). b, Correlation of the percentage of CTLA-4 in CD8 T cells and months since last dose of anti-CTLA-4 (pretreatment, n = 26; week 3, n = 25). c, Correlation of clinical parameters such as PFS, overall survival (OS), tumour burden, and Ki67 to tumour burden ratio with months since last dose of anti-CTLA-4 (pretreatment, n = 23; week 3, n = 22). r and P values, Pearson’s correlations.
Extended Data Figure 5 CD8 T cells with multiple inhibitory receptors and PD-1+CXCR5+ CD8 T cells are reinvigorated by anti-PD-1 therapy.
a, Ki67 expression in CD8 T cells with multiple inhibitory receptors over time. Week 0 versus week 3 (n = 27). Wilcoxon matched-pairs test. b, Percentage of CD8 T cells positive for PD-1 during pembro treatment (n = 27), Wilcoxon matched-pairs test. c, Back-gating of TEMRA and naive CD8 T-cell populations onto CD45RA versus TCF-1 (right). d, TCF-1 expression in PD-1+CXCR5+ CD8 T cells in blood at week 3 (n = 11). Paired t-test. e, Eomes/T-bet (red) and Eomes/TCF-1 (green) expression in PD-1+CXCR5+ (left) and PD-1+CTLA-4+ (right) subsets. f, Ki67 expression in PD-1+CTLA-4+ and PD-1+CXCR5+ CD8 T cells over time (left) and fold change of Ki67 in PD-1+CXCR5+ and PD-1+CTLA-4+ subsets (right) (n = 11). Wilcoxon matched-pairs test. g, IFNγ production by PD-1+CXCR5+ and PD-1+CTLA-4+ subsets over time; paired t-test. For all panels, *P < 0.05, **P < 0.01, ***P < 0.001, ****P < 0.0001. Error bars denote s.d. CXCR5 and TCF-1 stain is representative of one technical replicate. All other flow cytometry data are representative of 1–4 independent technical replicates of the stain indicated.
Extended Data Figure 6 Conventional differentiation state and clusters of Tex cells can be identified using CyTOF and high-dimensional visualization.
a–c, SPADE analysis applied to blood samples from patients with melanoma and analysed by CyTOF. a, SPADE tree showing MMI of CD27 (left) and CCR7 (right) (representative of 4 patients). b, SPADE tree coloured by median intensities of fold change frequency (left), and Ki67 expression (middle and right) before treatment and at 3 weeks. c, Fold change frequency (left) and MMI of Ki67 (right) of Tex, Tmem, and Teff subsets. d, Frequency of Tex cluster in PD-1+ CD8 T cells over time. e, SPADE tree coloured by MMI of Eomes (left) and CD39 (right) expression at 3 weeks (n = 4). f, MMI of Eomes (left) and CD39 (right) of Tex, Tmem, and Teff subsets. g, Percentage of cells in Tex cluster (left) and Teff cluster (right) in PD-1+ CD8 T cells over time based on CyTOF and SPADE analysis. h, Frequency of Tex versus tumour burden coloured by response. Mass cytometry data in all panels are representative of one technical replicate. MMI shown in this figure represents arcsinh transformed data.
Extended Data Figure 7 RNA-seq of CD8 T cells reveals molecular pathways correlating with reinvigoration.
a–d, RNA-seq was performed on total purified CD8 T cells from three patients at weeks 0, 3, 9, 12. a, Volcano plot of genes altered at 3 weeks compared to pretreatment. Volcano plot constructed using log2 fold changes and their P values of all genes. b, Pathways identified by gene ontology analysis that were altered at week 3 compared to pretreatment using top 50 differentially expressed genes (all genes with fold change >1.5 and P < 0.05). c, Correlation coefficients to Ki67 were used to generate a correlation network. Nodes coloured by strength of correlation to Ki67 (Pearson r = 1 (red), −1 (blue)); node size indicates degree of connectivity. d, Pathways identified by gene ontology analysis using top 100 correlated genes with Ki67 (positive and negatively correlated genes with correlation coefficients >0.67 and <−0.67). RNA sequencing data in all panels are representative of one technical replicate.
Extended Data Figure 8 HLA-DR and CD38 expression enriches for responding Ki67+ cells and TCR clones found in top 100 clones in tumour identified in blood.
a, TCR clones present at pretreatment and post-treatment that are also in the top 100 clones in the tumour. Clones that are among the top 10 in the peripheral blood post treatment highlighted in red. Patient 14–784 did not have an available pretreatment sample and was not included. b, Percentage of CD8 T cells that are Ki67+ (red) and HLA-DR+CD38+ (blue) over time. c, Representative plot of Ki67 expression in HLA-DR+CD38+ CD8 T cells and CD8 T cells that were not CD38+HLA-DR+ (that is, CD38−HLA-DR−, CD38+HLA-DR−, and CD38−HLA-DR+). d, Representative plot of HLA-DR and CD38 expression on Ki67+ and Ki67− CD8 T cells. e, Representative plot of Eomes versus T-bet and PD-1 versus CTLA-4 in HLA-DR+CD38+ (‘DR+38+’) CD8 T-cell subsets and cells that were not CD38+HLA-DR+. f, Percentage of EomeshiT-betlo, PD-1, CTLA-4 and expression on CD8 T cells (n = 5). TCR sequencing and flow cytometry data in all panels are representative of one technical replicate.
Extended Data Figure 9 High Ki67 to tumour burden ratio correlates with improved clinical outcomes and model selection identifies BRAF and lactate dehydrogenase as correlates to Ki67.
a, Scatter plot of maximum fold change of Ki67 expression after treatment versus tumour burden stratified by PFS (n = 23). b, Maximum post-treatment Ki67 expression versus tumour burden by response (n = 23). c, Ki67 expression to tumour burden ratio stratified by landmark PFS (PFS starting from 6 weeks into therapy) (left; n = 23). Kaplan–Meier analysis stratified by a Ki67 to tumour burden ratio of 1.94 (right; Ki67 to tumour burden ratio: high, n = 13; low, n = 10); log-rank test. d, Baysean Information Criteria (BIC), used as a criterion for selection of multiple regression models that best predicted Ki67 (low BIC score produces a stronger model). e, Percentage of Ki67 expression in CD8 T cells (left) and tumour burden (right) stratified by BRAF status. All BRAF+ patients had been treated with BRAF-targeted therapy (n = 4, after removal of patients with unmeasurable tumour burden); Mann–Whitney U-test. f, Correlation of percentage Ki67+ versus lactate dehydrogenase (LDH) (left) and tumour burden versus LDH (right); Pearson’s correlation. g, Ki67 to LDH ratio stratified by landmark overall survival (overall survival starting from 6 weeks into therapy) (left; n = 23). Kaplan–Meier analysis stratified by a Ki67 to LDH ratio of 0.065 (right; Ki67 to LDH ratio: high, n = 18; low, n = 5); log-rank test.
Supplementary information
Supplementary Information
This file contains Supplementary Tables 1-3. (PDF 269 kb)
Rights and permissions
About this article

Cite this article
Huang, A., Postow, M., Orlowski, R. et al. T-cell invigoration to tumour burden ratio associated with anti-PD-1 response. Nature 545, 60–65 (2017). https://doi.org/10.1038/nature22079
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/nature22079
This article is cited by
-
Efficacy and safety of thoracic radiotherapy in extensive-stage small-cell lung cancer patients receiving first-line immunotherapy plus chemotherapy: a propensity score matched multicentre retrospective analysis
Radiation Oncology (2024)
-
Efficacy and safety of PD-1 blockade plus long-course chemoradiotherapy in locally advanced rectal cancer (NECTAR): a multi-center phase 2 study
Signal Transduction and Targeted Therapy (2024)
-
Integrating artificial intelligence in osteosarcoma prognosis: the prognostic significance of SERPINE2 and CPT1B biomarkers
Scientific Reports (2024)
-
Adjuvant and neoadjuvant immunotherapies in hepatocellular carcinoma
Nature Reviews Clinical Oncology (2024)
-
Regorafenib plus nivolumab in unresectable hepatocellular carcinoma: the phase 2 RENOBATE trial
Nature Medicine (2024)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
