
Abstract
Studydesign:
Epidemiological survey.
Objectives:
To study the incidence and epidemiology of acute traumatic spinal cord injury (ATSCI) of 2002 in Beijing municipality.
Setting:
Beijing.
Methods:
After quota sampling, data of all ATSCI patients who were injured in Beijing in 2002 from sample hospitals were collected for detailed investigation.
Results:
In all, 1079 patients were estimated to have ATSCI in 2002 in Beijing municipality and the annual incidence was 60.6 per million. The incidence increased more than ninefold compared with that of 6.7 per million between 1982 and 1986. The mean age of patients at the time of injury was 41 years. The male/female ratio was 3.1/1. The causes of injury were fall from height (37.5%), traffic accidents (26.9%), struck by object (16.3%) and fall on ground (8.3%), in that order. The mean expenditure of hospitalisation was 27819.3 RMB in 2002. The proportion of cervical, thoracic and lumbar injuries was 4.9, 28.0 and 65.9, respectively in 2002. The mean time of hospitalisation was 18.9 days and only 1.5% of the spinal cord injury (SCI) patients went to rehabilitation hospitals after their discharge. The severity of neurological impairment was not recorded in the majority of hospitals.
Conclusion:
There was a rapid increase of the annual SCI incidence from 1982 to 2002 during an economic boom. Safety regulations are of primary importance in preventing the injury. Once happened, long-term health insurance is essential for the well-being of the victims. Although some improvement has been made since 2002, much remains to be done in this direction.
Similar content being viewed by others

Introduction
Spinal cord injury (SCI) is a devastating and debilitating condition that affects all regions of the world.1, 2 Its pathology affects multiple systems of the human body, and its management could be lengthy and very expensive. Although on its own, it affects only a small section of the population, its impact spreads far beyond the victims themselves to people and institutions surrounding and supporting them, such as relatives, carers, friends, construction and other industries, social welfare system, charities, regulatory bodies and many others. It becomes even more so in developing countries where nationwide rehabilitation programs are almost non-existent, and the victims totally dependent. Prevention is the best way to minimise such adverse impact. Since early 1990, China has experienced a sustained economic boom. According to Ackery et al.,1 SCI incidence was closely related with the economy of the country. Hence, changes in the incidence and causes of SCI were expected in China. An epidemiological survey to shed some light on the issue would be instrumental in formulating an up-to-date prevention strategy.
Materials and methods
Stratification of data collection
The hospitals in Beijing are divided into two categories depending upon the nature of their authorities, namely civilian hospitals and military hospitals. The latter also treat civilians. Civilian hospitals are subdivided into primary, secondary and tertiary hospitals according to their size and expertise. Military hospitals are mostly tertiary. There is no specialised centre for trauma. Public and health authorities recognise a hospital with strong orthopaedic department as specialised in trauma. In this study, three civilian hospitals were classified as such. As to SCI, there was and still is no specialised centre in strict sense, except one. It is known as the China Rehabilitation Research Centre where acute care to completion of medical rehabilitation is provided. However, the general misperceptions that rehabilitation is a second rate service and acute traumatic spinal cord injury (ATSCI) patients must be treated surgically have led to the allocation of these patients to the nearest hospitals where spine surgery can be done at the earliest. These misperceptions have made spine surgery popular and widely done. The overwhelming majority of ATSCI patients in these hospitals do not receive any rehabilitation owing to either financial restraint or lack of expertise. Hospitals of traditional Chinese medicine normally do not take ATSCI patients.
The survey was approved by the Beijing Health Bureau and authorities of military hospital involved in the survey.
The data for the survey were searched in the Information Center of Beijing Health Bureau, using the term ‘paraplegia’ or ‘tetraplegia’ in Chinese language. The normal practice is that patients’ data were reported to and archived in the Bureau after discharge of patients. One thousand seven hundred and ninety two ATSCI patients were admitted to civilian hospitals from 1 January to 31 December 2002, while 205 patients were admitted to military hospitals during that period. Materials from military hospitals were not reported to the bureau and kept confidential within the military establishment. However, access to materials of individual military hospitals was permitted. This was the way data from relevant military hospitals were collected. There were four military hospitals well known for taking ATSCI patients. They were all chosen for the survey. The method of collecting data was quota sampling. The statistical method of sampling was designed by the Mathematical Department of Capital University of Medical Sciences.
Altogether, 1997 patients with ATSCI from 86 hospitals were documented in the archives. Of these hospitals, 82 were civilian. Three of the civilian hospitals were more or less specialised in SCI, although none of them offered comprehensive management in strict sense. All their ATSCI patients were included for analysis. Apart from the 3 specialised hospitals, of which all were included, the primary principle of stratification of the other 79 civilian hospitals was their size and expertise, as just mentioned. They were further divided into eight zones depending upon their distance from the city centre. One biggest hospital was chosen from each of the eight zones to represent the zone and detailed data were collected for analysis. Of the four military hospitals, two were randomly chosen for further detailed analysis together with the civilian hospitals. The high rate of two out of four was used because military hospitals were normally of high expertise and attracted more ATSCI patients than average civilian hospitals. In summary, a total of 13 hospitals, namely three specialised civilian, eight general civilian and two military, were included for detailed demographic, social and medical data collection and analysis.
The survey team was composed of three groups. Each group consisted of a rehabilitation physician and two rehabilitation nurses. They had been briefed and trained for the purpose and standardised method of conducting the survey before they embarked on the retrospective review of medical records of ATSCI patients. SPSS10 was used for statistical analysis.
From the above-mentioned 13 hospitals, the total number of ATSCI patients was 710. They included those injured in and outside Beijing. When those injured outside Beijing were excluded, there were only 264 patients who were injured in Beijing. These patients serve as the material for epidemiological analysis below.
The proportion of ATSCI patients in each category of the sample hospitals, who were injured in Beijing, was calculated by dividing the number of these patients in the category by the total number of ATSCI patients, regardless of their location of injury:
Proportion of ATSCI patients of each category=

Assuming that all hospitals in each category had similar percentage of ATSCI patients who were injured in Beijing as the sample hospitals did, then the total number of such patients in various categories can be calculated using the following formula: total number of ATSCI patients of all hospitals in the category × % of patients injured in Beijing in the category.
Results
Incidence
The average proportions of ATSCI patients in each category of sample hospitals, who were injured in Beijing, are:
-
1
General civilian hospitals: 159/252 (63.1%)
-
2
Specialised civilian hospital: 75/412 (18.2%)
-
3
Military hospitals: 30/46 (65.2%)
-
4
The numbers of patients injured in Beijing of all hospitals in each category are:
-
5
General civilian hospitals: 1380 × 63.1%=870
-
6
Specialised civilian hospital: 412 × 18.2%=75
-
7
Military hospitals: 205 × 65.2%=134
-
8
Total 1079
Hence, the estimate of total of ATSCI occurred in the entire Beijing municipality in 2002 based on all admissions into hospitals is 1079.
A total of 1079 patients sustained ATSCI in Beijing. During this period, the permanent population amounted 14 million, while floating 3.8 million. The total population was 17.8 million. Hence, the annual incidence of ATSCI was estimated to be 60 per million population.
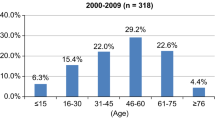
Gender and age
Among the 264 ATSCI patients, there were 200 male and 64 female patients, the male/female ratio being 3:1. The youngest at the time of injury was 6 years, while the oldest was 80 years, with a mean age of 41.7 years (Figure 1).

Age distribution at the time of injury.
Vocation
The vocational characteristics are shown in Table 1. The industrial workers and farmers constituted the majority of 62.5%. The large number of unclassified occupation is due to poor documentation. This on its own indicates that the overwhelming majority of them were migrant workers in the construction industry who did not even have a proper identity in the city.
Cause
The major causes of ATSCI were fall from height, road traffic accident and hit by an object, in order of frequency. They constituted 82.2% of all cases. The breakdown is shown in Table 2.
Level of vertebral injury
The level of vertebral injury and its relation to age are shown in Figure 2. Apart from 3 patients (1.1%) with unknown level of injury, cervical injuries were recorded in 13 patients (4.9%), thoracic in 74 (28.0%), thoracolumbar, lumbar and lumbosacral in 176 (66.0%). Regardless of the level of injury, the peak age is always between 30 and 49 years. Neurological impairment was so poorly documented that the data were not satisfactory for analysis.

Breakdown of level of vertebral injury in relation to age.
Management
Ninety-seven patients (36.7%) had received surgical treatment for stabilisation of the spine. The remaining 167 patients received conservative treatment.
Length of hospitalisation
The time of hospitalisation was 1–136 days, with a mean of 18.9 days. The details were presented in Figure 3. The reason of short stay in hospital was financial and lack of rehabilitation facilities in almost all cases.

Length of stay in hospital (days).
Expenses of hospitalisation
The average expense of hospitalisation was 27 819.3 RMB (Chinese currency unit), a rough equivalent of $3500. Of 51.8% of the patients, the expenses were below 5000 RMB, a rough equivalent of $525 in 2002. The breakdown of expenses is shown in Table 3.
Destination after discharge from acute hospital
Of the 264 patients, only 4 (1.5%) went to rehabilitation hospitals after acute hospitals, while 250 (94.7%) went home without further treatment or rehabilitation. The destinations of the remaining 10 patients (3.8%) were unclear.
Discussion
Before the current epidemiological survey of ATSCI, there was another survey conducted in the Beijing municipality during 1982–1986. The previous one covered the period when China's economy began to open to the outside world, while the current one experienced a booming economy with unprecedented pace.
In both surveys, the overwhelming cause of injury was fall from height, 36% in the previous, while 41% in the current one. However, the overall incidence had risen drastically from 6.7 per million to 60 per million population, a little over ninefold. The populations of these two surveys were not totally comparable. In the 1987 survey, only permanent residents were included, while the 2003 SCI survey included all patients admitted to hospitals of Beijing municipality regardless of their status of residency, permanent or temporary. The latter involved a large population of migrant workers who constituted 70–90% of all workforce in the construction industry that expanded rapidly and enormously to cope with the pace of the economic development.3, 4, 5 It was this workforce who sustained fall from height most despite this difference in inclusion of candidates between the two studies. The inclusion of migrant workers, the overwhelming majority of whom were construction workers, and the colossal scale of construction of 2002 explain the drastic ninefold increase of SCI. The incidence was the highest of all reports on ATSCI, occurring from late 1980s worldwide.6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30 The high incidence and its pattern can to certain extent reflect the scale and pace of economic development, particularly in rapidly developing countries. It also helps understand the culture of the country and its people.
Lack of strict safety regulations and insurance contributed to the high incidence. Proper management of acute stage was impossible without medical insurance, let alone that beyond it. Obviously, resolving these issues is far beyond the responsibility of medical profession. Under public and government pressure and guidance, the situation has been improved dramatically since 2002. However, studies are needed to substantiate the improvement.
The male/female ratio of 3/1 is in the lower middle of the ranges reported in the literature. The highest of 5.8/1 was recorded in Jordan, while the lowest of 2.4/1 in the United States.11, 30 This was probably due to the difference in culture to what degree women are exposed to the open society and risk of SCI.
The peak age in the overwhelming reports is 20–29 because, as a general rule, population of this age group are most active physically and easily exposed to SCI. However, in this study, the first and second peak age groups were 30–39 and 40–49, respectively.10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34 It was because fall from height in construction industry was the main cause of injury followed by road traffic accident. In China, members of a farmer's family aged 20–29 are not keen to travel far away from home to take a risky job like construction worker. They prefer staying at home, getting married and establishing a family. Only afterwards, they go to big cities to find a job with higher earning. As to road traffic accident, people of 20–29 are not rich enough to own a car or become a professional driver because of lack of experience. As fall from construction site and road traffic accident are the main causes of injury, people of 30–39 prevailed instead of those of 20–29. Also, people of 20–29 were not as active as their western counterparts in those activities that could lead to SCI, such as horse riding, rugby, skiing, assault and so on. It is exceptional that in a Japanese report, the main peak was at 59 years. This is obvious because of the high incidence of degenerative diseases of the spine, particularly cervical spine in Japan. Although ossification of the posterior longitudinal ligament is also seen in other countries, including China, it is a rarity. The high incidence of cervical injuries in Japan further supports this judgement.16 There is no cervical injury before the age of 30 simply because they were well protected. In contrast to western people, Chinese are not keen to take physical risk at this stage when safe earning is the priority of their life.
Domestic fall of the elderly was null in this survey. Although isolated cases may have slipped through the survey, the number is definitely negligible. Such a low incidence is due to housing characteristics. Beijing residents live in flat of high-rise buildings. In developed countries, where many old people live on their own in houses with staircase, domestic fall from stairs is common. In China, most old people live in apartments of high-rise buildings. They move up and down via lift and hence domestic fall from staircase is very rare. They are also less active than their western counterparts and well protected by their younger generations in a Chinese traditional extended family. In addition, Chinese have much few degenerative diseases of the spine compared with the Japanese.
The very low incidence of cervical injury (4.9%) in sharp contrast with the very high one (51%) of the 1982–86 survey needs some explanation.2 First, it is due to the different populations involved in the surveys. The 1982–86 survey included only permanent residents. Migrant workers were completely excluded. Therefore, a huge number of falls of construction workers who belonged to this category were not reported. This made the number of cervical injuries appear to be comparatively high. The cause of cervical injuries is mainly road traffic accidents. It is very rare among migrant workers who hardly use any fast moving motor vehicles, public or private. However, they are the major population of more than 70% of the entire cohort of this study, including workers, farmers and unidentified population. The remaining 30% of the 264 patients amount to 80 permanent Beijing residents. Then, 13 patients of cervical injury constitute 16% of these 80 permanent Beijing residents. However, 16% is still too far below the 51% of the 1982–1986 survey. The second possible explanation could be that because of the dramatically improved living, shopping and others services in the local community from 1980s to 2000s, many people, particularly housewives no longer need to travel long distance within the city by motor vehicles as it was the case in the 1980s. In the 1980s, there was only one big department store in the entire Beijing, while in 2002 it was everywhere. All these hypotheses need further survey to substantiate them.
The expenses of health care of the year of this survey were relatively low. It has risen many fold since then because of inflation in line with the rapid development of economy and technology. The coverage of the expenses was not recorded in the medical records for analysis. However, the small number of state-paid employees of 19 (7.2%) explains that most victims did not receive long-term insurance cover because in China only state-paid employees received such generous insurance cover. The cover for construction workers was restricted to acute stage of no more than a month. Of the 80 patients whose vocations were unclassified, the overwhelming majority of them had to be devoid of long-term insurance cover because otherwise their vocations would have been documented in the medical records. Most of them were likely to be migrant workers.
Owing to limited funding, the samples were smaller than what the authors liked to see. Despite this limitation, the survey has shed some light on the current status and problems of SCI prevention and management of a rapidly developing country. Although, the results of the survey may not precisely reflect the reality in its entirety, the trend of increase of SCI incidence and change of pattern is unmistakable. It has to be pointed out that the incidence of SCI cannot keep increasing forever. There must be a point at which it will plateau and go down when the conditions improve.
It is regretful that no follow-up was done because of financial restraint, and practical difficulties of lacking permanent contact details of a huge number of migrant workers. This would be possible only if China's economy improved tremendously. Since 2002, much stricter safety regulations on construction industries have been implemented and basic health insurance for acute care has become compulsory. The obvious impression of improvement needs another survey to substantiate it. It is worth reminding that at the moment although China's GDP ranks third in the world, when divided by a huge population of 1.4 billion, its GDP per capita ranks only 98, immediately after Albania as estimated by International Monetary Fund in 2009.35 China remains a developing country in real sense. As SCI service is closely related to economy, medical profession cannot on its own influence the progress. As China's economy is developing with unprecedented pace, it is expected that in a few decades, health insurance and expertise in SCI care can be improved to international standard with involvement of medical expertise
References
Ackery A, Tator C, Krassioukov A . A global perspective on spinal cord injury epidemiology. J Neurotrauma 2004; 21: 1355–1370.
Wyndaele M, Wyndaele J-J . Incidence, prevalence and epidemiology of spinal cord injury: what learns a worldwide literature survey? Spinal Cord 2006; 44: 523–529.
Spinal cord injury investigating group in Beijing. The reviewing survey for spinal cord injury in Beijing between 1982–1986. J Ch rehabil 1988; 3: 59–62 (Chinese).
Statistical Bureau of Beijing. Statistical Yearbook of Beijing 2003, Vol 6. Statistical Publishing House of Beijing: Beijing, 2003, pp 58, 74, 285, 391, 416, 479, 484, 494 (in Chinese).
Statistical Bureau of Beijing. Social and Economic Statistical Yearbook of Beijing 1987, Vol 9. Statistical Publishing House of Beijing: Beijing, 1987 p 1359 (in Chinese).
Wang D, Wu X, Shi G, Wang Y . China's first total care unit for the spinal cord injured. Paraplegia 1990; 28: 318–320.
Beijing increases migrant worker's salary for construction of Olympic venues. http://en.beijing2008.cn/25/97/article214009725.shtml.
Wang S, Wu H . Unions protect migrant workers. http://211.167.236.236/zt/magazine/200402007412100101.html.
Andrew Scheineson. China's internal migrants. http://www.cfr.org/publication/12943/chinas_internal_migrants.html (updated 14 May 2009).
Shingu H, Ikata T, Katoh S, Akatsu T . Spinal cord injuries in Japan: a nationwide epidemiological survey in 1990. Paraplegia 1994; 32: 3–8.
Lan C, Lai JS, Chang KH, Kan YC . Lein traumatic spinal cord injuries in the rural region of Taiwan; an epidemiological study in Hualien County, 1986–1990. Paraplegia 1993; 31: 398–403.
Nan D, Miao H . Medical Rehabilitation. The People's Publishing House of Health: Beijing, 1993 p 232 (in Chinese).
Karacan İ, Koyuncu H, Pekel Ö, Sümbüloǧlu G, Kirnap M, Dursun H et al. Traumatic spinal cord injuries in Turkey: a nationwide epidemiological study. Spinal Cord 2000; 38: 697–701.
Burke DA, Linden RD, Zhang YP, Maiste AC, Shields CB . Incidence rates and populations at risk for spinal cord injury: a regional study. Spinal Cord 2001; 39: 274–278.
Otom AS, Doughan AM, Kawar JS, Hattar EZ . Traumatic spinal cord injuries in Jordan, an epidemiological study. Spinal Cord 1997; 35: 253–255.
Karamehmetoǧlu SS, Nas K, Karacan I, Sarac AJ, Koyuncu H, Ataolu S et al. Traumatic spinal cord injuries in Southeast Turkey: an epidemiological study. Spinal Cord 1997; 35: 531–533.
Lin KH, Chuang CC, Kao MJ, Lien IN, Tsauo JY . Quality of life of spinal cord injured patients in Taiwan: subgroup study. Spinal Cord 1997; 35: 841–849.
Chen CF, Lien IN . Spinal cord injuries in Taipei, Taiwan, 1978–1981. Paraplegia 1985; 23: 364–370.
Katoh S, Shingu H, Ikata T, Iwatsubo E . Sports-related spinal cord injury in Japan (from the nationwide spinal cord injury registry between 1990–1992). Spinal Cord 1996; 34: 416–421.
Shingu H, Ohama M, Ikata T, Katoh S, Akatsu T . A nationwide epidemiological survey of spinal cord injuries in Japan from January 1990 to December 1992. Paraplegia 1995; 33: 183–188.
Maharaj JC . Epidemiology of spinal cord paralysis in Fiji: 1985–1994. Spinal cord 1996; 34: 549–599.
Pajareya K . Traumatic spinal cord injuries in Thailand: an epidemiological study in Siriraj hospital, 1989–1994. Spinal Cord 1996; 34: 608–610.
Blumer CE, Quine S . Surveillance of traumatic spinal cord injury in Australia: the identification of information need. Spinal Cord 1996; 34: 639–643.
Walsh J . Costs of spinal cord injury in Australia. Paraplegia 1988; 26: 380–388.
Fine PR, Kuhlemeier KV, De Vivo MJ, Stover S . Spinal cord injury: an epidemiological perspective. Paraplegia 1979; 17: 237–250.
Ergas Z . Spinal cord injury in the United States: a statistical update. Central Nerv Syst Trauma 1986; 2: 19–30.
Kraus JF, Franti CE, Riggins RS, Richards D, Borhani NO . Incidence of traumatic spinal cord lesions. J Chronic Dis 1975; 28: 471–492.
Bracken MB, Freeman DH, Hellenbrand K . Incidence of acute spinal cord injury in the United States, 1970–1977. Am J Epidemiol 1981; 113: 615–622.
Silberstein B, Rabinovich S . Epidemiology of spinal cord injury in Novosibirsk, Russia. Paraplegia 1995; 33: 322–325.
Karamehmetoǧlu SS, Ûnal Ş, Kaeacanǐ Iˇ, Yǐmaz H, Iogay HŞ, Ertekin M et al. Traumatic spinal cord injuries in Istanbul, Turkey. An epidemiological study. Paraplegia 1995; 33: 469–471.
Hart C, Williams E . Epidemiology of spinal cord injuries: a reflection of changes in South African society. Paraplegia 1994; 32: 709–714.
Soopramanien A . Epidemiology of spinal injury in Romania. Paraplegia 1994; 32: 715–722.
Schönherr MC, Groothoff JM, Mulder GA, Eisma WH . Rehabilitation of patients with spinal cord lesions in the Netherlands: an epidemiological study. Spinal Cord 1996; 34: 679–683.
Larsfargues JE, Custis D, Morrone F, Carswell J, Nguyen T . A model for estimating spinal cord injury prevalence in the United States. Spinal Cord 1995; 33: 94–97.
Data refer to the year 2010, World economic outlook database-April 2010, International Monetary Fund (accessed 24 April 2010) http://www.imf.org/external/pubs/ft/weo/2010/01/weodata/index.aspx.
Acknowledgements
We would like to thank all Beijing hospitals that allowed us access to patient data, the Department of Mathematics, the Capital University of Medical Sciences for designing the sampling and the Information Centre of Beijing Health Bureau for assisting in organising the survey. We would also like to thank Y Hong, J Ji, S Li, C Zhao, Y Dong, Y Fang, P Tan, T Zhou and A Thang for participating in this survey. This work was sponsored by the China Foundation for Disabled Persons, Coloplast.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article
Cite this article
Li, J., Liu, G., Zheng, Y. et al. The epidemiological survey of acute traumatic spinal cord injury (ATSCI) of 2002 in Beijing municipality. Spinal Cord 49, 777–782 (2011). https://doi.org/10.1038/sc.2011.8
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2011.8
Keywords
This article is cited by
-
Long-term trends and risk factors of tracheostomy and decannulation in patients with cervical spinal cord Injury
Spinal Cord (2024)
-
Epidemiological features of traumatic spinal cord injury in Wuhan, China
Journal of Orthopaedic Surgery and Research (2023)
-
Spinal cord injury: molecular mechanisms and therapeutic interventions
Signal Transduction and Targeted Therapy (2023)
-
Urinary tract infections and intermittent catheterization among patients with spinal cord injury in Chinese community
Scientific Reports (2023)
-
Paeonol regulates NLRP3 inflammasomes and pyroptosis to alleviate spinal cord injury of rat
BMC Neuroscience (2022)
