
Abstract
Colorectal liver metastases (CRLM) are the predominant factor limiting survival in patients with colorectal cancer and liver resection with complete tumor removal is the best treatment option for these patients. This study examines the predictive ability of three-dimensional lung volumetry (3DLV) based on preoperative computerized tomography (CT), to predict postoperative pulmonary complications in patients undergoing major liver resection for CRLM. Patients undergoing major curative liver resection for CRLM between 2010 and 2021 with a preoperative CT scan of the thorax within 6 weeks of surgery, were included. Total lung volume (TLV) was calculated using volumetry software 3D-Slicer version 4.11.20210226 including Chest Imaging Platform extension (http://www.slicer.org). The area under the curve (AUC) of a receiver-operating characteristic analysis was used to define a cut-off value of TLV, for predicting the occurrence of postoperative respiratory complications. Differences between patients with TLV below and above the cut-off were examined with Chi-square or Fisher’s exact test and Mann–Whitney U tests and logistic regression was used to determine independent risk factors for the development of respiratory complications. A total of 123 patients were included, of which 35 (29%) developed respiratory complications. A predictive ability of TLV regarding respiratory complications was shown (AUC 0.62, p = 0.036) and a cut-off value of 4500 cm3 was defined. Patients with TLV < 4500 cm3 were shown to suffer from significantly higher rates of respiratory complications (44% vs. 21%, p = 0.007) compared to the rest. Logistic regression analysis identified TLV < 4500 cm3 as an independent predictor for the occurrence of respiratory complications (odds ratio 3.777, 95% confidence intervals 1.488–9.588, p = 0.005). Preoperative 3DLV is a viable technique for prediction of postoperative pulmonary complications in patients undergoing major liver resection for CRLM. More studies in larger cohorts are necessary to further evaluate this technique.
Similar content being viewed by others

Introduction
Colorectal cancer (CRC) is the third most common cancer worldwide and colorectal liver metastases (CRLM) can affect up to 80% of patients with CRC1,2. The best option for cure or long-term survival in patients with CRLM is liver resection with complete tumor removal. This may be carried out directly in cases of primarily resectable disease (approximately 30%), or after tumor downsizing through systemic chemotherapy3,4.
Patients with CRLM often require multimodal treatment approaches, which may include perioperative chemotherapy, local ablative techniques, portal vein embolization (PVE), and staged resections, including Associating Liver Partition and Portal vein ligation for Staged hepatectomy (ALPPS)1,3,5. Patients requiring major liver resection for CRLM are at increased risk of perioperative morbidity and mortality, despite technical advances and high experience of specialized centers6. Previous attempts have been made to develop scores and algorithms, which can identify patients at risk for high morbidity and mortality following liver surgery7,8,9. Postoperative pulmonary complications, in particular, are a major cause of mortality and morbidity and accountable for longer intensive care unit (ICU) stays after liver surgery10. Furthermore, due to an increase in overall life expectancy, more elderly patients undergo major liver resection11, which is associated with increased rate of pulmonary complications10. Therefore, the ability to identify patients at risk for postoperative pulmonary complications is of great clinical relevance.
Three-dimensional lung volumetry (3DLV) based on computerized tomography (CT) is a novel technique, which can be performed on routine staging CT scans of the thorax. It provides a technically stable estimation of lung volume12, which is well-correlated with spirometric measurements of total lung capacity13. The capability of 3DLV to reliably predict postoperative pulmonary function has been previously established in thoracic surgery13,14,15,16. In a novel approach, the aim of this study was to examine the ability of preoperative 3DLV to predict postoperative respiratory complications, postoperative overall morbidity, and length of ICU- and hospital stay after major curative liver resection for CRLM.
Methods
Patient cohort and inclusion criteria
Consecutive adult patients undergoing elective major liver resection for CRLM at the University Hospital RWTH Aachen (UH-RWTH) between 2010 and 2021, with a preoperative CT of the thorax within 6 weeks of operation, were eligible for inclusion in this retrospective study. Liver resections were described according to the Brisbane classification17 and defined as major, when ≥ 3 segments were resected. Patients were excluded, if they underwent resections of hepatic metastatic recurrence, or exploration without resection. Patients with inadequate quality of the thorax CT (for example, where lungs were not completely captured) or evidence of active lung disease, were also excluded.
The primary endpoint of the study was the incidence of postoperative respiratory complications within 90 days of operation, defined as the occurrence of any of the following: respiratory failure, pulmonary embolism, pneumonia, pleural empyema, pleural effusion requiring thoracentesis and pneumothorax necessitating thoracic drainage. Further perioperative outcomes, such as cumulative morbidity defined by the Comprehensive Complication Index (CCI)18 and major complications according to the Clavien-Dindo score (CD ≥ 3)19, as well as length of intensive care unit (ICU)- and hospital stay were examined as secondary endpoints.
Data collection
Clinical data were recovered from a prospective institutional database and analyzed retrospectively. These included demographic information such as body mass index (BMI) and American Society of Anesthesiology (ASA) score, radio-oncological staging, and treatment strategies. Primary tumors located in the cecum to transverse colon were categorized as right-sided, whereas tumors located from the splenic flexure to rectum as left-sided. Histological staging of the primary tumor was documented according to the Union for International Cancer Control (UICC) tumor/lymph node/metastasis system (TNM). Kirsten rat sarcoma viral oncogene homolog (KRAS) mutation status was obtained from histological analysis of either the primary tumor or CRLM (with mutated status overriding wildtype in any configuration). Synchronous metastases were defined as those being diagnosed simultaneously or within 3 months of the primary tumor. The number, size, and location of CRLM were obtained from preoperative computerized tomography (CT) and corroborated with liver-protocol magnetic resonance imaging (MRI), where available9. Preoperative chemotherapy was defined as any systemic treatment administered within six months before surgery. Radicality of resection (denoted R0 for radical, otherwise R+) was determined by postoperative pathological analysis. Postoperative extubation point was recorded as either in the operating room or on ICU9. Respiratory complications were diagnosed commonly by X-ray or CT.
Routine preoperative staging CT scans of the thorax, within 6 weeks of liver resection, were used for 3DLV measurements. Suitable scans were identified using electronic patient records and the hospital Picture Archiving and Communication System (PACS). Anonymized Digital Imaging and Communications in Medicine (DICOM) image series were exported for analysis and organized according to an identification number, matched to the patient data from our database. Exported series were loaded into the software 3D-Slicer version 4.11.20210226 including the Chest Imaging Platform extension (http://www.slicer.org). Axial, coronal, and sagittal views were used for the analysis. Manual marking was used to identify lung parenchyma and mapping of lung volume was carried out automatically. For this, lung volume was quantified using a predefined Hounsfield unit (HU) range of − 1000 HU to − 200 HU. Trachea and bronchial system volume was automatically removed by the software, whereas pneumatic intestinal loops and any errors from the automatic process were manually corrected. Figure 1 shows an example of a 3DLV.

Three-dimensional computer-tomography-based lung volumetry of a male patient. (A) axial view; (B) Three-dimensional model of the respiratory system; (C) coronal view; (D) sagittal view. Green shading: right lung; Yellow shading: left lung; Blue shading: trachea with main bronchi; Total lung volume calculated as the sum of the right and left lung volumes.
Operative technique
Operative technique adhered to common clinical standards for liver resection9. Intraoperative sonography confirmed preoperative imaging findings and ruled out new or undetected lesions. The Cavitron Ultrasonic Surgical Aspirator (CUSA®, Integra LifeSciences, Plainsboro NJ, USA) was used for parenchymal transection in open surgery, with clipping or ligation of vascular and biliary structures. In laparoscopic cases, either the THUNDERBEAT (Olympus K.K., Tokyo, Japan), HARMONIC ACE® (Ethicon Inc. Somerville, NJ, USA) or laparoscopic CUSA® (Integra LifeSciences, Plainsboro NJ, USA) devices were combined with ECHELON™ vascular staplers (Ethicon, Somerville, New Jersey, USA) or Weck® Hem-o-lok® polymer clips (Teleflex Inc., Pennsylvania, USA). Intermittent Pringle maneuvers were carried out as needed. Anatomical or parenchyma-sparing resections were carried out according to general patient condition, preoperative liver function tests, and limiting factors, such as macrovascular invasion. Radicality of tumor resection was controlled through frozen section. Anesthesiologic management aimed for a low central venous pressure (CVP) during the resection phase.
Statistical analysis
The Kolmogorov–Smirnov test was used to check data for normal distribution. Data were described as medians and interquartile range (IQR, given as 25th–75th percentiles) for non-normally distributed continuous variables, or absolute and relative frequencies for categorical and ordinal variables. To examine the predictive capability of 3DLV regarding respiratory complications, the area under the curve (AUC) of the receiver operating characteristic (ROC) analysis was calculated. Group comparisons were performed using the Chi-square test or Fisher’s exact test and the Mann–Whitney-U test. Uni- and multivariable binary logistic regression was used to determine independent risk factors for the development of respiratory complications and corresponding odds ratios (OR) were given with 95% confidence intervals (CI). Only p-values < 0.05 were considered statistically significant. Statistical analysis was performed using SPSS Statistics version 28.0.1.0 (IBM Corp., Armonk, NY, USA). Analysis was carried out using the whole cohort and repeated for subgroups of interest. These were: age above 60 years, BMI classification according to the World Health Organization (WHO)20, and patients undergoing ALPPS. The latter were examined separately, because of the increased complexity of the procedure and associated increased morbidity and mortality21.
Ethical approval
The study was conducted under the ethical approval of the Institutional Review Board of the RWTH Aachen University (EK-001/21) and in accordance with the current version of the Declaration of Helsinki, the Declaration of Istanbul, and good clinical practice guidelines (ICHGCP). Informed consent was waived due to the retrospective study design and collection of readily available clinical data.
Results
Patient characteristics
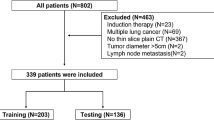
Between 2010 and 2021, 550 patients underwent curative liver resections for CRLM at the UH-RWTH. Of these, 243 received major resections, 124 of which had a CT scan of the thorax within 6 weeks before surgery. One patient was excluded, because the CT scan did not include the whole lung, resulting in a final cohort of 123 patients (Fig. 2). The median age of the study cohort was 62 years, and 59% of patients had an ASA score of ≥ III. Thirty-five (29%) patients developed respiratory complications, as there were: respiratory failure (11.4%), pulmonary embolism (8.6%), pneumonia (14.3%), pleural empyema (2.9%), pleural effusion requiring thoracentesis (74.3%) and pneumothorax necessitating thoracic drainage (17.1%) (sum is more 100% due to the fact that some patients had more than one complication. All patients with respiratory failure or pulmonary embolism required ICU or intermediate care (IMC) admission, and 100% of patients with pleural effusion or pneumothoraces underwent thoracentesis. The median TLV of the cohort was 4945 cm3, with a minimum TLV of 2492 cm3 and a maximum TLV of 8444 cm3. Patient characteristics of the whole study population are given in Table 1 and postoperative outcomes are described in Table 2.

Flowchart of inclusion and exclusion criteria, leading to the final study population. Abbreviations: CRLM, colorectal liver metastases; CT, Computerised Tomography.
ROC analysis
The ROC analysis demonstrated a predictive ability for TLV with regard to respiratory complications, with an AUC of 0.62 (p = 0.036), as shown in Fig. 3. Youden Index analysis was used to identify the ideal cut-off value for TLV, which was determined to be 4500 cm3 (Youden index, YI = 0.25). The cut-off was then used to divide the cohort into two groups. The median TLV were 3883 cm3 and 5419 cm3 in the groups below and above the cut-off, respectively. More male patients (74% vs. 27%, p < 0.001) and a higher median height (176 cm vs. 168 cm) were observed in the TLV ≥ 4500 cm3 group, whereas no significant differences were seen in age or BMI. Single-step operations, staged resections and ALPPS were also equally distributed in both groups (see Table 1).

Receiver operating characteristic (ROC) curve of the main cohort: Total lung volume can predict postoperative respiratory complications. Abbreviations: AUC, Area Under the Curve.
Patients with TLV < 4500 cm3 suffered from a two-fold increase in rate of respiratory complications (44% vs. 21%, p = 0.007). Furthermore, these patients also suffered from more postoperative complications in general, without achieving significance. Although not significant, the median CCI was also higher in the group with TLV < 4500cm3 (30.8 vs. 25.7, p = 0.199). The median length of ICU- and total hospital stay was similar in both groups. Further details are given in Table 2.
Univariable binary logistic regression identified TLV < 4500 cm3 (OR 2.992, 95%CI 1.323–6.765, p = 0.008), the number of intraoperative red blood cell (RBC) transfusions (OR 1.289, 95%CI 1.029–1.614, p = 0.027), the operating time (OR 1.004, 95%CI 1.001–1.008, p = 0.025) and PVE (OR 3.375, 95%CI 1.427–7.985, p = 0.006) as predictors for the occurrence of respiratory complications. Further predictors were right-sided hepatectomy (OR 4.000, 95%CI 1.120–14.287, p = 0.033), the staged resection (OR 2.421, 95%CI 1.039–5.640, p = 0.040) and ALPPS surgery (OR 3.429, 95%CI 1.137–10.341, p = 0.029). Multivariable analysis confirmed TLV < 4500 cm3 as an independent predictor for the occurrence of respiratory complications (OR 3.777, 95%CI 1.488–9.588, p = 0.005). Logistic regression results are summarized in Table 3.
Patients undergoing open surgery
The predictive ability of TLV regarding respiratory complications was stronger for patients undergoing open surgery (n = 100), with an AUC of 0.65 (p = 0.018), as shown in Supplemental Fig. 1. Here, a cut-off TLV value of 4494 cm3 (YI = 0.29) was calculated. Patients with TLV < 4494 cm3 suffered a 2.5-fold increase in rate of respiratory complications (48% vs. 20%, p = 0.004). These patients also developed more postoperative complications in general, without achieving significance (CD ≥ 3a, 61% vs. 41%, p = 0.055; CD ≥ 3b, 39% vs. 25%, p = 0.151; CD ≥ 4a: 29% vs. 13%, p = 0.054). The median CCI was also higher in the group with TLV < 4494 cm3, without achieving significance (38.1 vs. 25.7, p = 0.060). Although not significant, the median length of total hospital stay was also longer in the group with TLV < 4494 cm3 (16 vs. 11 days, p = 0.110), whereas the median length of ICU stay was similar in both groups. Further results are shown in Supplementary Table 1.
Univariable binary logistic regression analysis identified TLV < 4494 cm3 (OR 3.683, 95%CI 1.473–9.212, p = 0.005), the number of intraoperative RBC transfusions (OR 1.310, 95%CI 1.034–1.660, p = 0.025) and the number of intraoperative fresh frozen plasma (FFP) transfusions (OR 1.134, 95%CI 1.002–1.283, p = 0.046) as predictors for the occurrence of respiratory complications. Further predictors were confirmed in univariable binary logistic regression: operating time (OR 1.006, 95%CI 1.002–1.011, p = 0.006), PVE (OR 4.164, 95%CI 1.619–10.709, p = 0.003), staged resection (OR 2.793, 95%CI 1.114–7.005, p = 0.029) and ALPPS surgery (OR 4.127, 95%CI 1.284–13.260, p = 0.017). Multivariable analysis confirmed TLV < 4494 cm3 as an independent predictor (OR 4.728, 95%CI 1.374–16.274, p = 0.014) for the occurrence of respiratory complications. Results of the logistic regression analysis in patients with open surgery are summarized in Supplementary Table 2.
Non-overweight patients
We investigated the prognostic capability of TLV in different BMI groups, as defined by the WHO classification, and found significant results in the non-overweight population (BMI < 25 kg/m2). In this combined group of normal- and underweight patients (n = 50), the ROC analysis demonstrated a good predictive ability for TLV regarding respiratory complications (AUC 0.70, p = 0.021), as shown in Supplemental Fig. 2. The Youden Index analysis identified 4943 cm3 as an optimal cut-off value in these patients (YI = 0.35). In patients with TLV < 4943 cm3, the rate of respiratory complications was more than double (52% vs. 20%, p = 0.018) and the rate of life-threatening complications (CD ≥ 4a) was more than triple (40% vs. 12%, p = 0.024). Although not significant, patients with TLV < 4943 cm3 also exhibited higher median CCI (39.7 vs. 27.6, p = 0.093). The median number of days on ICU (2 vs. 1, p = 0.127) and in hospital (19 vs. 11, p = 0.047) was nearly double in patients with TLV < 4943 cm3. Further results are shown in Supplementary Table 3.
Univariable binary logistic regression analyses identified TLV < 4943 cm3 (OR 4.333 95%CI 1.235–15.206, p = 0.022) and operating time (OR 1.006 95%CI 1.000–1011, p = 0.038) as predictors for the occurrence of respiratory complications in non-overweight patients. The former was also an independent predictor in the multivariable analysis (OR 6.355 95%CI 1.369–29.501, p = 0.018). Results are summarized in Supplementary Table 4.
Patients 60 years and older
The predictive ability of TLV was also strong in patients 60 years or older (AUC = 0.69, p = 0.01), as shown in Supplementary Fig. 3. The analysis identified 5345 cm3 (YI = 0.35) as the optimal cut-off value in this group of 71 patients. Remarkably, patients with TLV < 5345 cm3 suffered from a four-fold increase in the rate of respiratory complications (44% vs. 12%, p = 0.004). These patients also developed more CD ≥ 3a complications (58% vs. 35%, p = 0.06), without achieving significance. The median CCI of these patients was significant higher (34.8 vs. 24.2, p = 0.007). Patient characteristics of this subgroup are given in Supplementary Table 5.
Univariable binary logistic regression analyses showed TLV < 5345 cm3 as a predictor for the occurrence of respiratory complications in this subgroup (OR 6.133, 95%CI 1.607–23.403, p = 0.008). Further predictors for the occurrence of respiratory complications were BMI < 25 kg/m2 (OR 2.862, 95%CI 1.017–8.055, p = 0.046), operating time (OR 1.005, 95%CI 1.000–1.010, p = 0.042) and right-sided hepatectomy (OR 6.300, 95%CI 1.319–30.091, p = 0.021). Height also had a significant influence on respiratory complications, with an OR of 0.937 (95%CI 0.881–0.996, p = 0.038), which was not found in the main study cohort. In the multivariable analysis, only TLV < 5345 cm3 (OR 6.225 95%CI 1.375–28.185, p = 0.018) was an independent predictor of respiratory complications (Supplementary Table 6).
Patients undergoing ALPPS
Patients undergoing ALPPS (n = 15) comprised the third subgroup of our analysis and TLV was found to have the best predictive ability for respiratory complications in these patients, with AUC = 0.82 (p = 0.037), as shown in Supplementary Fig. 4. The cut-off value for TLV was defined as 4249 cm3 (YI = 0.63). All patients with TLV below the defined cut-off suffered from respiratory complications (100% vs. 30%, p = 0.010) and they also exhibited a significantly higher rate of life-threatening complications (CD ≥ 4a 80% vs. 30%, p = 0.067). The median CCI was also higher in these patients, (71.7 vs. 39.5, p = 0.165) without achieving significance. Further results are given in Supplementary Table 7. Logistic regression analysis was not carried out in this group, because of the limited sample size.
Discussion
In this study, we investigated the predictive ability of preoperative CT-based 3DLV regarding postoperative respiratory complications, in patients undergoing major liver resection for CRLM. Through ROC analysis, we defined a TLV cut-off of 4500 cm3 and showed a two-fold higher rate of respiratory complications in patients with TLV below this value. To the best of our knowledge, this is the first study to demonstrate this in patients undergoing liver surgery.
Computerized 3DLV can be performed with relative ease on routine CT scans of the thorax. No additional CT with specific protocols is required. The repeatability of the lung volume measurements is excellent in both healthy persons, as well as patients with obstructive or restrictive lung disease, as shown by Shin et al.22. As previously shown12,13, 3DLV of routine chest CT scans allows a technically stable estimation of lung volume and is well correlated with spirometric measurements. In thoracic surgery, various studies have shown that 3DLV is able to reliably predict postoperative pulmonary function13,14,15,16 and to predict pulmonary complications. For example, Murakami et al. combined forced vital capacity (FVC) with TLV measurements from preoperative CT volumetry, to diagnose a lung size-function mismatch and predict cardiopulmonary complications after major lung resection for cancer 23. Kawakami et al. used preoperative 3DLV of emphysematous lungs to predict postoperative pulmonary complications in patients with chronic obstructive pulmonary disease undergoing resection of lung cancer24. Furthermore, according to Saito et al., 3DLV is able to differentiate patients who develop restrictive allograft syndrome, from those who develop bronchiolitis obliterans syndrome, after bilateral lung or heart–lung transplantation25.
Using 3DLV as a predictor for postoperative respiratory complications after major curative liver resection for CRLM is a novel application. We focused on patients undergoing major liver surgery, which is associated with higher rate of complications compared to minor liver resections. We found TLV to be predictive of respiratory, but not general complications in the ROC analysis (data not shown). Nevertheless, the ability to identify patients at risk of respiratory complications after major liver surgery is of great clinical value. Firstly, these complications can increase ICU- and hospital stay, as can new complications arising from their treatment (for example, pneumothorax after punction of a pleural effusion). This increases cumulative morbidity for the affected patients, as well as treatment costs. Secondly, physical status, including lung capacity, is amenable through pre-habilitation. Identification of patients at risk in the ambulatory setting provides the opportunity to improve their pulmonary status through exercise and physiotherapy. Finally, the same applies postoperatively, where intensive pulmonary therapy, physiotherapy, and regular monitoring of lung function (e.g., through clinical examination and bedside pleural sonography) may lead to prevention or earlier diagnosis of these complications.
To further investigate the predictive ability of TLV, we analyzed subgroups of interest, according to factors associated with lung volume and/or complication rates26,27. These included BMI < 25, age over 60, open surgery and ALPPS. Obesity is associated with reduced respiratory function and detrimental effects28,29. Zimmitti et al. showed that patients with BMI ≥ 30 kg/m2 undergoing liver surgery were more often comorbid, had longer operation duration and more intraoperative blood loss, as well as significantly higher rates of wound- and respiratory-related complications30. A linear correlation between BMI and TLV has been previously described by Jones et al.26. They found decreasing functional residual capacity (FRC) and expiratory reserve volume (ERV) with increasing BMI on all lung volume measurements. But also underweight has a negative impact on lung function, as shown by Grigsby et al. In a study with 12,396 participants, they showed individuals with lower BMI were more likely to have COPD and decreased lung function31. The association with lung function remained positive after excluding participants with COPD, suggesting that being underweight alone has a detrimental effect on lung function31. The association of BMI with lung function was apparent in our study, where the predictive ability of TLV was stronger in the non-overweight population, compared to the whole study cohort (AUC 0.70 vs. 0.62, respectively). However, we did not find a predictive ability of TLV for respiratory complications in overweight patients, probably due to the small sample size (n = 19). Further studies with larger cohorts in each BMI category are necessary to elucidate this effect.
Since lung function deteriorates from the age of 60 years onwards32, we analyzed this patient cohort separately. Remarkably, there was a fourfold increase in the rate of respiratory complications in patients with TLV below the defined cut-off-value for that subgroup. Reasons for increased rate of respiratory complications in older patients include a smaller lung volume and the natural effect of weakening of immune system in elderly patients, called immunosenescence33,34. Additionally, morphological and functional changes occur, such as smaller airway size and a decrease in lung elastic tissue, chest wall compliance, and respiratory muscle strength35,36. The reduced lung function in the elderly was reflected in the higher cut-off value for TLV in this subgroup, compared to the whole study population (5345 cm3 vs. 4500 cm3). This suggests that a higher lung volume is necessary to compensate for the reduced lung function.
Commonly, open liver surgery is associated with higher complications rates compared to minimal-invasive liver surgery37. In this cohort with patients who underwent open surgery, we found 2.5-fold higher respiratory complication rates in patients with lower TLV compared to those with higher TLV. The nearly similar cut-off value for TLV in this subgroup is explained by the fact that most patients underwent open surgery in this study (100 vs. 23).
The fourth subgroup analyzed in this study comprised patients undergoing ALPPS. The introduction of this technique was a milestone in liver surgery, allowing patients with extensive hepatic tumor burden the chance of resection, at the expense of higher rates of perioperative morbidity and mortality21,38. Refinements in patient selection and operative techniques resulted in significant improvements in perioperative outcomes over the years, but ALPPS remains a high-risk operation38,39. In our cohort, we found a significantly higher AUC value (0.82) for TLV, with regards to respiratory complications, compared to the main cohort. Additionally, all ALPPS patients below the calculated TLV cut-off suffered from respiratory complications and the rate of respiratory complications in the whole ALPSS group was twice as high as non-ALPPS patients (53% vs. 25%). This suggests a potentially great applicability of 3DLV and TLV for the prediction of respiratory complications in ALPPS patients, with the caveat of the small sample size in this study (n = 15). In any case, these results merit further investigation with a larger cohort.
Interestingly, PVE was found to be a significant risk factor for respiratory complications in the univariable logistic regression analysis. Although a quarter of our cohort (n = 31, 25%) underwent preoperative PVE, we did not analyze these patients separately, as we believe the association between PVE and respiratory complications to be indirect. In other words, these patients underwent PVE in preparation for extended or staged liver resections, which were the cause of these complications, rather than the PVE itself. This was supported by the lack of any studies in the literature reporting pulmonary complications after PVE.
Certain limitations should be considered when interpreting the results of this study, including its retrospective design, monocentric nature, and relatively small patient cohort, including subgroups. A major reason for the cohort size was the lack of thorax CT within six weeks prior to surgery, as required in the inclusion criteria of our study. We excluded older imaging, as the physical status of the patient may have significantly changed between CT and operation, especially if chemotherapy had been administered in the meantime. We did not split the dataset into training- and test-sets as this was an explorative study investigating the effects of lung volume and our goal was not to train a predictive model, rather to explore the associated effects retrospectively. The variation in timing and place of imaging between patients in our cohort is a further limiting factor. Ideally, all patients in this study would have undergone their CT on the day before surgery, at UH-RWTH, to better reflect pulmonary status at the time of operation and exclude differences in CT protocols between our center and referring hospitals or practices. Additionally, using the Brisbane classification to define major resections has inherent limitations: multiple or large atypical resections also result in significant parenchyma loss and are also associated with increased complications, due to the non-anatomical resection planes, with a larger number of transected vessels and bile ducts. Going forward, measuring the percentage of lost volume may better serve to stratify the extent of liver resection.
In any case, accounting for the study’s limitations, preoperative 3DLV with TLV measurement is a viable technique for prediction of postoperative pulmonary complications in patients undergoing major liver resection for CRLM. Particularly patients over 60 years of age, non-overweight patients, and those undergoing ALPPS could benefit from this novel application.
Conclusion
We have shown 3DLV with TLV measurement to be a viable technique for prediction of postoperative pulmonary complications in patients undergoing major liver resection for CRLM. The methodology could be routinely applied in the preoperative setting, to identify patients at risk and commence mitigating measures, such as prehabilitation. Further studies with larger cohorts and external validation are necessary to assess and optimize this technique.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- 3DLV:
-
Three-dimensional lung volumetry
- ALPPS:
-
Associating liver partition and portal vein ligation for staged hepatectomy
- ASA:
-
American society of anesthesiology
- AUC:
-
Area under the curve
- BMI:
-
Body mass index
- CI:
-
Confidence interval
- CRC:
-
Colorectal cancer
- CRLM:
-
Colorectal liver metastases
- CT:
-
Computerized tomography
- CUSA:
-
Cavitron ultrasonic surgical aspirator
- CVP:
-
Central venous pressure
- DICOM:
-
Digital imaging and communications in medicine
- FVC:
-
Forced vital capacity
- ICU:
-
Intensive care unit
- IMC:
-
Intermediate care unit
- IQR:
-
Interquartile range
- KRAS:
-
Kirsten rat sarcoma viral oncogene homolog
- MRI:
-
Magnetic resonance imaging
- OR:
-
Odds ratio
- PACS:
-
Picture archiving and communication system
- PVE:
-
Portal vein embolization
- R0:
-
Resection margin negative
- R+:
-
Resection margin positive
- TLV:
-
Total lung volume
- TNM:
-
Tumor, lymph node, metastasis
- UH-RWTH:
-
University hospital RWTH Aachen
- UICC:
-
Union for international cancer control
- YI:
-
Youden index
References
Hitpass, L. et al. Primary tumor location is a prognostic factor for intrahepatic progression-free survival in patients with colorectal liver metastases undergoing portal vein embolization as preparation for major hepatic surgery. Cancers (Basel) 12(6), 1638 (2020).
Sung, H. et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 71(3), 209–249 (2021).
Hitpass, L. et al. MRI-based quantitation of hepatic steatosis does not predict hypertrophy rate after portal vein embolization in patients with colorectal liver metastasis and normal to moderately elevated fat fraction. J. Clin. Med. 10(9), 2003 (2021).
Cervantes, A. et al. Metastatic colorectal cancer: ESMO clinical practice guideline for diagnosis, treatment and follow-up. Ann. Oncol. 34, 10–32 (2022).
Schnitzbauer, A. A. et al. Right portal vein ligation combined with in situ splitting induces rapid left lateral liver lobe hypertrophy enabling 2-staged extended right hepatic resection in small-for-size settings. Ann. Surg. 255(3), 405–414 (2012).
Jin, S. et al. Management of post-hepatectomy complications. World J. Gastroenterol. 19(44), 7983–7991 (2013).
Amygdalos, I. et al. Low postoperative platelet counts are associated with major morbidity and inferior survival in adult recipients of orthotopic liver transplantation. J. Gastrointest. Surg. 24(9), 1996–2007 (2020).
Amygdalos, I. et al. Clinical value and limitations of the preoperative C-reactive-protein-to-albumin ratio in predicting post-operative morbidity and mortality after deceased-donor liver transplantation: a retrospective single-centre study. Transpl. Int. 34(8), 1468–1480 (2021).
Amygdalos, I. et al. Novel machine learning algorithm can identify patients at risk of poor overall survival following curative resection for colorectal liver metastases. J. Hepatobiliary Pancreat. Sci. 30, 602–614 (2022).
Choudhuri, A. H. et al. Predictors of postoperative pulmonary complications after liver resection: Results from a tertiary care intensive care unit. Indian J. Crit. Care Med. 18(6), 358–362 (2014).
Zhou, Y. et al. Hepatectomy in elderly patients: Does age matter?. World J. Surg. 37(12), 2899–2910 (2013).
Haas, M., Hamm, B. & Niehues, S. M. Automated lung volumetry from routine thoracic CT scans: How reliable is the result?. Acad. Radiol. 21(5), 633–638 (2014).
Iwano, S. et al. 3D-CT volumetry of the lung using multidetector row CT: Comparison with pulmonary function tests. Acad. Radiol. 16(3), 250–256 (2009).
Kobayashi, K. et al. Three-dimensional computed tomographic volumetry precisely predicts the postoperative pulmonary function. Surg. Today 47(11), 1303–1311 (2017).
Sverzellati, N. et al. Reliability of quantitative computed tomography to predict postoperative lung function in patients with chronic obstructive pulmonary disease having a lobectomy. J. Comput. Assist. Tomogr. 29(6), 819–824 (2005).
Yabuuchi, H. et al. Prediction of post-operative pulmonary function after lobectomy for primary lung cancer: A comparison among counting method, effective lobar volume, and lobar collapsibility using inspiratory/expiratory CT. Eur. J. Radiol. 85(11), 1956–1962 (2016).
Strasberg, S. M. et al. The Brisbane 2000 terminology of liver anatomy and resections. HPB 2(3), 333–339 (2000).
Slankamenac, K. et al. The comprehensive complication index: A novel continuous scale to measure surgical morbidity. Ann. Surg. 258(1), 1–7 (2013).
Dindo, D., Demartines, N. & Clavien, P. A. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 240(2), 205–213 (2004).
WHO. A Healthy Lifestyle—WHO Recommendations (2010).
Kang, D. & Schadde, E. Hypertrophy and liver function in ALPPS: Correlation with morbidity and mortality. Visc. Med. 33(6), 426–433 (2017).
Shin, J. M. et al. The repeatability of computed tomography lung volume measurements: Comparisons in healthy subjects, patients with obstructive lung disease, and patients with restrictive lung disease. PLoS One 12(8), e0182849 (2017).
Murakami, J. et al. Size-capacity mismatch in the lung: A novel predictor for complications after lung cancer surgery. J. Surg. Res. 209, 131–138 (2017).
Kawakami, K. et al. Evaluation of emphysema using three-dimensional computed tomography: Association with postoperative complications in lung cancer patients. Nagoya J. Med. Sci. 77(1–2), 113–122 (2015).
Saito, T. et al. Low-dose computed tomography volumetry for subtyping chronic lung allograft dysfunction. J. Heart Lung Transplant. 35(1), 59–66 (2016).
Jones, R. L. The Effects of Body Mass Index on Lung Volumes (2006).
Talaminos Barroso, A. et al. Factors affecting lung function: A review of the literature. Arch. Bronconeumol. (Engl. Ed.) 54(6), 327–332 (2018).
Littleton, S. W. & Tulaimat, A. The effects of obesity on lung volumes and oxygenation. Respir. Med. 124, 15–20 (2017).
Bhatti, U., Laghari, Z. A. & Syed, B. M. Effect of body mass index on respiratory parameters: A cross-sectional analytical Study. Pak. J. Med. Sci. 35(6), 1724–1729 (2019).
Zimmitti, G. et al. Indications, trends, and perioperative outcomes of minimally invasive and open liver surgery in non-obese and obese patients: An international multicentre propensity score matched retrospective cohort study of 9963 patients. Int. J. Surg. 107, 106957 (2022).
Grigsby, M. R. et al. Low body mass index is associated with higher odds of COPD and lower lung function in low- and middle-income countries. COPD 16(1), 58–65 (2019).
Luoto, J. et al. Relative and absolute lung function change in a general population aged 60–102 years. Eur. Respir. J. 53(3), 1701812 (2019).
Duchateau, J. Immunosenescence and the lung. Rev. Mal. Respir. 20(5 Pt 1), 735–741 (2003).
Rodriguez, I. J. et al. Immunosenescence study of T cells: A systematic review. Front. Immunol. 11, 604591 (2020).
Garcia-Rio, F. et al. Lung volume reference values for women and men 65 to 85 years of age. Am. J. Respir. Crit. Care Med. 180(11), 1083–1091 (2009).
Janssens, J. P., Pache, J. C. & Nicod, L. P. Physiological changes in respiratory function associated with ageing. Eur. Respir. J. 13(1), 197–205 (1999).
Ozair, A. et al. Minimally invasive versus open hepatectomy for the resection of colorectal liver metastases: A systematic review and meta-analysis. Surg. Endosc. 36(11), 7915–7937 (2022).
Lang, H., Baumgart, J. & Mittler, J. Associated liver partition and PVE ligation for staged hepatectomy (ALPPS) registry: What have we learned?. Gut Liver 14(6), 699–706 (2020).
Linecker, M. et al. Risk adjustment in ALPPS is associated with a dramatic decrease in early mortality and morbidity. Ann. Surg. 266(5), 779–786 (2017).
Funding
Open Access funding enabled and organized by Projekt DEAL. This research project was supported by the START-Program (#01/23) of the Faculty of Medicine of the RWTH Aachen University, Aachen, Germany. The funding body was not involved in study design, data collection, data analysis, manuscript preparation or the decision to publish.
Author information
Authors and Affiliations
Contributions
The study was designed by the initiating study team (S.E., C.T., S.A.L., I.A.). Data collection and analysis were carried out by S.E., P.M., I.A. The manuscript was drafted by S.E. All additional authors contributed substantially to the final version of the manuscript. All authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Elmaagacli, S., Thiele, C., Meister, F. et al. Preoperative three-dimensional lung volumetry predicts respiratory complications in patients undergoing major liver resection for colorectal metastases. Sci Rep 14, 10594 (2024). https://doi.org/10.1038/s41598-024-61386-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-61386-8
Keywords
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
