
Abstract
Hand-foot-and-mouth disease (HFMD) is a common childhood disease with substantial disease burden in Asia. Mixed results were reported on the associations between HFMD incidence and meteorological factors or school holidays, while limited studies focused on their association on transmissibility. We aimed to measure the transmissibility of HFMD and to examine its potential driving factors in Hong Kong. A likelihood-based procedure was used to estimate time-dependent effective reproduction number (Rt) based on weekly number of HFMD-associated hospitalizations from 2010 to 2014. The associations of between-year effects, depletion of susceptibles, absolute humidity and school holidays with Rt were examined using linear regression. Rt usually started increasing between early spring and summer and peaked in April to May at around 1.1–1.2, followed by a slight rebound in autumn. Depletion of susceptibles and between-years effects explained most of the variances (19 and 13% respectively) in Rt. We found a negative association between depletion of susceptibles and Rt (coefficients ranged from −0.14 to −0.03 for different years), but the estimated effects of absolute humidity and school holidays were insignificant. Overall, HFMD transmission was moderate in Hong Kong and was mainly associated with depletion of susceptibles. Limited impact was suggested from meteorological factors and school holidays.
Similar content being viewed by others

Introduction
Hand-foot-and-mouth disease (HFMD) causes a substantial disease burden in Asian regions including Hong Kong, mainly in children below 5 years of age1,2,3,4. Enterovirus 71 (EV71), coxsackievirus A16 (CA16) and coxsackievirus A6 (CA6) are the most common enterovirus serotypes causing HFMD in Hong Kong2,5. HFMD has a clear seasonal pattern in temperate regions with annual peaks in the summer1,6, while in tropical and subtropical regions including Hong Kong, multiple peaks may occur within a year2,7. Inconsistent findings about the associations between meteorological factors, such as temperature and relative humidity and the incidence of HFMD were reported by different studies6,7,8,9,10,11,12,13,14,15.
HFMD is considered to be transmitted mainly through direct contact with contaminated discharges, fluid of blisters or stool from infected persons, or contaminated objects16. Attending kindergarten or child-care center and visiting public playground were also reported as risk factors for HFMD17,18,19. HFMD is highly transmissible, with a basic reproduction number (R0) ranging from 2.5 to 5.5 for different serotypes in Hong Kong and Singapore20,21. A temperature of 21.1 to 26.7 °C, higher relative humidity and school period were reported to be associated with higher HFMD transmission in mainland China22. Other factors, such as host susceptibility and virus-specific transmissibility were also found to play vital roles in transmission of infectious diseases23. Currently, there is a lack of evidence about the potential risk factors and their impact on HFMD transmission. This study therefore aims to examine the transmissibility of HFMD and its potential driving factors in Hong Kong, where HFMD shows less obvious seasonality.
Results
Figure 1 shows the weekly HFMD-associated hospitalizations in Hong Kong between 1 January 2010 and 31 December 2014. Larger epidemics were observed in 2010 and 2013. A main summer peak from May to August was observed annually and the exponential growth phase usually started around March (Figs 1 and 2). Another milder autumn wave often occurred from September through early-October and sometimes extended into the winter. The HFMD epidemics usually peaked around the start of the summer holidays and other school vacations usually fell outside the main peak of HFMD epidemics. Hong Kong has a humid summer with relatively stable peak absolute humidity in May and August (Fig. 1). The mean absolute humidity was 17.2 g/m3 and fluctuated from 12.7 to 24.5 g/m3 during the study periods.

HFMD epidemic and transmission, absolute humidity and school vacations in Hong Kong, 2010–2014.
(A)Weekly effective reproduction number (Rt) of hand foot and mouth disease in Hong Kong, 2010–2014. Blue dots and vertical solid line represent non-smoothed weekly Rt and its 95% confidence interval (CI). Green lines and the green shade represent smoothed weekly Rt and its 95% CI. The dashed line represents the Rt threshold of 1. (B)Weekly mean absolute humidity in Hong Kong, 2010–2014. The 95% CI was estimated using bootstrap. The histogram in the two panels represents the weekly number of HFMD-associated hospitalizations while the light grey bars represent weeks in school vacations.

Identification of the main epidemic periods.
(A)The estimated daily number of hand foot and mouth disease from a smoothing spline. Background is the number of HFMD-associated hospitalizations by week while the light grey bars represent weeks in school vacations. (B)The growth rate of the estimated daily number of HFMD per day. The grey blocks represent the main HFMD epidemic period identified in each year.
The smoothed effective reproduction number (Rt) for HFMD began to increase above 1 during early January and late March (Fig. 1). Disregarding the exceptionally high Rt estimates in early 2014 due to a small number of cases, the smoothed Rt peaked at 1.12 to 1.24 in April or May and subsequently declined to below 1 in June or July preceding the peaks of the epidemic curve. The smoothed Rt usually remained above 1 for around 4 to 5 months from spring to mid-summer. A rebound of Rt occurred between August and October in autumn, then afterwards fluctuated below 1 for most of the time during winter. In the sensitivity analyses, Rt peaked at 1.17 to 1.26 by assuming a mean serial interval of 2 days; while Rt peaked at 1.42 to 1.60 when assuming the mean as 7 days. A longer serial interval led to larger uncertainty in the Rt estimates and slightly shortened the duration with estimated Rt ≥ 1 (Supplementary Fig. 1). The assumption on case-hospitalization risk (CHR) did not affect the point estimate of Rt but will result in narrower 95% confidence intervals for a lower CHR (Supplementary Fig. 2).
The regression model fitted with between-year effects, the depletion of susceptibles, absolute humidity and school vacations (Model 4 in Table 1, Fig. 3) explained 35% of the variance in Rt during the main epidemic periods. Depletion of susceptibles explained the most (19%) of the variance observed in Rt while between-year effects explained 13%. Absolute humidity and school vacations explained 2% and 1% of the variance in Rt respectively, though our results suggest absolute humidity does not explain the variance after accounting for autocorrelations (Table 2). For the sensitivity analysis which accounted for autocorrelations, the total variance in Rt explained was 26% (Table 2).

Weekly effective reproduction number (Rt) of HMFD during the study period in Hong Kong, 2010–2014.
Blue dots and vertical solid line represent non-smoothed weekly Rt of HFMD and its 95% CI estimated from the epidemic curve during the main epidemic periods; green line and the shades represent the smoothed weekly Rt and its 95% CI estimated from the epidemic curve; red line represents Rt estimated from the model fitted without adjusting autocorrelation. The histogram is the epidemic curve of the HFMD-associated hospitalizations by week while the light grey bars represent weeks in school vacations during the main epidemic periods.
We found a negative association between the depletion of susceptibles and Rt of HFMD (coefficients ranging from −0.14 to −0.03 among different years) and a marginally insignificant positive association between absolute humidity and the reproduction number (0.11, 95% confidence interval: −0.01 to 0.22) (Table 3). A significant positive association was also found between holidays and Rt while the association was not significant after adjusting for autocorrelation (Supplementary Table 1). Autocorrelogram and partial autocorrelogram of model residuals suggest unaccounted autocorrelations (Supplementary Fig. 3); however, results from models with or without adjustment for autocorrelation were very similar (Table 2 and Supplementary Tables 1 and 2), except that the association between holidays and Rt was not significant when accounted for autocorrelation. Sensitivity analyses on the end of HFMD epidemic period showed similar results (Table 2 and Supplementary Table 2). Results from models stratified by EV71 activity were also similar with our main findings (Supplementary Tables 3 and 4). We also did not find significant associations between other meteorological factors and HFMD transmission, except for temperature in one model accounting for the autocorrelation of Rt (results not shown).
Discussion
HFMD epidemics in Hong Kong occurred at least once per year and larger epidemics occurred every 2 to 3 years, similar to the pattern in other subtropical and tropical regions such as Macau, Taiwan, Singapore and Vietnam24,25,26. The main spring-summer peak usually started around March and peaked in June or July, while a milder autumn peak occurred after the start of a new school year in September. Smaller winter epidemics, which sometimes occurred in other subtropical regions, were also observed in 2012 and 2014 in Hong Kong1,2,27,28.
The estimated Rt usually exceeded 1 by March each year, corresponding to the exponential growth phase of the HFMD epidemic. Rt peaked in around April to May, suggesting that HFMD transmission was most intense well before summer. Rt dropped below 1 in June or July and rebounded to above 1 around September, probably driven by a new cohort of susceptible children entering kindergartens and the increase in contact rates among children in the new school year. However, further confirmatory study is needed to demonstrate the difference in transmission between the entry versus higher grades in kindergartens. Rt usually fluctuated below the threshold of 1in winter although mild HFMD activity can be observed in some years, indicating a generally low HFMD transmission during winter.
The estimated annual peak values of Rt ranged from 1.14 to 1.24 in the study period, indicating a relatively moderate HFMD transmissibility in Hong Kong. A transmission study in mainland China using a susceptible-infected-recovered model estimated a slightly higher Rt, ranging from 1.4 to 1.6 across different geographical regions22. In our study, the yearly intercepts log(R0S0 j), which is the logarithm of the product between R0 and the fraction of susceptibles at the beginning of each year, were estimated to range from −0.19 to 0.07 between 2008 and 2014, translating to an R0 ranging from 1.7 to 2.2 assuming 50% susceptibility at the start of the epidemic4,29,30. Two studies using similar statistical methods estimated that the R0 of HFMD ranged from 2.5 to 5.5 for the causative enterovirus serotypes CA16, CA6 and EV71 in Hong Kong and Singapore20,21. The estimates appear to be higher than that in our study, as the studies focused on institutional outbreaks rather than at the community level. In addition, R0 was highly sensitive to the assumed incubation period (R0 reduced by up to 50% for incubation period of 3 days instead of 5 days20) and the incubation period was assumed to be 5 days in the two studies, which is towards the upper end of the commonly quoted incubation period31,32.
Our results indicate that 35% of the variance in weekly Rt for HMFD can be explained by between-year effects, the depletion of susceptibles, absolute humidity and school holidays (Table 1). The order for potential driving factors of HFMD in our main results remained the same as that in the sensitivity analysis (explaining 22–49% of the variance in Rt), indicating that the relative importance of the above factors were not affected by the definition of the epidemic period23. The depletion of susceptibles appears to be the most important driving factor of HFMD transmission, while absolute humidity and school holiday seem to have limited effects on HFMD transmission.
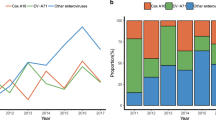
Between-year effects also explained a noticeable portion (13%) of the variation in HFMD transmission in Hong Kong. One possible reason was the alternating predominant serotype with different basic transmissibility and associated immunity in the community5,20,21. For example, 71% of the HFMD outbreaks in 2013 were associated with the subtype CA6, but only less than 30% for other years in our study period5. In the following year, only around 10% of the outbreaks were associated with the subtype CA6, with a similar proportion as other subtypes CA4, CA10 and EV715. The remaining unexplained variance in R0 may be partly due to factors such as the different control measures in the kindergartens and schools which were difficult to measure. The unexplained variance may also due to stochasticity and individual-level factors.
Our results showed an insignificant positive association between absolute humidity and Rt. Together with the low R2 explained, the absolute humidity may have limited effect on the transmission of HFMD in Hong Kong. We did not identify any other important driving meteorological factors (e.g. rainfall and sunshine) on HFMD transmission, with an exception for temperature under the model adjusting for autocorrelations (data not shown). A number of studies have reported a positive association between HFMD incidence and meteorological factors such as temperature and relative humidity, although some of the studies were conducted in temperate regions6,7,8,9,10,11,12,13. Once an epidemic takes off, the number of new cases will continue increasing even when Rt decreases but stays above 1. This feature somehow makes our results less comparable with previous findings which mostly focused on incidence. Another possible reason for the inconsistency is that Hong Kong is a subtropical city with relatively high temperature (median 27.0 °C, IQR 21.7–28.7 °C) and relative humidity (median 83.1%, IQR 79.4–86.4%) in most of the main epidemic periods and transmission of HFMD may be most efficient at a temperature of 23.9 °C and higher relative humidity22. Our model is therefore underpowered to detect the full impact of the meteorological factors due to the small number of days when the transmission is not active in Hong Kong. More evidence on the underlying biological mechanism of HFMD transmission is needed to improve the understanding of the potential effect of meteorological factors.
Summer or spring school breaks with duration longer than one month were reported to be associated with lower HFMD transmission22. Our results however did not suggest that school holidays substantially reduced the transmission of HFMD in Hong Kong. This may be partially explained by the fact that Hong Kong has relatively short school holidays except for the summer holidays. In many cases, Rt has already been decreasing well before the summer holiday (Fig. 2). Besides, previous findings showed that household plays an important role in HFMD transmission, where the transmission risk among siblings could reach 84%33. Public playground, which younger children would go for during school holidays, was reported as a risk factor of HFMD transmission18,19. We did not attempt to examine the potential effect of reactive school closure due to HFMD outbreaks, during which the social activities of the children may have a very different pattern from those in holidays. There were large HFMD outbreaks in 2010 in Hong Kong which led to some school closures and had significantly raised the awareness and preparedness in the schooling setting in the subsequent years. Considering the high social cost and enhanced preventive measures already in place at schools, the additional effect of school closure to reduce HFMD transmission may be limited. Furthermore, even if the EV71 vaccine would be available in Hong Kong in the future, it may have limited effect on HFMD transmission at the population, as the EV71 serotype was responsible for less than 20% of the HFMD outbreaks in Hong Kong5. However, EV71 is disproportionately responsible for the most severe HFMD infections1.
This study focused on the transmissibility of HFMD which has more direct implications on the control measures, while incidence depends on the combined effect of transmissibility and time to symptom appearance. Our study has several limitations. First, our estimations were based on hospitalized HFMD cases and may not reflect trend of population incidence reliably if the CHR changed substantially within a short period. Second, Rt could be overestimated if there were substantial imported cases or differences in transmissibility among serotypes. Third, we adopted the dates of summer vacations from the Education Bureau, but some kindergartens started schools earlier in August. This may partly explain the rebound of Rt slightly earlier than the start of the school year in September for most schools. Finally, we could not establish causation between HFMD transmission and various potential driving factors. However, the lack of association between meteorological variables and HFMD transmissibility may indicate limited effectiveness in weather-based strategies, especially for places such as Hong Kong with strengthened hygiene measures in schools.
Conclusions
Transmissibility of HFMD in Hong Kong was relatively moderate in 2010–14. Depletion of susceptibles was the most important driving factor of the HFMD transmission dynamics. Meteorological factors and school vacations appear to have limited impact on HFMD transmission in Hong Kong.
Methods
Data sources
The weekly numbers of HFMD-associated hospitalizations between 1 January 2010 and 31 December 2014 in all public hospitals in Hong Kong are publicly available from the Centre for Health Protection (CHP) website34. The year-end and mid-year populations of Hong Kong for the years 2009 through 2014 were obtained from the Census and Statistics Department of Hong Kong35. Weekly and daily population were estimated by linear interpolation assuming the growing rate of population were uniform during each half-year interval. Daily counts of HFMD cases (ns) were derived from the weekly data as follows: we first calculated the weekly HFMD-associated hospitalizations rate It by dividing the weekly number by the interpolated weekly population. The cumulative incidence of HFMD-associated hospitalizations (Ct) in each week t was then calculated. We used cubic spline interpolation to obtain the cumulative daily incidence (Cs) and took the daily difference of Cs to derive daily incidence (Is). The case-hospitalization risk (CHR), which is defined as the risk of hospitalization among all HFMD cases, was assumed to be constant at 1.3%, based on a previous study in Hong Kong2. Finally, nswas derived using daily incidence, case-hospitalization risk and daily population.
We obtained the daily mean temperature (°C) and daily relative humidity (%) between 2010 and 2014 from the Hong Kong Observatory36. Absolute humidity was shown to have a more direct effect on the activity of several viruses and hence was used in our main analysis37,38,39. We calculated absolute humidity (g/m3), using Bolton’s conversion formula based on mean temperature and relative humidity40. Weekly absolute humidity was calculated as the arithmetic mean of daily absolute humidity in the corresponding week.
School vacations considered in the study include the Christmas, New Year, Chinese Lunar New Year, Easter and school summer holidays, which usually last for at least one week for most kindergartens and schools in Hong Kong. The period of school vacations was determined according to the guideline of school calendar issued by the Education Bureau41. The summer holiday was defined as from mid-July to the end of August, while the other holidays were defined as the week(s) when most of the general holiday days fell.
Effective reproduction number
We adopted the likelihood-based approach proposed by Wallinga et al. and Cauchemez et al. to estimate the daily reproduction number (Rs)42,43 accounting for right censoring, which is outlined below. We first calculated the relative probability (pks) that cases with illness onset on day k were infected by cases showing symptoms on day s, based on an assumed serial interval distribution w(·). We then obtained Xs, the number of secondary case infected by cases on day s, by assuming a binomial distribution Bin(ns, pks) and observable infected cases governed by w(·). Rs was calculated by dividing Xs with ns. The weekly Rt was calculated as the geometric mean of the estimated daily Rs. We assumed a negligible number of imported cases in the study period. The serial interval of HFMD was assumed to follow a Weibull distribution with mean 3.7 days and standard deviation 2.6 days33. Sensitivity analyses were conducted assuming serial intervals with mean 2 days and 7 days respectively and a CHR of 0.6% and 2.8%. To capture the overall trend of HFMD transmissibility in Hong Kong, we also estimated the smoothed Rt based on spline smoothed average weekly incidence with the lowest generalized cross-validation (GCV) score44.
Potential factors of HFMD transmissibility
To further examine the potential factors that influence HFMD transmission, we used the linear regression approach as proposed by te Beest et al.23. Weekly Rt was used as proxy of HFMD transmission. Rt was assumed to be proportional to the basic reproduction number R0, scaled by the between-year effects, depletion of susceptibles and effects of absolute humidity (AH) and school vacations (V). Based on the above assumption, the linear regression model can be expressed as23:

where Rtj is the effective reproduction number in week t of year j; βoj denotes the between-year intercepts, which represents different susceptibility in the beginning of each year j; Ctj is the weekly cumulative incidence of HFMD up to week t-1. The coefficients βj, βAH and βV represent the effect of the yearly depletion of susceptibles, absolute humidity and school vacations. To assess the potential impact of autocorrelation, we conducted a sensitivity analysis by fitting models accounting for autocorrelations in Rt.
The analysis was restricted to the main wave of HFMD epidemics, defined as the period from the beginning of exponential growth phase through the last week of August for each year. The exponential growth phase was defined as the period when the estimated daily number of HFMD increased steadily and the growth rate (Δns) continuously increased for no less than two months at the beginning of an epidemic. This allowed for the different start time of HFMD epidemic in each year (Fig. 2) and controlled for the new cohort of students admitted to the kindergartens in September each year. We also carried out sensitivity analyses by defining the end of HFMD epidemic period in July, September or October. Other meteorological factors such as temperature, relative humidity and air pressure were also tested. We also carried out a sensitivity analysis by stratifying the years of EV71 activity to account for the potential impacts of changing predominant serotypes.
All analyses were conducted in R version 3.1.1 (R Foundation for Statistical Computing, Vienna, Austria). We provided detailed statistical methods in the web appendix.
Additional Information
How to cite this article: Yang, B. et al. Transmission of Hand, Foot and Mouth Disease and Its Potential Driving Factors in Hong Kong. Sci. Rep. 6, 27500; doi: 10.1038/srep27500 (2016).
References
Xing, W. et al. Hand, foot and mouth disease in China, 2008–12: an epidemiological study. Lancet Infect Dis. 14, 308–318 (2014).
Ma, E., Lam, T., Chan, K. C., Wong, C. & Chuang, S. K. Changing epidemiology of hand, foot and mouth disease in Hong Kong, 2001–2009. Jpn J Infect Dis. 63, 422–426 (2010).
Solomon, T. et al. Virology, epidemiology, pathogenesis and control of enterovirus 71. Lancet Infect Dis. 10, 778–790 (2010).
Yang, B. et al. Seroprevalence of Enterovirus 71 Antibody Among Children in China: A Systematic Review and Meta-analysis. Pediatr Infect Dis J. 34, 1399–1406 (2015).
Centre for Health Protection. Update on Situation of Enterovirus Infection. (2015) Available at: http://www.chp.gov.hk/files/pdf/update_on_situation_of_ev_infection.pdf. (Accessed: December 13 2015).
Onozuka, D. & Hashizume, M. The influence of temperature and humidity on the incidence of hand, foot and mouth disease in Japan. Sci Total Environ. 410–411, 119–125 (2011).
Hii, Y. L., Rocklov, J. & Ng, N. Short term effects of weather on hand, foot and mouth disease. PLoS One. 6, e16796 (2011).
Feng, H., Duan, G., Zhang, R. & Zhang, W. Time series analysis of hand-foot-mouth disease hospitalization in Zhengzhou: establishment of forecasting models using climate variables as predictors. PLoS One. 9, e87916 (2014).
Huang, Y. et al. Effect of meteorological variables on the incidence of hand, foot and mouth disease in children: a time-series analysis in Guangzhou, China. BMC Infect Dis. 13, 134 (2013).
Liu, W. et al. Spatiotemporal Dynamics of Hand-Foot-Mouth Disease and Its Relationship with Meteorological Factors in Jiangsu Province, China. PLoS One. 10, e0131311 (2015).
Liu, Y. et al. Spatio-temporal analysis of the relationship between climate and hand, foot and mouth disease in Shandong province, China, 2008–2012. BMC Infect Dis. 15, 146 (2015).
Ma, E., Lam, T., Wong, C. & Chuang, S. K. Is hand, foot and mouth disease associated with meteorological parameters? Epidemiol Infect. 138, 1779–1788 (2010).
Wei, J. et al. The effect of meteorological variables on the transmission of hand, foot and mouth disease in four major cities of shanxi province, China: a time series data analysis (2009–2013). PLoS Negl Trop Dis. 9, e0003572 (2015).
Dong, W. et al. The Effects of Weather Factors on Hand, Foot and Mouth Disease in Beijing. Sci Rep. 6, 19247 (2016).
Lee, C. C., Tang, J. H., Hwang, J. S., Shigematsu, M. & Chan, T. C. Effect of Meteorological and Geographical Factors on the Epidemics of Hand, Foot and Mouth Disease in Island-Type Territory, East Asia. Biomed Res Int. 2015, 805039 (2015).
World Health Organization. Hand, foot and mouth disease information sheets. (2012) Available at: http://www.wpro.who.int/emerging_diseases/hfmd.information.sheet/en/. (Accessed: January 15 2016).
Chang, L. Y. et al. Risk factors of enterovirus 71 infection and associated hand, foot and mouth disease/herpangina in children during an epidemic in Taiwan. Pediatrics. 109, e88 (2002).
Xie, Y. H. et al. Important roles of public playgrounds in the transmission of hand, foot and mouth disease. Epidemiol Infect. 143, 1432–1441 (2015).
Sun, L. et al. Evaluating the transmission routes of hand, foot and mouth disease in Guangdong, China. Am J Infect Control. 44, e13–14 (2016).
Lim, C. T., Jiang, L., Ma, S., James, L. & Ang, L. W. Basic reproduction number of coxsackievirus type A6 and A16 and enterovirus 71: estimates from outbreaks of hand, foot and mouth disease in Singapore, a tropical city-state. Epidemiol Infect. 1–7 (2015).
Ma, E. et al. Estimation of the basic reproduction number of enterovirus 71 and coxsackievirus A16 in hand, foot and mouth disease outbreaks. Pediatr Infect Dis J. 30, 675–679 (2011).
Wang, Y. et al. Hand, foot and mouth disease in China: patterns of spread and transmissibility. Epidemiology. 22, 781–792 (2011).
te Beest, D. E., van Boven, M., Hooiveld, M., van den Dool, C. & Wallinga, J. Driving factors of influenza transmission in the Netherlands. Am J Epidemiol. 178, 1469–1477 (2013).
Ministry of Health Singapore. Communicable Diseases Surveillance in Singapore. Available at: https://www.moh.gov.sg/content/moh_web/home/Publications/Reports.html. (Accessed: November 18 2015).
World Health Organization. Hand, foot and mouth disease situation update. (2015) Available at: http://www.wpro.who.int/emerging_diseases/HFMD/en/. (Accessed: November 18 2015).
Chen, K. T., Chang, H. L., Wang, S. T., Cheng, Y. T. & Yang, J. Y. Epidemiologic features of hand-foot-mouth disease and herpangina caused by enterovirus 71 in Taiwan, 1998–2005. Pediatrics. 120, e244–252 (2007).
Chan, K. P. et al. Epidemic hand, foot and mouth disease caused by human enterovirus 71, Singapore. Emerg Infect Dis. 9, 78–85 (2003).
Tu, P. V. et al. Epidemiologic and virologic investigation of hand, foot and mouth disease, southern Vietnam, 2005. Emerg Infect Dis. 13, 1733–1741 (2007).
Ang, L. W. et al. Seroepidemiology of Coxsackievirus A6, Coxsackievirus A16 and Enterovirus 71 Infections among Children and Adolescents in Singapore, 2008–2010. PLoS One. 10, e0127999 (2015).
Diedrich, S., Weinbrecht, A. & Schreier, E. Seroprevalence and molecular epidemiology of enterovirus 71 in Germany. Arch Virol. 154, 1139–1142 (2009).
Ministry of Health Singapore. Hand, Foot & Mouth Disease. (2014) Available at: https://www.moh.gov.sg/content/moh_web/home/diseases_and_conditions/h/hfmd.html. (Accessed: January 05 2016).
National Health Service. Hand, foot and mouth disease. (2014) Available at: http://www.nhs.uk/Conditions/Hand-foot-and-mouth-disease/Pages/new_Symptoms.aspx. (Accessed: January 05 2016).
Chang, L. Y. et al. Transmission and clinical features of enterovirus 71 infections in household contacts in Taiwan. JAMA. 291, 222–227 (2004).
Center for Health Protection. Hospital Admission Episodes reported by Hospital Authority. (2015) Available at: http://www.chp.gov.hk/en/sentinel/26/44/699.html. (Accessed: January 5 2015).
Census and Statistics Department Hong Kong Statistics. (2015) Available at: http://www.censtatd.gov.hk/hkstat/. (Accessed: January 5 2015).
Hong Kong Observatory Past weather. (2015) Available at: http://www.hko.gov.hk/wxinfo/pastwx/past.htm. (Accessed: 1 July 2015).
Shaman, J. & Kohn, M. Absolute humidity modulates influenza survival, transmission and seasonality. Proc Natl Acad Sci USA 106, 3243–3248 (2009).
Colas de la Noue, A. et al. Absolute Humidity Influences the Seasonal Persistence and Infectivity of Human Norovirus. Appl Environ Microbiol. 80, 7196–7205 (2014).
Xu, H. Y. et al. Statistical modeling reveals the effect of absolute humidity on dengue in Singapore. PLoS Negl Trop Dis. 8, e2805 (2014).
National Oceanic and Atmospheric Administration. Relative humidity and dewpoint temperature from temperature and wet-bulb temperature. (2015) Available at: http://www.srh.noaa.gov/images/epz/wxcalc/rhTdFromWetBulb.pdf. (Accessed: August 20 2015).
Education Bureau. Guidelines on Drawing up the School Calendar. (2015) Available at: http://www.edb.gov.hk/en/curriculum-development/resource-support/guidelines-sch-calendar/index.html. (Accessed: 15 July 2015).
Cauchemez, S. et al. Real-time estimates in early detection of SARS. Emerg Infect Dis. 12, 110–113 (2006).
Wallinga, J. & Teunis, P. Different epidemic curves for severe acute respiratory syndrome reveal similar impacts of control measures. Am J Epidemiol. 160, 509–516 (2004).
Craven, P. & Wahba, G. Smoothing noisy data with spline functions. Numerische Mathematik. 31, 377–403 (1978).
Acknowledgements
The authors thank Sheikh T. Ali for technical assistance. This project was supported by the Harvard Center for Communicable Disease Dynamics from the National Institute of General Medical Sciences (grant no. U54 GM088558), the Early Career Scheme from the Research Grants Council of the Hong Kong Special Administrative Region (grant no. 27100814) and a commissioned grant from the Health and Medical Research Fund from the Government of the Hong Kong Special Administrative Region (grant no. HKS-16-E07).
Author information
Authors and Affiliations
Contributions
B.Y. participated in study design, performed the analysis and wrote the manuscript. E.H.Y.L. participated in the study design, analysis and critically reviewed the manuscript. P.W. critically reviewed the manuscript. B.J.C. participated in the study design, analysis and critically reviewed the manuscript. All authors contributed to the interpretation of the data, drafting the article and final approval of the version to be published.
Ethics declarations
Competing interests
BJC has received research funding from MedImmune Inc. and Sanofi Pasteur and consults for Crucell NV.
Electronic supplementary material
Rights and permissions
This work is licensed under a Creative Commons Attribution 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/
About this article

Cite this article
Yang, B., Lau, E., Wu, P. et al. Transmission of Hand, Foot and Mouth Disease and Its Potential Driving Factors in Hong Kong. Sci Rep 6, 27500 (2016). https://doi.org/10.1038/srep27500
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/srep27500
This article is cited by
-
Trend analysis and forecast of daily reported incidence of hand, foot and mouth disease in Hubei, China by Prophet model
Scientific Reports (2021)
-
Spatial-temporal heterogeneity of hand, foot and mouth disease and impact of meteorological factors in arid/ semi-arid regions: a case study in Ningxia, China
BMC Public Health (2019)
-
The complex transmission seasonality of hand, foot, and mouth disease and its driving factors
BMC Infectious Diseases (2019)
-
Development and evaluation of a deep learning approach for modeling seasonality and trends in hand-foot-mouth disease incidence in mainland China
Scientific Reports (2019)
-
Recombinant heat shock protein 78 enhances enterovirus 71 propagation in Vero cells and is induced in SK-N-SH cells during the infection
Archives of Virology (2017)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
