
Abstract
Study design
Retrospective study.
Objectives
To investigate the epidemiological changes in persons with traumatic spinal cord injury (TSCI) over the past 7 years in Beijing Bo’ai Hospital, China Rehabilitation Research Center, China.
Setting
Beijing Bo’ai Hospital, China Rehabilitation Research Center (CRRC).
Methods
A database containing the records of all persons treated with SCI from 1 January 2013 to 31 December 2019 was reviewed. Variables including demographic and clinical data were analysed. Comparisons were made with data previously published in 2002.
Results
During the study period, 2448 persons with recent TSCI were included in the analysis. The mean age at the time of injury increased from 38.1 years to 40.2 years (P = 0.025). The percentage of elderly persons increased (8.8–14.6%, P = 0.036) and was higher than that in 2002. The percentage of retirees increased. Transport related injuries were the leading cause of injury and the percentage of TSCI due to low falls increased 6%. Low falls were the most common cause for elderly persons (y ≥ 60) and were even higher for elderly women. Persons with cervical injuries increased compared to the 2002-data (44.1% vs 4.9%). The percentage of persons with incomplete SCI increased significantly over the study duration.
Conclusions
Persons with TSCI are becoming older, and the percentage of elderly persons is increasing year by year. These changes are likely due to a combination of population ageing in the region and changes in aetiology, with corresponding changes including an increase in persons with cervical TSCI and persons with incomplete injury.
Similar content being viewed by others

Introduction
The ageing population is now a global issue, with global epidemiological surveys showing that the mean age of persons with recent TSCI is increasing, especially in developed countries [1,2,3,4]. In contrast to data from developed countries, a systematic review showed that the mean age of persons with recent TSCI in developing countries was 32.4 years [5].
TSCI in elderly persons appears to be different from that in young people in terms of the common causes, level and severity of injury, treatment strategies and prognosis of recovery. Timely and adequate awareness of this new change is essential for implementing better prevention strategies, estimating the number of persons affected and allocating health care resources effectively. Furthermore, it is increasingly being addressed by researchers in the countries concerned [6, 7].
China is now the world’s largest developing country, and with rapid economic development, the number of privately owned vehicles and the total length of the road network have increased dramatically, leading to a significant increase in traffic accidents and injuries. In addition, large scale urban construction and increased industrial production have contributed to the occurrence of many accidental injuries [8]. At the same time, China is already a country with an ageing society, and its ageing population accounts for 1/5 of the global elderly population [9]. China has a large number of persons with spinal cord injury (SCI), but due to the lack of a national registration system, the problems and needs of persons with TSCI are largely unknown, with the small number of reported data varying widely from region to region [10].
Beijing is one of China’s most economically developed and ageing regions. In 2018, the city’s mean life expectancy reached 82.20 years, and in 2019, the permanent population reached 21.536 million, with 17.2% of the population being older than 60 years of age [11]. With rapid economic development and an ageing population, the epidemiological profile of persons with TSCI in Beijing is likely to change even more rapidly than in the past. Our research team previously reported on the local epidemiology of persons with TSCI in 2002 [12], and to the best of our knowledge, there have been no published studies on the changing demographics of TSCI in the Beijing area since then. Therefore, the aim of this study was to investigate the epidemiological changes in persons with TSCI at a regional SCI center in Beijing, China, over the past 7 years, to capture and analyse their characteristics. Referring to the other national and regional studies mentioned above, we assume that the mean age of persons and the percentage of elderly persons increase year by year.
Methods
As a grade-A first-class general hospital in China specialising in rehabilitation, our hospital is a designated hospital for medical insurance and industrial injury insurance. In addition, an all-in-one service chain has been established, covering disability prevention, treatment at the acute stage, early intervention, rehabilitation at the middle and late stages, and community and family self-reliance. Our hospital is also one of the priority referral hospitals for SCI rehabilitation in the region, and persons with both traumatic and non-traumatic SCI can be referred to us after acute phase treatment.
A database containing the records of all persons with SCI treated from 1 January 2013 to 31 December 2019 in our hospital was reviewed. TSCI has been defined as the impairment of the spinal cord or cauda equina function resulting from the application of an external force of any magnitude [13]. The exclusion criteria were as follows: (1) SCI with non-traumatic causes; (2) hospital visits for re-examination or other treatments (such as pressure ulcers, spasm, neuropathic pain); and (3) incomplete medical records or medical records with uncertain diagnoses. Approval from the hospital ethics committee was obtained before commencing the study (No. CRRC-IEC-RF-SC-005-01).
In data collection, the variables mainly referred to the International SCI Core Data Set, as recommended by Biering-Sorensen et al. [13]. The variables included sex, age, occupation, marital status, aetiology, the presence of vertebral fractures and associated injuries, whether spinal surgery was performed, ventilator dependence at discharge, and the neurological level and severity of injury. Assessment of neurological severity was performed according to the International Standards for Neurological Classification of SCI [14]. Marital status was categorised as married, unmarried, or other (divorced and widowed). Injuries caused by falls were specifically classified as low falls (from a height <1 m) or high falls (from a height of 1 m or more). The types of associated injuries were selected from the International SCI Core Data Set [13]. Elderly persons were persons aged ≥60 years.
The demographic and clinical characteristics of the participants in this study were compared with data from our previous study in 2002 [12].
All of the data were gathered in a Microsoft Excel spreadsheet (Redmond, WA, USA) by three researchers and then cross-checked twice to ensure information accuracy. Statistical analyses were performed using IBM SPSS Statistics software, version 26.0 for Mac (IBM, Armonk, NY, USA). Continuous variables are expressed as the means with standard deviations. Categorical variables are expressed as the numbers of cases and percentages. The mean age for each year was compared with the Kruskal–Wallis H test for several independent samples. The chi-square trend test was used to compare the annual changes in the number of hospitalised elderly persons or other groups. Differences with 2002 data and differences between elderly persons by sex were assessed by the chi-square test. The Kruskal–Wallis H test for several independent samples was applied for between-different age comparisons for aetiology and the level and severity of injury. Statistical significance was set at P < 0.05.
Results
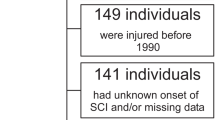
During the study period, 2448 persons with recent TSCI were finally included in the analysis and 888 cases were excluded for various reasons (Fig. 1).

Of the 3336 patients with SCI, 2896 had TSCI, and then after screening and exclusion, information from 2448 patients was included in the final analysis.
Characteristics of the study population
The mean (SD) age was 39.1 (±16.7) years, up from 38.1 (±15.9) years in 2013 to 40.2 (±19.1) years in 2019 (H = 14.413, P = 0.025) (Table 1). The gradual increase in age was observed for both sexes, with a significant increase in men (H = 23.870, P = 0.001). The gradual increase in age was also observed in the transport and high falls groups, with a significant increase in the transport group (H = 13.645, P = 0.034) (Table 2).
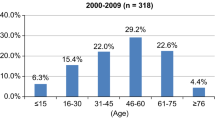
A total of 271 elderly persons were admitted to the hospital, and the percentage of elderly persons increased significantly over the study duration (χ2 = 13.481, P = 0.036), from 8.8% in 2013 to 14.6% in 2019. Of these cases, the percentage of elderly persons in 2018 and 2019 was already higher than in 2002 (χ2 = 4.094, P = 0.043; χ2 = 1.705, P = 0.192). Inspired by the study by Thompson et al. [2], we calculated that the percentage of persons ≥55 years increased from 16% in 2013 to 28.3% in 2019.
Despite the predominance of men in all years, the percentage of women increased gradually, from 22.5% in 2013 to 29.1% in 2018 (Table 1). Persons younger than 15 years were mainly females, while other age groups were mainly males (Fig. 2).

The proportion of females was highest among persons younger than 15 years of age; it declined, reaching a minimum at 45–59 years of age and then slightly increased again.
We observed that the percentage of workers and farmers decreased and was significantly less than in the 2002 data (χ2 = 754.810, P < 0.001), while the percentage of retirees increased. The percentage of married persons with TSCI increased, peaked in 2016, and then declined. With the increasing mean age, we observed an increasing percentage of people who were divorced or widowed (Table 1), while a gradual decrease in percentage was observed among persons with vertebral injury, spinal surgery and associated severe injuries (See Supplementary Table S1 for clinical characteristics of persons with recent TSCI).
Aetiology
Compared to 2002 (χ2 = 149.163, P < 0.001), high falls were no longer the leading cause of injury and had been replaced by transport (30.8%), but the percentage of both high falls and transport declined, while the percentage of low falls increased from 9.6% in 2013 to 15.5% in 2019 (See Supplementary Table S1 for clinical characteristics of persons with recent TSCI).
The frequency distributions for the causes of injury differed significantly among age groups (H = 227.097, P < 0.001) (Fig. 3). As shown in Fig. 3, with increasing age, persons with SCI caused by low falls gradually increased. As expected, low falls were the most common cause for persons aged 60 years and older (44.3%), followed by transport (26.2%). In contrast, for those younger than 60 years of age, the most common cause was transport (31.4%), followed by high falls (30.4%). In addition, in this study, sports and leisure were the most common causes of injury in the populations aged 14 years and younger (55.9%).

Persons younger than 15 years had mainly sports and leisure injuries, those aged 15–59 years had mainly transport or high fall injuries and those older than 60 years were mainly low fall injuries (black line).
Traffic accidents were the most common cause in female persons. In total, 28.6% of persons who suffered a TSCI due to transport were female compared with 22.9% for all other aetiologies. However, the most common cause of injuries in elderly women was low falls, and the percentage was even higher than in elderly men (48.4% vs 43.1%) (see Supplementary Table S2 for clinical characteristics of persons with recent TSCI among men and women in the elderly group).
Level and severity of injury
In all, 44.1% of persons with TSCI suffered a cervical injury, which increased significantly compared to 4.9% in 2002 (χ2 = 7980.190, P < 0.001). This increase can be attributed mainly to an increase in C1–C4 injuries, from 65% of all persons with cervical TSCI in 2013 to 70.3% in 2019. The frequency distributions for the levels of injury differed significantly among age groups (H = 305.567, P < 0.001) (see Supplementary Fig. S1 for distribution line chart for injury level according to age). As shown in Supplementary Fig. S1, the number of persons with tetraplegia gradually increased with age. The most common level of injury in elderly persons was C1–C8 (74.5%), while T1-S5 injury was more common in persons younger than 60 years of age (59.6%). From Supplementary Table S2, it can be further seen that the percentage of C1–4 injury in elderly men gradually increased. Although C1–4 injury was also very common in elderly women, the percentage of T1-S5 injury was much higher than in elderly men (χ2 = 13.858, P < 0.001).
The percentage of persons with incomplete SCI (AIS B, C and D) increased significantly over the study duration, from 47.8% in 2013 to 56% in 2018 (χ2 = 14.395, P = 0.026). The frequency distributions for the severity of injury differed significantly among age groups (H = 173.445, P < 0.001) (see Supplementary Fig. S2 for distribution line chart for severity of injury according to age). As shown in Supplementary Fig. S2, the number of persons with incomplete SCI gradually increased with age. Complete injury (AIS A) accounted for 51.2% of persons younger than 60 years of age, while incomplete injury accounted for more, 78.6%, in elderly persons. Supplementary Table S2 shows that the percentage of elderly men with incomplete SCI increased year by year, but no such change was found among elderly women.
Discussion
The results of this study showed that there was a significant increase in the mean age of persons with recent TSCI during the study period. The gradual increase in age was observed for both sexes and in the transport and high falls groups (these two groups were the most common causes of injury, together accounting for more than 50%). More importantly, we found that the percentage of elderly persons increased dramatically from 8.8% in 2013 to 14.6% in 2019. This increase even tended to accelerate year by year. In 2019, we had a ward renovation; thus, there was a reduction in admissions, but the percentage of elderly persons was still very high. In addition, the percentage of persons aged 55 years and older reached 28.3% in 2019. These findings clearly confirm our hypothesis regarding the changes of an increased mean age of persons with TSCI and the percentage of elderly persons, which reflect population ageing in the region.
The mean age at time of injury was 39.1 years, which is still low compared to the mean age in developed countries such as the United States (42.2 years) [1], Norway (47 years) [4], Spain (48 years) [3] and Italy (54 years) [15]; however, our result is among the highest among developing countries [5]. This result is less than the mean age of participants in the 2002 multicentre study in Beijing (41 years) [12] and lower than the mean age of persons in a single-centre study in Tianjin (50 years), another neighbouring city [16]. The number of children with TSCI in the Tianjin single-centre study was significantly lower than that in our study, which our analysis suggests might have been due to the well-known treatment of paediatric SCI in our hospital, which attracts some paediatric SCI patients from other provinces and cities.
In addition to the increase in the mean age and the percentage of elderly persons, our study found that the aetiologies also showed some significant changes. Compared to our previous study (Supplementary Table S1), transport became the leading cause of injury, followed by high falls, but both were on the decline. The percentage of low falls increased from 9.6% in 2013 to 15.5% in 2019, while this aetiology accounted for only 8.3% in 2002. Our study showed that the percentage of workers and farmers decreased and was significantly lower than that in the 2002 data. Moreover, the percentage of retirees increased (Table 1). Despite the predominance of male persons in all years, the percentage of female persons increased gradually. The change in marital status is an important indicator, which is influenced in part by the ageing of the TSCI population. A previous study showed that married persons with SCI had better rehabilitation training outcomes and positive influences on the application of family and social life [17].
The increasing number of cars, new drivers and poorly designed roads as well as the lack of separation between pedestrians and motor vehicles have led to a large number of traffic accidents in China [18]. A study of the demand for pre-hospital emergency calls in Beijing found that traffic incidents and falls accounted for half of all trauma-related demands and were growing rapidly [19]. The decline in the percentage of high fall injuries could be related to the continuous improvement of the safety production system in recent years, as well as increasing attention from the public and the government. It might also be related to the gradual decrease in large-scale construction projects once economic development reached a certain stage. Since high falls were mainly associated with young male workers, these changes may not only led to an increase in the mean age but also influenced the occupational and sex characteristics of persons with TSCI. China has become an ageing society, and Beijing, the capital of China, has become an ageing city [20], which could lead to an increase in the number of low falls among the elderly. One local study showed that the use of emergency medical services for low falls increased from 7.12% to 9.45% as the percentage of the elderly population increased between 2010 and 2017 [21]. This is true for elderly persons of both sexes, and our study showed that percentage of low falls was even higher for elderly women (Supplementary Table S2). In addition, our study showed a high percentage of elderly persons with TSCI due to traffic accidents, which could have been due to the high rate of non-motor vehicle accidents in recent years (such as those involving bicycles, tricycles, electric bicycles, electric wheelchairs for disabled people and power vehicles) [22]; thus, more attention is needed to address this problem. Notably, for the paediatric persons in our study, the aetiology was mainly sports and leisure (55.9%), with many cases being due to dance practice. These cases could constitute a specific type of SCI that is rarely seen in other countries and further research is needed because the mechanism of injury remains unclear [23]. Largely due to this factor, our study showed a high percentage of female persons aged 0–14 years (Fig. 2).
In all, 44.1% of persons with TSCI in our study suffered in a cervical injury, which was a significant increase compared to 4.9% in 2002. This increase can be mainly attributed to an increase in C1–C4 injury. For a variety of reasons, the severity of neurological impairment was not collected or analysed in the 2002 study, although this variable was supplemented for our paper. The results showed that the percentage of persons with incomplete SCI increased significantly over the study duration. In marked contrast to young people, elderly persons were predominantly tetraplegic, and most had incomplete injuries (Supplementary Figs. S1 and S2). Our data showed that elderly women had significantly higher rates of paraplegia than elderly men. Elderly persons with TSCI are often caused by minor trauma based on spinal degeneration. Wu et al. [24] analysed 22,951 hospitalised persons with spinal degenerative diseases from 2008 to 2014 at a leading orthopaedic hospital in the region. The results showed that there was a higher percentage of male persons(P < 0.001) younger than 45 years with lumbar degenerative spinal diseases(LDD); however, in persons who were older than 45 years and had LDDs, a higher percentage was female (P < 0.05). The exact causes of this phenomenon remain unclear. Possibly related to these factors, there was a gradual decrease in persons with vertebral injury, spinal surgery and associated severe injuries.
Although the majority of elderly persons with TSCI suffer incomplete injuries, most cases involve central cord syndrome, and these persons have poor upper limb and hand function; thus, their ability to live on their own is significantly limited [25]. In addition, elderly persons are more likely to develop complications, have limited physiological reserves to overcome traumatic injury and have an increased risk of death [26]. These new situations will undoubtedly pose an increasing challenge to spine surgery and rehabilitation physicians and related institutions. Since the majority of elderly persons have incomplete spinal cord injuries and are expected to regain good function, striving for the ideal treatment for this group could have a significant impact on prognosis. For example, Ahn et al. [6] found that even after researchers adjusted for influencing factors such as injury severity, neurological level and trauma severity, diagnosis and time to surgery remained delayed in elderly persons. Additionally, Inoue et al. [27] showed that delaying surgery solely because of advanced age, fear of complications and other factors did not seem desirable. Truchon et al. [28] found that the amount of rehabilitation therapy was positively associated with the change in motor function in a nonlinear fashion in persons with TSCI and that raising the amount of therapy received through an increase in therapy intensity could lead to reduced resource utilisation and increase cost savings. These findings could be useful in our daily medical practice.
Given the large sample size, we were able to examine changes in detail by cross-tabulating several demographic and injury factors. Furthermore, the categorical variables in this study refer to the International SCI Core Data Set, as recommended. The chief limitation of the current study was the potential for selection bias implicit to a single-centre analysis. This study might not reflect the actual situation of persons with TSCI in Beijing; thus, it is impossible to estimate the regional incidence of persons with TSCI. Data from the Second National Sample Survey of Disability and the 2006–2016 Statistical Bulletin on the Development of People with disabilities in China showed that 41.46% of persons with disabilities do not receive any rehabilitation services [29]. In addition, family models play a dominant role in the life of the elderly in Beijing [30], and many families believe that elderly persons with SCI only require care. Thus, it is true that there is a proportion of elderly persons with TSCI who do not receive rehabilitation or who are referred to other, non-specialised rehabilitation centres. Because our institution is regionally recognised as a referral centre for persons with SCI, our findings, as mentioned earlier, might overestimate the percentage of persons with severe injuries and surgical treatments and underestimate the percentage of elderly persons.
In conclusion, this paper enhances our understanding of the regionally changing epidemiological characteristics of persons with TSCI through a retrospective survey of a large number of persons. The results of the study confirm our hypothesis that persons with TSCI are ageing and the percentage of elderly persons increases year by year. These changes are likely due to a combination of population ageing in the region and changes in the aetiology of TSCI, with corresponding changes including an increase in persons with cervical TSCI and persons with incomplete injury. Based on the findings of this study, we strongly recommend that a new multicentre prospective epidemiological survey of persons with TSCI in the region be initiated as soon as possible to calculate the latest incidence rate and better assess the injury characteristics in this new situation. At the same time, we should promote campaigns for the prevention of low falls, particularly among elderly persons, and explore better treatment and rehabilitation options based on their unique pathophysiology.
References
Chen Y, He Y, DeVivo MJ. Changing demographics and injury profile of new traumatic spinal cord injuries in the United States, 1972–2014. Arch Phys Med Rehabil. 2016;97:1610–9.
Thompson C, Mutch J, Parent S, Mac-Thiong JM. The changing demographics of traumatic spinal cord injury: an 11-year study of 831 patients. J Spinal Cord Med. 2015;38:214–23.
Barbara-Bataller E, Mendez-Suarez JL, Aleman-Sanchez C, Sanchez-Enriquez J, Sosa-Henriquez M. Change in the profile of traumatic spinal cord injury over 15 years in Spain. Scand J Trauma Resusc Emerg Med. 2018;26:27.
Halvorsen A, Pettersen AL, Nilsen SM, Halle KK, Schaanning EE, Rekand T. Epidemiology of traumatic spinal cord injury in Norway in 2012–2016: a registry-based cross-sectional study. Spinal Cord. 2019;57:331–8.
Rahimi-Movaghar V, Sayyah MK, Akbari H, Khorramirouz R, Rasouli MR, Moradi-Lakeh M, et al. Epidemiology of traumatic spinal cord injury in developing countries: a systematic review. Neuroepidemiology 2013;41:65–85.
Ahn H, Bailey CS, Rivers CS, Noonan VK, Tsai EC, Fourney DR, et al. Effect of older age on treatment decisions and outcomes among patients with traumatic spinal cord injury. CMAJ. 2015;187:873–80.
Kudo D, Miyakoshi N, Hongo M, Kasukawa Y, Ishikawa Y, Ishikawa N, et al. An epidemiological study of traumatic spinal cord injuries in the fastest aging area in Japan. Spinal Cord. 2019;57:509–15.
Yin XF, Wang TB, Zhang PX, Kou YH, Zhang DY, Yu K, et al. Evaluation of the effects of standard rescue procedure on severe trauma treatment in china. Chin Med J. 2015;128:1301–5.
China-WHO. Country cooperation strategy 2016–2020. https://iris.wpro.who.int/handle/10665.1/13088, Accessed 14 April 2020.
Yuan S, Shi Z, Cao F, Li J, Feng S. Epidemiological features of spinal cord injury in China: a systematic review. Front Neurol. 2018;9:683.
http://www.phic.org.cn/tjsj/, Accessed 14 April 2020.
Li J, Liu G, Zheng Y, Hao C, Zhang Y, Wei B, et al. The epidemiological survey of acute traumatic spinal cord injury (ATSCI) of 2002 in Beijing municipality. Spinal Cord. 2011;49:777–82.
Biering-Sorensen F, DeVivo MJ, Charlifue S, Chen Y, New PW, Noonan V, et al. International Spinal Cord Injury Core Data Set (version 2.0)-including standardization of reporting. Spinal Cord. 2017;55:759–64.
Waring WP III, Biering-Sorensen F, Burns S, Donovan W, Graves D, Jha A, et al. Review and revisions of the international standards for the neurological classification of spinal cord injury. J Spinal Cord Med. 2009;2010(33):346–52.
Ferro S, Cecconi L, Bonavita J, Pagliacci MC, Biggeri A, Franceschini M. Incidence of traumatic spinal cord injury in Italy during 2013-2014: a population-based study. Spinal Cord. 2017;55:1103–7.
Zhou Y, Wang XB, Kan SL, Ning GZ, Li YL, Yang B, et al. Traumatic spinal cord injury in Tianjin, China: a single-center report of 354 cases. Spinal Cord. 2016;54:670–4.
Xie H, Chang F, Shen C, Shen X, Zhang J, Lin P, et al. Factors influencing the outcomes of specialized institution-based rehabilitation in spinal cord injury.Chinese. J Spine Spinal Cord. 2018;28:529–34.
Wang T, Yin X, Zhang P, Kou Y, Jiang B. Road traffic injury and rescue system in China. Lancet. 2015;385:1622.
Wang T, Zhang J, Wang F, Liu H, Yin X, Zhang P, et al. Changes and trends of pre-hospital emergency disease spectrum in Beijing in 2003–12: a retrospective study. Lancet. 2015;386:S39.
Chen Z, Yu J, Song Y, Chui D. Aging Beijing: challenges and strategies of health care for the elderly. Ageing Res Rev. 2010;9(Suppl 1):S2–S5.
Zhao S, Cao Y, Lei Y, Liu F, Shao S, Liu J, et al. Population ageing and injurious falls among one million elderly people who used emergency medical services from 2010 to 2017 in Beijing, China: a longitudinal observational study. BMJ Open. 2019;9:e028292.
Wang X, Yu H, Nie C, Zhou Y, Wang H, Shi X. Road traffic injuries in China from 2007 to 2016: the epidemiological characteristics, trends and influencing factors. PeerJ. 2019;7:e7423.
Pang D. Editorial comment to article: Pediatric thoracic SCIWORA after back bend during dance practice: a retrospective case series and analysis of trauma mechanisms. Childs Nerv Syst. 2017;33:1199.
Wu Y, Liu Z, Liu X, Sun Y, Chen Z, Dang G. An analysis of social characteristics of hospitalized spinal degenerative disease patients in the orthopedic department of Peking University Third Hospital during a period of 2008 to 2014. Chinese. J Spine Spinal Cord. 2016;26:70–76.
Shigematsu H, Cheung JP, Mak KC, Bruzzone M, Luk KD. Cervical spinal canal stenosis first presenting after spinal cord injury due to minor trauma: an insight into the value of preventive decompression. J Orthop Sci. 2017;22:22–26.
Fassett DR, Harrop JS, Maltenfort M, Jeyamohan SB, Ratliff JD, Anderson DG, et al. Mortality rates in geriatric patients with spinal cord injuries. J Neurosurg Spine. 2007;7:277–81.
Inoue T, Suzuki S, Endo T, Uenohara H, Tominaga T. Efficacy of early surgery for neurological improvement in spinal cord injury without radiographic evidence of trauma in the elderly. World Neurosurg. 2017;105:790–5.
Truchon C, Fallah N, Santos A, Vachon J, Noonan VK, Cheng CL. Impact of therapy on recovery during rehabilitation in patients with traumatic spinal cord injury. J Neurotrauma. 2017;34:2901–9.
Lu D. Current situation and demand analysis of rehabilitation personnel by stratified sampling. Chin J Rehabil Theory Pract. 2019;25:859–64.
Zhang Q, Zhang D. Study on select of pension methods of the elderly and its influencing factors in Beijing. Res Econ Manag. 2014;35:102–6.
Acknowledgements
We are deeply grateful to Pengkun Li of medical record statistics room for his assistance of collection data.
Funding
This study was supported by grants from China Rehabilitation Research Center (No. 2019ZX-04); National Key Research and Development Program (No. 2018YFF0301104).
Author information
Authors and Affiliations
Contributions
HL was responsible for convening researchers, collecting, aggregating and analysing data, interpreting results and writing the report. JL and MS were responsible for collecting and analysing data. XY was responsible for the statistical analysis and graphing. LD and MY contributed to the design of the study protocol and interpreting results. JL and FG contributed to writing the report, providing important references and interpreting results. JL was responsible for designing and writing the study protocol and interpreting results. He is the corresponding author. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Statement of ethics
Approval from the hospital ethics committee was obtained before commencing the study (No. CRRC-IEC-RF-SC-005-01).
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Liu, H., Liu, J., Shen, M. et al. The changing demographics of traumatic spinal cord injury in Beijing, China: a single-centre report of 2448 cases over 7 years. Spinal Cord 59, 298–305 (2021). https://doi.org/10.1038/s41393-020-00564-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-020-00564-7
This article is cited by
-
Long-term trends and risk factors of tracheostomy and decannulation in patients with cervical spinal cord Injury
Spinal Cord (2024)
-
The impact of COVID-19 and associated lockdowns on traumatic spinal cord injury incidence: a population based study
Spinal Cord (2024)
-
The trends in sports-related spinal cord injury in China
Spinal Cord (2023)
-
Incidence, prevalence and disability of spinal cord injury in China from 1990 to 2019: a systematic analysis of the Global Burden of Disease Study 2019
European Spine Journal (2023)
-
A systematic review and meta-analysis of the global epidemiology of pediatric traumatic spinal cord injuries
European Journal of Pediatrics (2023)
