
Abstract
New technologies such as laparoscopic and robotic surgery are spreading, and there is a demand for physicians to keep up with novel methods. In contrast to the recent focus on healthcare professional burnout, the mental and physical costs during surgery are not well-understood. We aimed to quantify surgeons’ workloads in daily urological surgical practice and clarify potential background factors associated with such workloads. Urologists in Hokkaido, Japan, were invited to this study. Between December 2020 and December 2021, participants repeatedly reported workloads, which were assessed using the National Aeronautics and Space Administration-Task Load Index (NASA-TLX), after each surgery in conjunction with participants’ names, patients’ backgrounds, their roles (independent operator, operator under supervision, instructor, and 1st or 2nd assistant), and surgical outcomes, via SurveyMonkey®. Because of the heterogeneity among individuals, a linear mixed-effects model was utilized to analyze factors associated with NASA-TLX, calculating the parameter estimates (PE) of regression coefficients for each factor and their 95% confidence interval (CI). Sixty-five urologists (5 women) joined the study, and 2169 data were collected within 7 days after surgeries. A linear mixed-effects model revealed that female surgeons (PE + 15.56, 95% CI 2.36–28.77), urgent/emergency surgery (PE + 6.65, 95% CI 4.59–8.70), intraoperative complications (PE + 9.26, 95% CI 6.76–11.76), and near-miss incidents (PE + 3.81, 95% CI 2.27–5.36) were associated with higher workloads. Regarding the surgeons’ role, operator under supervision (PE + 12.46, 95% CI 9.86–15.06) showed the highest workloads. Surgeons’ workloads decreased as the number of previous cases of the same procedure increased. Surgeons’ workloads were associated with various factors. Given that the highest workloads were for operators under supervision, instructors should be aware of trainees’ high workloads and devise appropriate instructional interventions.
Similar content being viewed by others

Introduction
Recently, healthcare professional burnout has been emphasized1,2,3,4,5,6,7,8. For example, Pulcrano M et al.3 reported in their systematic review across multiple surgical specialties that high emotional exhaustion was observed in up to 31% of attending surgeons versus up to 42% of residents, high depersonalization was observed in up to 26% of attending surgeons versus up to 53% of residents, and a low personal sense of accomplishment was observed in up to 54% of attending surgeons versus up to 55% of residents. Al-Ghunaim et al.4 reported in their meta-analysis that surgeon burnout was significantly correlated with a higher incidence of medical errors. Symptoms of burnout were also noted in urology1,2,5,6. Harris AM et al.2 observed that, based on the American Urological Association census survey, in 2021, 36.7% of urologists reported burnout according to the Maslach Burnout Inventory, compared with 36.2% in 2016.
In surgical care including urology, according to the spreading of new technologies such as laparoscopic and robotic surgery, there is a demand for physicians to keep up with these emerging novel methods, and the mental and physical costs during surgery have also drawn scientific interest. Law et al. recently reported that a robot-assisted approach was associated with less mental demand, physical demand, and effort than open or laparoscopic after assessing the National Aeronautics and Space Administration Task Load Index (NASA-TLX) to self-assess workload following abdominopelvic colon and rectal surgeries9.
Beyond question, the operating room is a place where marked workloads are placed on medical staff, and surgeons frequently have to address difficult problems under time pressure. In order to promote the well-being of surgeons, develop better training curriculums, and improve surgical performance and patient safety, we consider that it is paramount to better understand surgeons’ mental workloads (MWLs). In the present study, we quantified surgeons’ workloads in daily urological surgical practice, and clarified potential background factors associated with MWLs.
Methods
This prospective study was approved by the Institutional Review Board at Hokkaido University Hospital Clinical Research Administration Center (No. 020-0159) and conducted in accordance with the Declaration of Helsinki as well as the Ethical Guidelines for Medical and Health Research Involving Human Subjects. Urologists practicing at Hokkaido University Hospital and affiliated institutions were recruited for the present study by email. After obtaining written informed consent regarding the use of their data for research, participants’ demographic data were collected via an online survey tool (SurveyMonkey®, https://www.surveymonkey.com/), such as: age, sex, year of graduation from medical university, years of clinical experience in urology, board-certified urologist, certification of attending doctor, that of laparoscopic surgery, and that of robotic surgery. Previous surgical experiences as a primary surgeon or an instructor (leading role) were also collected regarding transurethral, open, laparoscopic, or robotic surgery.
NASA-TLX collection
Between December 2020 and December 2021, after each surgical case, participants reported their NASA-TLX scores via SurveyMonkey®, using the original version in English. NASA-TLX includes six subscales: mental, physical, and temporal task demands, as well as effort, frustration, and perceived performance, and the questionnaire uses a 20-point visual analogue scale to measure MWLs based on the 6 abovementioned subscales10. Participants’ names, operative procedure, previous surgical experience of the same procedure as a primary or leading surgeon, surgical role (independent operator, operator under supervision, instructor, and 1st or 2nd assistant), patients’ backgrounds (age, sex, and comorbidities), surgical information (date, elective or urgent/emergency surgery, operative time, blood loss, and order of surgery on the day), intraoperative complications, near-miss incidents (such as anatomical misidentification, surgical equipment malfunction, trouble with anesthesia, intraoperative telephone calls, communication errors in the surgical team, etc.), subjective procedure difficulty, and on-call duty last night, were also collected. Furthermore, participants were allowed to describe additional surgical findings in the free-description column, such as: adhesive visceral fat due to obesity, difficulty due to patients’ body size, marked adhesion in the abdominal cavity, and collaborative surgery with other disciplines, and such information was classified as “other difficulty” for subsequent analysis. In this study, because we collected NASA-TLX scores not only from operators, but also from assistants, there could be overlapping patients in the present dataset. During the study period, one of the authors (SH) emailed the total number of reported cases at the end of every month to participants as a study reminder.
Data analysis
During the 13 months of the study period, NASA-TLXs were collected from the participants after surgeries. Considering the effect of time-dependent memory loss, we included data reported within 7 days after surgery in the present analysis. Cases with missing data were excluded from the analysis.
In the present study, we aimed to explore the overall relationship between mental workloads of urologic surgeons and potentially influencing factors abovementioned. Because of the heterogeneity among individuals, we utilized a linear mixed-effects model, a statistical model containing both fixed and random effects, to analyze the factors associated with NASA-TLX, estimating the regression coefficients for each factor and calculating their 95% confidence interval11. We included an individual participant identifier as a random effect, considering the subjective tendency of reporting high or low NASA-TLX scores. We then included surgeons’ sex, previous experience (years), information on certificates (laparoscopic or robotic surgery), previous surgical experiences of the same procedure, surgical role (independent operator, operator under supervision, instructor, first assistant, or second assistant), order of surgery on the day, on-call duty last night, patients’ information (age, sex, history of hypertension, diabetes, cardiovascular disease, cerebrovascular disease, cancer, and previous surgical experience), surgical situation (elective or emergency surgery), surgical approach (open, laparoscopic, robotic, transurethral, or others), surgical outcomes (operative time, blood loss, intraoperative complications, and near-miss incidents), and other difficulties as covariates with fixed effects. For combination surgeries involving multiple procedures performed simultaneously, two of the authors (SH and TA) discussed and classified them. For example, in combination surgeries like robot-assisted radical cystectomy and laparoscopic radical nephroureterectomy, we classified it as “Robotic”. All calculations were performed using JMP® Pro, version 17.0.0 (SAS Institute, Cary, NC, USA). Descriptive statistics were also calculated using JMP Pro, version 17.0.0. P < 0.05 was considered significant.
Results
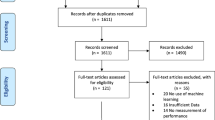
During the study period, a total of 2372 surgeries were reported from 67 participants. Of those, 2185 (92.1%) were reported within 7 days after surgery by 65 urologists [1384 (58.4%) were reported on the day of surgery, 317 (15.6%) were on the next day, and 430 (18.1%) were 2–7 days later]. Of the 2185 cases, after excluding 16 cases with missing data, 2169 cases (91.4%) were finally included in the analysis. The median number of reports per surgeon was 17 (range, 1–177). Ninety-five cases (4.4%) were reported by 5 female surgeons. Table 1 summarizes the backgrounds of 65 participants. The median age was 42 years (range, 27–61), and the median years of previous clinical experience was 15 (range, 1–36). Female surgeons accounted for 7.7% (5/65). Regarding skill qualification, 28 (43.1%) had the endoscopic surgical skill qualification authorized by Japanese Society of Endourology and Robotics12, and 40 (61.5%) had Da Vinci® certification.
Table 2 summarizes the 2169 surgeries collected in this study. Elective surgery accounted for 90.3% (1959/2169), and emergency surgery for 9.7% (210/2169). Regarding the surgical approach, “Open” accounted for 11.9% (259/2169), “Laparoscopic” for 14.8% (321/2169), “Robotic” for 19.1% (415/2169), “Transurethral” for 33.8% (733/2169), and other procedures for 20.3% (441/2169). Regarding the surgeons’ role, operator (independent) accounted for 23.1% (501/2169), operator under supervision for 28.8% (625/2169), 1st assistant as an instructor for 30.4% (659/2169), 1st assistant for 10.5% (228/2169), and 2nd assistant for 7.2% (156/2169). Surgeons reported subjective procedural difficulty levels as follows: 64.7% as expected (1403/2169), 25.0% more difficult than expected (542/2169), and 10.2% less difficult than expected (221/2169). Intraoperative complications were reported in 6.4% (138/2169), including injuries of other organs (n = 61), urethral injuries during transurethral surgeries (n = 34), massive bleeding (n = 19), vascular problems (n = 14), and others (n = 10). Regarding near-miss incidents, intraoperative telephone calls were the most frequent (49.4%, 310/627), followed by malfunctions and connection problems with surgical forceps and devices (19.6%, 123/627), and anatomical misidentifications (8.1%, 51/627) (Supplementary Table 1). In terms of other difficulties, marked adhesion in the abdominal cavity was the most common at 35.4% (69/195), followed by experiencing any difficulty or exhaustion during the procedure at 24.1% (47/195), and surgery with an unscheduled procedure at 11.3% (22/195) (Supplementary Table 2). Supplementary Tables 3 and 4 summarize patients’ histories other than previous surgery and cancer, and details of surgical procedures.
Factors associated with NASA-TLX scores
Overall, the 65 participants reported a mean NASA-TLX score of 32.2 (standard deviation [SD]: 22.7) for 2169 surgeries in total. Figure 1 shows a comparison of mean NASA-TLX subscales. Effort was the highest reported subscale (mean: 5.82, SD 4.58), followed by mental demand (mean 5.72, SD 4.41), and frustration (mean: 5.52, SD 4.49). To identify factors associated with NASA-TLX scores, we utilized a linear mixed-effects model. Figure 2 shows scatter plots between actual and predicted NASA-TLX scores based on the present linear mixed-effects model. The random coefficients (intercepts) varied widely among the participants (Supplementary Fig. 1). Table 3 summarizes the estimates (slopes) of fixed effects, and Fig. 3 shows a waterfall-plot of the significant characteristics. Female surgeons showed higher NASA-TLX scores (Parameter estimate [PE] + 15.56, 95% confidence interval [CI] 2.36–28.77; p = 0.022) than male surgeons. While urgent/emergency surgery was associated with higher MWLs (PE + 6.65, 95% CI 4.59–8.70; p < 0.001) compared with elective surgery, the order of surgery on the day showed no significant correlation with MWLs. MWLs decreased with increased previous surgical experiences of the same procedure, although years of previous surgical experience did not show a significant correlation with MWLs. Regarding the surgeons’ role (reference standard: 2nd assistant), operator under supervision showed the highest MWLs (PE + 12.46, 95% CI 9.86–15.06; p < 0.001), followed by independent operator (PE + 7.12, 95% CI 4.34–9.91; p < 0.001), 1st assistant as an instructor (PE + 5.46, 95% CI 2.67–8.25; p < 0.001), and 1st assistant (PE + 3.32, 95% CI 0.33–6.31; p = 0.030). Furthermore, NASA-TLX scores were increased by + 0.07 per minute of operative time (95% CI 0.06–0.08; p < 0.001), and + 0.002 per mL of blood loss (95% CI 0.001–0.003; p < 0.001), and higher for unexpected intraoperative events [+ 9.26 higher for intraoperative complications (95% CI 6.76–11.76; p < 0.001), and + 3.81 higher for near-miss incidents (95% CI 2.27–5.36; p < 0.001)]. Other difficulties were also associated with higher MWLs (PE + 12.22, 95% CI 10.04–14.39; p < 0.001). Surgeons’ experience, technical qualifications, on-call duty, and patients’ factors (age, sex, history) did not show significant correlations with MWLs.

Comparison of mean NASA-TLX subscales Effort was the highest reported subscale (mean 5.82, standard deviation [SD] 4.58), followed by mental demand (mean 5.72, SD 4.41), and frustration (mean 5.52, SD 4.49). Error bars in the graph represent the standard deviation.

Scatter plots between actual and predicted NASA-TLX scores based on the present linear mixed-effects model.

Waterfall-plot of the significant estimates (slopes) of the present mixed-effects model Red bars represent the impact on higher workloads, and blue bars represent the impact on lower workloads. Error bars in the graph represent 95% confidence intervals. Operative time and blood loss are shown enlarged because the length of each bar is very short. Female surgeons, urgent or emergency surgery, and unexpected intraoperative events (intraoperative complications and near-miss incidents) were associated with higher workloads. In terms of the surgeon’s role, operator under supervision had the highest workload. As previous surgical experiences of the same procedure increased, surgeons’ workloads decreased.
Discussion
Recently, burnout among surgeons has been well-recognized and reported to be influenced by multifactorial backgrounds. Shanafelt TD et al. reported that, in an anonymous survey involving members of the American College of Surgeons with a response rate of 32% (7905/24,922), a high rate of burnout syndrome (severe emotional exhaustion and depersonalization) was observed in 40% of respondents, and a younger age, having children, the area of specialization, number of nights on call per week, hours worked per week, and having compensation determined entirely based on billing were independent factors7. Chati R et al. observed that, in an anonymous questionnaire survey involving French digestive surgeons with a response rate of 65.6% (328/500), 62% of the surgeons had burnout syndrome, and a multivariate model revealed that perceived aggression from patients, lack of gratitude on the part of seniors, a level of responsibility deemed unsuitable, and the absence of extracurricular activities were independent adverse factors8.
Operations demand marked workloads and surgeons frequently have to tackle with difficult situations under time pressure. As abovementioned, in order to better understand surgeons’ MWLs in daily clinical practice, we prospectively collected surgeons’ MWLs in real-world surgical cases with a wide range of procedure types, which were performed by urologic surgeons at a variety of career levels, including trainees. As data were repeatedly collected from each participant (not only from operators, but also from assistant surgeons) via an online survey tool with a registered form (with individual names), we utilized a linear mixed-effects model, which included an individual participant identifier as a random effect, and evaluated factors (fixed effects) related to subjective MWLs assessed by NASA-TLX, considering individual tendencies at the time of reporting MWLs. As expected, the random effects varied widely among the present participants (range: − 20.94 to + 24.19); in other words, each participant had a certain tendency of reporting high or low NASA-TLX scores.
Regarding the surgeons’ role, operators showed higher MWLs compared with the reference standard of the 2nd assistant. Furthermore, operators under supervision showed the highest MWLs. Our observations may reflect two aspects: one is that operators perform difficult cases, and they need senior doctors’ advice; and the other is that operators are in a training phase, and they still need continuous supervision. In both situations, in order to optimize surgical outcomes and education, supervising instructors should understand trainees’ high MWLs under their supervision, and prevent excessive workloads by adopting an appropriate attitude.
In this study, female surgeons showed higher MWLs than male surgeons. While the present cohort included a limited number of female surgeons (n = 5, 95 workload data), we have certain concerns regarding the current observations. Sex inequality in the workplace remains an unresolved problem, including surgeons and surgical trainees13. Joh DB et al. analyzed 119,380 general surgery procedures performed by 120 trainees (male = 78, female = 42) in New Zealand between 2012 and 2017. Operative autonomy was classified by the trainees for each procedure according to 5 levels: (1) Assisting senior resident, (2) Assisting surgeon mentor, (3) Primary operator with surgeon mentor scrubbed, (4) Primary operator with surgeon mentor in the operating room, (5) Primary operator with surgeon mentor available. When defining meaningful autonomy as levels 4 and 5, female trainees performed fewer procedures with meaningful autonomy than male trainees14. Meyerson et al. utilized a smartphone app and collected operative autonomy assessments according to the 4-point Zwisch scale (1. Show and tell, 2. Active help, 3. Passive help, 4. Supervision only). During the 9-month study period, 412 residents and 524 faculty members evaluated 8900 cases, and female residents received less autonomy from faculty members than male residents overall15. Furthermore, in terms of professional burnout in urology, female urologists reported a higher prevalence of burnout2,6. At present, although we do not have a clear explanation for higher intraoperative MWLs in our female cohort, we believe that autonomy in the operating room is a pivotal part of surgical training, which helps trainees develop confidence and realize their current limitations, and mentors should determine the degree of trainees’ latitude based on their current competency, not sex bias. Gas et al.6 reported very important findings based on self-assessment questionnaires sent to trainees of the French Association of Urologists, whereby a “Feeling of being well-trained” was the only protective factor against emotional exhaustion, depersonalization, and negative feelings of personal accomplishment.
Regarding the length of surgery, NASA-TLX scores increased by + 0.07 per minute of surgical time. Rieger et al.16 also reported a similar observation. They evaluated surgeons’ intraoperative workloads through a mobile health system, such as heart rate, breathing rate, and skin temperature, and NASA-TLX scores. Ten surgeons participated in their 24-h monitoring study, and the length of surgery had a significant impact on NASA-TLX scores, while working as primary surgeons did not result in higher workloads. Although intermittent breaks during surgery are not common, several researchers reported promising findings17,18. Engelmann C et al., in their prospective randomized study, assigned 51 operations randomly to an investigational group with intraoperative breaks or a conventional group without intraoperative breaks, and the investigational group showed lower stress hormone levels, intraoperative events, and error-performance scores, without prolonging the operative duration18.
In this study, near-miss incidents were associated with higher MWLs. In Supplementary Table 1, these events mostly represented distractions during surgeries. According to the cognitive load theory, a well-known learning theory proposed by Sweller et al., the present near-miss incidents could be categorized into Extraneous loads. Our observation, in which NASA-TLX scores decreased according to increased previous caseloads of the same procedure, should reflect the decrease of Intrinsic load which comes from difficulty, complexity, or prior experience of the procedure. To maximize learning chances of trainees, in other words, maximize Germane load for learning, we consider that extraneous loads should be minimized during surgery. Unnecessary intraoperative disruptions such as telephone calls should be avoided as much as possible.
This study had several limitations. First, because data collection was performed in a voluntary manner, we could not collect workload data from all surgical cases during the study period. Thus, there may be a bias between reported and non-reported cases. Second, we included only 5 female participants, and the wide range of CI (2.36–28.77) may be related to this small number. We need to assess a larger cohort in the future to confirm our findings. Third, this study was performed among Japanese urologists in Hokkaido Prefecture, and so our observations may be biased due to this cohort. Similar studies are warranted to assess whether the present findings are universal. Fourth, during the study period, we had the novel coronavirus disease (COVID) 2019 pandemic. Although Japan did not experience lockdown measures and mortality due to COVID-19 infection remined low (0.2%), surgeons’ workloads may have been indirectly influenced. Fifth, in addition to surgery, urologists have numerous other duties such as outpatient clinics, in-hospital patient management, on-call/night-shifts, academic jobs, and other miscellaneous work. Nevertheless, we believe that our observations facilitate a better understanding of surgeons’ MWLs in daily clinical practice, being helpful for promoting the well-being of surgeons, developing better training curriculums, and improving surgical performance and patient safety.
Conclusion
Surgeons’ MWLs were associated with various factors. Regarding the surgeons’ role, operators showed higher MWLs, especially under supervision. Instructors should be aware of the high MWLs of trainees under their supervision and devise appropriate instructional interventions.
Data availability
The datasets generated and/or analyzed during the current study are not publicly accessible, but are available from the corresponding author on reasonable request.
Abbreviations
- CI:
-
Confidence interval
- COVID-19:
-
Coronavirus disease 2019
- MWLs:
-
Mental workloads
- NASA-TLX:
-
National aeronautics and space administration-task load index
- PE:
-
Parameter estimates
- SD:
-
Standard deviation
References
Dyrbye, L. N. et al. Association of clinical specialty with symptoms of burnout and career choice regret among us resident physicians. JAMA 320, 1114–1130. https://doi.org/10.1001/jama.2018.12615 (2018).
Harris, A. M. et al. Burnout: A call to action from the AUA workforce workgroup. J Urol. 209, 573–579. https://doi.org/10.1097/JU.0000000000003108 (2023).
Pulcrano, M., Evans, S. R. & Sosin, M. Quality of life and burnout rates across surgical specialties: A systematic review. JAMA Surg. 151, 970–978. https://doi.org/10.1001/jamasurg.2016.1647 (2016).
Al-Ghunaim, T. A. et al. Surgeon burnout, impact on patient safety and professionalism: A systematic review and meta-analysis. Am. J. Surg. 224, 228–238. https://doi.org/10.1016/j.amjsurg.2021.12.027 (2022).
Marchalik, D. et al. Resident burnout in USA and European urology residents: an international concern. BJU Int. 124, 349–356. https://doi.org/10.1111/bju.14774 (2019).
Gas, J. et al. Prevalence of and predictive factors for burnout among French urologists in training. Eur. Urol. 75, 702–703. https://doi.org/10.1016/j.eururo.2018.12.037 (2019).
Shanafelt, T. D. et al. Burnout and career satisfaction among American surgeons. Ann. Surg. 250, 463–471. https://doi.org/10.1097/SLA.0b013e3181ac4dfd (2009).
Chati, R. et al. Factors associated With burnout among French digestive surgeons in training: Results of a national survey on 328 residents and fellows. Am. J. Surg. 213, 754–762. https://doi.org/10.1016/j.amjsurg.2016.08.003 (2017).
Law, K. E. et al. NASA-task load index differentiates surgical approach: Opportunities for improvement in colon and rectal surgery. Ann. Surg. 271, 906–912. https://doi.org/10.1097/SLA.0000000000003173 (2020).
SGSS, H. Development of NASA-TLX: Results of empirical and theoretical research. In Human Mental Workload (eds Hancock, P. A. & Meshkati, N.) (Elsevier, 1987).
Gibbons, R. D., Hedeker, D. & DuToit, S. Advances in analysis of longitudinal data. Annu. Rev. Clin. Psychol. 6, 79–107. https://doi.org/10.1146/annurev.clinpsy.032408.153550 (2010).
Matsuda, T. et al. The endoscopic surgical skill qualification system in urological laparoscopy: A novel system in Japan. J. Urol. 176, 2168–2172. https://doi.org/10.1016/j.juro.2006.07.034 (2006).
Stephens, E. H., Heisler, C. A., Temkin, S. M. & Miller, P. The current status of women in surgery: How to affect the future. JAMA Surg. 155, 876–885. https://doi.org/10.1001/jamasurg.2020.0312 (2020).
Joh, D. B. et al. Assessment of autonomy in operative procedures among female and male New Zealand general surgery trainees. JAMA Surg. 155, 1019–1026. https://doi.org/10.1001/jamasurg.2020.3021 (2020).
Meyerson, S. L. et al. The effect of gender on operative autonomy in general surgery residents. Surgery 166, 738–743. https://doi.org/10.1016/j.surg.2019.06.006 (2019).
Rieger, A. et al. Psychophysical workload in the operating room: Primary surgeon versus assistant. Surg. Endosc. 29, 1990–1998. https://doi.org/10.1007/s00464-014-3899-6 (2015).
Park, A. E. et al. Intraoperative “Micro Breaks” with targeted stretching enhance surgeon physical function and mental focus: A multicenter cohort study. Ann. Surg. 265, 340–346. https://doi.org/10.1097/SLA.0000000000001665 (2017).
Engelmann, C. et al. Effects of intraoperative breaks on mental and somatic operator fatigue: A randomized clinical trial. Surg. Endosc. 25, 1245–1250. https://doi.org/10.1007/s00464-010-1350-1 (2011).
Acknowledgements
We thank A. Sazawa, H. Katano, H. Matsuda, H. seki, H. Suzuki, H. Tanaka, I. Takeuchi, J. Shindo, K. Matsuda, K. Morita, K. Tsuchiya, N. Enami, R. Machino, S. Sato, T. Harabayashi, T. Hioka, T. Mochizuki, T. Mori, T. Yamashita, Y. Sasaki, Y. Shinno, and all the surgeons who participated in this study.
Author information
Authors and Affiliations
Contributions
S.H. and T.A. had full access to all data in the study and take responsibility for the integrity of the data and accuracy of data analysis. Conception and design: T.A. Data acquisition: S.H., T.A., J.F., K.H., N.A., M.K., S.M., H.M., H.K., R.M., and T.O. Data analysis and interpretation: S.H. and K.T. Drafting the manuscript: S.H. and T.A. Critical revision of the manuscript: S.H., T.A., J.F., K.T., K.H., N.A., M.K., S.M., H.M., H.K., R.M., T.O. and N.S. Statistical analysis: S.H. and K.T. Supervision: N.S. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Harada, S., Abe, T., Furumido, J. et al. A prospective study of surgeons’ workloads and associated factors in real-world practice. Sci Rep 14, 9741 (2024). https://doi.org/10.1038/s41598-024-59596-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-59596-1
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
