
Abstract
To investigate the association between serum neurofilament light chain (NfL) levels, inflammatory cytokines, and cognitive function to assess their utility in the early detection of mild cognitive impairment (MCI). We conducted a cross-sectional study involving 157 community-dwelling individuals aged 55 years and above, categorized into healthy controls, MCI, and probable Alzheimer's disease (AD). Serum levels of NfL, inflammatory cytokines, and AD pathology markers were measured using enzyme-linked immunosorbent assay (ELISA). Correlations between these biomarkers and cognitive function were analyzed, and the diagnostic performance of the cognitive assessment scales and serum biomarker concentrations was evaluated using receiver operating characteristic (ROC) curve analysis. Serum NfL levels were significantly elevated in MCI and probable AD groups compared to healthy controls. Positive correlations were found between serum NfL and inflammatory cytokines IL-1β, IL-6, and Aβ40. Combining serum NfL with p-tau217 and the Boston Naming Test significantly enhanced the predictive accuracy for MCI. However, combining serum NfL with inflammatory markers did not improve MCI prediction accuracy. Elevated serum NfL is associated with cognitive impairment and inflammatory markers, suggesting its potential as a peripheral serum biomarker for MCI detection. The combination of serum NfL with p-tau217 and cognitive tests could offer a more accurate prediction of MCI, providing new insights for AD treatment strategies.
Similar content being viewed by others


Introduction
Alzheimer's disease (AD) is a neurodegenerative disorder hallmarked by the accumulation of amyloid-beta (Aβ) and tau proteins, brain tissue atrophy, and progressive cognitive decline1.The global prevalence of AD is escalating in tandem with the aging population. The International Alzheimer's Disease Association reported approximately 46 million individuals with AD worldwide in 2018, with projections suggesting a rise to 131.5 million by 20502. In China, recent epidemiological data indicates a dementia prevalence of 6.04%, with AD accounting for 3.94% among those over 60, translating to nearly 9.83 million AD patients and an increasing socio-economic impact3.
The challenge of timely and accurate dementia diagnosis is formidable, with an estimated three-quarters of dementia cases remaining undiagnosed globally, a figure that could be as high as 90% in low- and middle-income countries. Current diagnostic markers, such as cerebrospinal fluid (CSF) Aβ and tau proteins, along with neuroimaging techniques like MRI, tau-PET, β-amyloid-PET, and F-FDG-PET, facilitate early AD detection but are limited by invasiveness, cost, and accessibility4. Consequently, there is an urgent need for less invasive and more cost-effective biomarkers.
Neurofilaments, specifically the light chain (NfL), have garnered attention as potential peripheral biomarkers for neuronal damage. Neurofilaments are neuron-specific, highly phosphorylated proteins that form a key component of the axonal cytoskeleton, with NfL being a critical subunit involved in axonal growth and stability5. Under physiological conditions, axonal cells release minimal amounts of NfL into the CSF, which can then enter the bloodstream, albeit at lower concentrations. However, pathological conditions trigger a marked increase in NfL, making it a sensitive marker for axonal injury6. Elevated CSF NfL levels have been associated with cognitive impairment, with studies demonstrating its rise in early AD and its correlation with cognitive decline and brain structural changes7. A study has found that the content of NfL is correlated with age, and NfL concentrations increased at a rate of 3.1% per year of age. Elevated CSF NfL has also been observed in other dementias, correlating with lower Mini-Mental State Examination (MMSE) scores and reduced survival times8. Furthermore, higher NfL levels have been linked to cognitive decline in mild cognitive impairment (MCI) and AD patients, irrespective of vascular burden9. Furthermore, a longitudinal study showed that the concentration of light filament chains at baseline predicted future cognitive performance in patients with small cerebral vessels10, raising the possibility that light filament chains could be used to predict future cognitive function in dementia.
Given the invasive nature of CSF collection, the focus has shifted towards blood-based NfL measurements. Because the use of Single Molecule Array (Simoa) technology analysis platform limits the feasibility of NfL as a global biomarker, we choose the simpler and more operable ELISA in terms of measurement method. Significant correlations between plasma NfL and CSF biomarkers have been reported, with increased plasma NfL levels observed in MCI and AD, suggesting its potential as a non-invasive biomarker for cognitive impairment1,11. The relationship between NfL and cognitive function in the older adults is further supported by its role as an axonal damage marker, which is closely related to microglial activation in the central immune system12. Inflammation is increasingly recognized as a contributor to neurodegeneration, with systemic elevations of pro-inflammatory cytokines like TNF-α implicated in cognitive decline in AD13,14. The dysregulation of inflammatory pathways in MCI may also serve as a predictor for the rate of cognitive deterioration15. While there is evidence of a strong correlation between plasma NfL and both peripheral and cortical inflammation during AD progression, and suggestions of AD as a chronic autoimmune condition with heightened pro-inflammatory factors16,17, research into the relationship between blood NfL and inflammatory markers remains limited. More than 40 years ago, the Chinese government introduced policies to carry out educational reforms, which not only focused on primary and secondary education, but also placed greater emphasis on university education, providing many people with opportunities to receive higher education. This had led to the diversity of cultural levels among elderly residents in the community. Therefore, based on this population, this study explores the role of serum NfL and inflammatory cytokines in early detection of MCI, and clarify the relationship between serum NfL and inflammatory markers.
Materials and methods
Study design and participants
This cross-sectional study was conducted from April 2021 to February 2022 in Hebei Province, China. Participants were recruited from the Yuhua District of Shijiazhuang City and Renze District of Xingtai City, resulting in a cohort of 157 older adults aged 55 years and older, comprising 74 males and 83 females. All participants were asked if they were willing to participate in this study and each person signed an informed consent form. The study was approved by the Ethics Committee of the First Hospital of Hebei Medical University (ethical approval number: 20190416). We confirm that all research were performed in accordance with relevant guidelines and regulations.
Inclusion and exclusion criteria
Inclusion criteria for the study were as follows: (1) age 55 years or older; (2) willingness and ability to participate in and complete a comprehensive questionnaire survey and cognitive function evaluation; (3) consent to provide blood samples for analysis. Exclusion criteria were established to omit individuals with potential alternative causes of cognitive decline, including those with a clear history of stroke, brain tumor, Parkinson's disease, epilepsy, severe head trauma, and significant mental disorders. Additionally, individuals with severe physical illnesses or substantial visual or hearing impairments that could interfere with cognitive function testing were excluded.
Diagnostic criteria
Participants were classified into two groups: Healthy older adults with normal cognition (healthy control, HC) and those with cognitive impairment, and the cognitive impairment group was further divided into the MCI group and the probable AD group.
HC Group Diagnostic Criteria:
-
(1)
Objective evidence of normal cognitive function, stratified by educational level with respective cut-off scores on the MMSE: ≥ 19 points for illiterate, ≥ 22 points for elementary school, and ≥ 24 points for junior high school and above18. Additionally, Montreal Cognitive Assessment (MoCA) scores of ≥ 13 points, ≥ 19 points, and ≥ 24 points were required for the respective educational levels19.
-
(2)
Normal daily living abilities, as indicated by a score of ≤ 26 points on the Activity of Daily Living Scale (ADL)20.
MCI Diagnostic Criteria:
As per the consensus established by the Chinese Expert Group on Cognitive Impairment Prevention and Treatment in 200621 , MCI diagnosis included:
-
1.
Self-reported or family-observed significant memory impairment.
-
2.
Preservation of other cognitive functions or only mild impairment, with MMSE scores of ≥ 19 for illiterate, ≥ 22 for elementary school, and ≥ 24 for junior high school or above. Corresponding MoCA scores should be < 13, < 19, and < 24, respectively.
-
3.
Maintenance of basic daily living activities, with an ADL score ≤ 26.
-
4.
Exclusion of dementia, ensuring that the criteria for dementia diagnosis are not met.
-
5.
Exclusion of other systemic diseases that could affect cognitive function.
Probable AD Diagnostic Criteria22:
-
(1)
Documented history of cognitive decline, as evidenced by reduced scores on neurocognitive tests, specifically MMSE scores of < 19 for illiterate, < 22 for elementary school, and < 24 for junior high school or higher education.
-
(2)
Slight impairment in daily living activities, with an ADL score > 26.
Data collection procedures
Trained survey personnel conducted the data collection process, which included administering a custom-designed general information survey form to collect demographic data such as age, gender, education level, smoking and alcohol consumption habits, and medical history.
Neuropsychological assessments
Cognitive function was assessed using the MMSE18 and the MoCA19. The MMSE is a widely utilized tool that evaluates nine cognitive domains, including temporal and spatial orientation, immediate memory, calculation, delayed recall, naming, repetition, comprehension, and visuospatial abilities, with a maximum score of 30 points. The scoring is adjusted for cultural differences.
The MoCA is known for its higher sensitivity in detecting mild cognitive deficits compared to the MMSE. It evaluates several cognitive domains: visuospatial and executive functions, naming, memory, attention, language, abstraction, delayed recall, and orientation.
Additionally, the Boston Naming Test (BNT)23 was used to assess language production, specifically the ability to name pictorial representations, and the Digit Span Test (DST)24 measured immediate memory, attention, and processing speed.
Blood sample collection and processing
Blood samples were collected from participants following an overnight fast. Standardized venipuncture procedures were performed in the morning by trained nurses, who collected 5 mL of venous blood from each participant in EDTA vacuum collection tubes (Inspeck, ST750EK, Sekisui, Osaka, Japan) at 8:00 a.m. in the morning. The whole blood samples were allowed to clot at room temperature for 2 h before centrifugation at 3000 rpm for 10 min25. The resulting serum was aliquoted using a serum separator tube and stored at − 80 °C until analysis, to avoid repeated freeze–thaw cycles.
Serum concentrations of NfL, Interleukin-1β (IL-1β), Interleukin-6 (IL-6), Tumor Necrosis Factor-α (TNFα), Amyloid-β40 (Aβ40), Amyloid-β42 (Aβ42), and phosphorylated tau protein 217 (p-tau217) were measured using enzyme-linked immunosorbent assay (ELISA) kits (Product IDs: CSB-E16094h, EK101B-24, EK106/2-24, EK182-24, CSB-E08299h, CSB-E10684h, ZC-55233, respectively). All kits are from ZCIBIO Technology Co.,Ltd, Business license code 91310120MA1HM97U98.
The ELISA procedure was conducted as follows: Reagents were equilibrated to room temperature (18–25 °C) for at least 30 min. Following the manufacturer's instructions, reagents were prepared and added to the ELISA plate wells, with 100 μl of standard or test sample per well. After mixing and sealing, the plates were incubated at 37 °C for 2 h. Post-incubation, the liquid was discarded, and the wells were washed three times with a 2-min soak of 200 μl per well. Subsequently, 100 μl of biotin-labeled antibody working solution was added to each well and incubated for another hour at 37 °C. Following this, the wells were washed five times, and 100 μl of horseradish peroxidase-labeled avidin working solution was added to each well. After a final hour of incubation and washing, 90 μl of substrate solution was added to each well, and the plates were incubated in the dark for 15–30 min at 37 °C. The reaction was stopped by adding 50 μl of stop solution to each well. The optical density (OD) of each well was measured at a wavelength of 450 nm within 5 min of adding the stop solution. A standard curve was generated from the OD values of the standard samples, and the concentrations of the proteins in the test samples were calculated accordingly. All plasma biomarker assays were performed in duplicate and averaged.
Statistical analysis
Data analysis was performed using SPSS software, version 26.0. The Shapiro–Wilk test was applied to determine the normality of the continuous variables. Continuous data that followed a normal distribution across the three groups were analyzed using one-way analysis of variance (ANOVA) followed by Bonferroni post hoc test, and the results were reported as means ± standard deviations. For continuous data that did not follow a normal distribution, the Kruskal–Wallis rank sum test was utilized, with results presented as medians with the 25th and 75th percentiles [M (P25, P75)]. Categorical data were compared using the chi-square test.
The diagnostic performance of the cognitive assessment scales and serum biomarker concentrations was evaluated using receiver operating characteristic (ROC) curve analysis. This method calculated the area under the curve (AUC) and determined the sensitivity and specificity of each test. GraphPad Prism version 8.0 was used for the generation of graphical representations of the data.
To investigate the relationships between serum NfL levels, age, and cognitive assessment scale scores across different groups, Spearman's rank correlation analysis was conducted. A P-value of less than 0.05 was considered statistically significant, indicating that the observed differences were unlikely to have occurred by chance.
Ethical approval
All participants had signed informed consent forms, and the study was approved by the Ethics Committee of the First Hospital of Hebei Medical University (Ethical Approval Number: 20190416).
Results
Demographic comparisons
The demographic analysis revealed no significant differences in gender, age, or educational level among the HC, MCI, and probable AD groups, ensuring comparability of the demographic data. The prevalence of hypertension and hyperlipidemia was also similar across the groups. However, significant differences emerged in the history of smoking, alcohol consumption, diabetes, and coronary heart disease among the participants (Table 1).
Cognitive function comparisons
Cognitive function assessments among the HC, MCI, and probable AD groups revealed significant differences in performance on the MoCA, MMSE, BNT, and DST. Both the MCI and probable AD groups scored significantly lower than the HC group on all cognitive tests, indicating a decline in cognitive function associated with disease progression (Table 2).
Serum biomarkers comparison
Upon comparing serum biomarkers among the HC, MCI, and probable AD groups, no significant differences were found in levels of IL-1β, TNF-α, and p-tau217. However, a notable difference was observed in serum IL-6 concentrations (F = 8.752, P = 0.013), with the MCI group exhibiting the highest levels, followed by the probable AD group, and the lowest in the HC group. Serum NfL concentrations also differed significantly across the groups (F = 7.582, P = 0.023), with the MCI group showing higher levels than the HC group. The MCI group's NfL levels were higher than those of the probable AD group, although this difference did not reach statistical significance. Aβ40 concentrations varied significantly among the groups, with the MCI group having the highest levels. Serum Aβ42 concentrations were significantly different across the groups, with the highest levels in the HC group and a significant difference between the HC and MCI groups. The Aβ42/Aβ40 ratio did not show a statistical difference (Table 3).
Correlation analysis between cognitive and hematological indicators
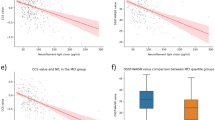
Spearman correlation analysis explored the relationships between serum NfL levels, inflammatory factors, and cognitive assessment scale scores. Age showed a positive correlation with IL-1β and Aβ40, but a negative correlation with Aβ42 and MMSE scores. Serum NfL was positively correlated with IL-1β and IL-6, as well as Aβ40, but no significant correlation was found with cognitive assessment scores. TNF-α correlated with Aβ42, Aβ40, and p-tau217. Aβ40 showed a positive correlation with DST scores (correlation coefficient = 0.288). Significant positive correlations were observed among the cognitive measurement scales (Table 4).
Sensitivity and specificity analysis of indicators predicting MCI
ROC curve analysis assessed the sensitivity and specificity of various blood and cognitive tests for predicting MCI. The BNT showed an AUC of 0.690, with a sensitivity of 0.773 and a cutoff value of 25.5. The DST had limited predictive ability, with an AUC of only 0.546(Fig. 1A). IL-6 demonstrated higher accuracy in predicting MCI compared to IL-1β and TNFα, with AUCs of 0.648, 0.595, and 0.562, respectively (Fig. 1B).

ROC analysis of different cognitive scales and blood indexes.Note: MoCA—Montreal Cognitive Assessment; MMSE—Mini-mental state examination; BNT—Boston naming test; DST—Digit span test; IL—Interleukin; TNFα—Tumor necrosis factor α; NfL—Neuroflament light chain; Aβ—β amyloid; p-tau—phosphorylated tau.
Serum NfL, Aβ42, Aβ40, and p-tau217 showed high specificity in predicting MCI, with Aβ40 outperforming the others (AUC = 0.707). The AUC for NfL was 0.646, and although p-tau217 had a lower AUC of 0.599, its specificity reached 0.907(Fig. 1C). Combining NfL with p-tau217 increased the predictive accuracy (AUC = 0.687), but combining NfL with IL-6 did not improve accuracy beyond that of NfL alone. The combination of NfL and BNT increased the accuracy of MCI prediction (AUC = 0.732) (Fig. 1D,E).
Gender differences in predicting MCI
Analysis of gender differences in the predictive accuracy of blood indicators and cognitive tests for MCI revealed that IL-6 predicted the highest AUC value for MCI in men. The combination of NfL and BNT improved the accuracy of identifying MCI in men (AUC = 0.777). In contrast, TNF-α was a more accurate predictor for MCI in women than other inflammatory indicators, while IL-6 was not a significant predictor for MCI in women. However, The AUC value of NfL combined with BNT for identifying MCI was not higher than BNT alone for in women (Table 5).
Discussion
The NfL protein, a neuron-specific element of the neuronal cytoskeleton, has been identified as a biomarker for neuronal damage, with elevated levels in CSF and blood linked to various neurological conditions, including multiple sclerosis, frontotemporal dementia, and Guillain–Barre syndrome26,27. Additionally, research has shown that higher CSF NfL concentrations correlate with compromised white matter integrity, as assessed by diffusion tensor imaging, suggesting that white matter damage is a primary contributor to memory decline in MCI28. Recent hypotheses propose that AD may be a chronic autoimmune disease, with cognitive decline closely associated with inflammatory processes17. Our study sought to explore the relationship between serum NfL, inflammatory factors, and cognitive function.
We observed that serum NfL levels were elevated in both the MCI and AD groups compared to the HC group, with the highest concentrations found in the MCI group. This aligns with previous findings29 and suggests that serum NfL levels begin to rise even before significant cognitive decline or impairment in daily living activities becomes apparent, offering potential implications for drug development and early intervention strategies. Longitudinal studies have indicated that higher baseline NfL levels are predictive of more rapid cognitive deterioration in individuals with MCI30. Furthermore, increases in plasma NfL levels have been associated with structural brain changes, including alterations in gray matter, white matter, and the cingulate gyrus, as well as with the volume of the lateral ventricles, hippocampus, and cortical thickness in AD patients31,32. The interaction between inflammatory processes and plasma NfL may also influence cognitive integrity through the disruption of core subsystems involved in AD progression and the frontoparietal network33.
In our study, serum IL-6 levels differed significantly across the groups, and IL-1β levels correlated with DST scores, suggesting that monitoring these cytokines could aid in the early detection of MCI in at-risk populations. The serum Aβ40 levels were higher in the MCI group and lower in the AD group, while serum Aβ42 levels were lowest in the MCI group and higher in the AD group compared to the MCI group. These findings contrast with some previous studies where Aβ40 and Aβ42 levels were found to be lower in MCI than in HC groups34. Other research indicates that plasma Aβ levels may decrease significantly during the AD stage, potentially due to changes in the blood–brain barrier permeability, lymphatic function, or activation of vascular components or microglia, leading to reduced clearance of Aβ from the CSF to the periphery35,36. Animal studies support this, suggesting that blood Aβ levels drop as Aβ begins to deposit in the brain37. The discrepancy in Aβ40 and Aβ42 levels observed in our study may reflect complex and as yet not fully understood mechanisms of Aβ production and clearance.
While previous research has indicated an association between age and NfL concentration38, our study did not observe this relationship. This discrepancy may be attributed to the different methodologies employed for quantifying blood NfL, such as ELISA, electrochemiluminescence immunoassay, and Single Molecule Array (Simoa), with Simoa being the most sensitive39. Due to its low cost, convenient operation, and the ability of key reagent antibodies to specifically bind to its target, ELISA has a low off target rate, which can produce high sensitivity and specificity results. Moreover, antibodies validated by ELISA can be replicated on a large scale. Previous studies have also used ELISA to detect NfL levels, a study utilizing ELISA also reported no correlation between age and NfL levels40. This suggests that the choice of detection method could significantly impact the observed correlations between NfL and age.
Our investigation into the correlation between NfL and inflammatory cytokines revealed a positive association between NfL and IL-1β and IL-6. This aligns with animal studies that have documented an increase in various inflammatory factors, including IL-2, IL-4, IL-6, and TNF-α, in conjunction with elevated CSF NfL in the context of chronic neuroinflammation and immune response41. These findings lend credence to the hypothesis that AD may be viewed as an innate autoimmune disease17. The association between NfL and Aβ40 suggests that axonal damage may play a significant role in the AD disease process, alongside the well-established roles of Aβ and tau pathology.
The relationship between inflammation and cognitive decline is widely acknowledged, yet the precise mechanisms and pathways of brain inflammation remain elusive. In the early stages of AD, the brain's neuroprotective mechanisms, such as amyloid clearance and antioxidant defenses, are believed to be effective. However, as AD progresses, stress-related upregulation of immune system mediators leads to an overproduction of pro-inflammatory molecules, resulting in brain inflammation. The accumulation of Aβ and the formation of neurofibrillary tangles in the AD brain can activate the immune system and trigger inflammatory stress. This sustained inflammatory response can create a positive feedback loop, culminating in irreversible neuronal damage42. Thus, we hypothesized that combining NfL with inflammatory markers might enhance the accuracy of MCI detection. However, our study did not support this hypothesis, which may be due to the limited sample size. Nonetheless, combining NfL with the BNT or p-tau217 improved diagnostic accuracy, highlighting the multifaceted nature of AD pathology and the limitations of relying on a single biomarker.
Autopsy studies have demonstrated a strong correlation between plasma p-tau217 levels and the extent of neurofibrillary tangles in AD patients, with p-tau217 showing high diagnostic performance in differentiating AD from other neurodegenerative diseases43. Although NfL is a marker of axonal injury and lacks specificity, as axonal damage can result from various neurological conditions, it still holds value in the early identification of MCI. Our findings suggest that the combination of NfL with p-tau217 can enhance the diagnostic accuracy for MCI, offering a potential avenue for future diagnostic approaches in AD.
Our study contributes to the understanding of AD by demonstrating correlations between NfL and other AD markers. Although most correlations were not statistically significant, this is consistent with previous studies32, suggesting that AD pathology is driven by diverse pathological conditions, such as Aβ pathology, tau pathology, and axonal degeneration, each eliciting different biomarker responses. Overall, the correlations between these biomarkers were weak, indicating the complexity of AD’s pathophysiological mechanisms.
Gender-based analysis in our study revealed that the diagnostic accuracy of certain biomarkers for MCI is inconsistent between males and females, which could be attributed to the small sample size. However, this observation may also reflect inherent gender differences in inflammatory responses. Previous research has indicated that sex may influence the regulation of pro-inflammatory and anti-inflammatory biomarkers44, and sex differences in inflammation have been reported45. While some studies suggest sex disparities in NfL levels46,47, the evidence is not yet conclusive, and further research with larger sample sizes is necessary to elucidate these potential differences.
The strength of this study lies in its integrative approach, combining serum NfL with inflammatory markers and other pathological indicators of AD, thereby shedding light on their interrelationships within the complex AD pathology. The inclusion of an elderly Eastern population provides valuable insights that are pertinent to our regional context and diversifies the demographic representation in AD research. Nevertheless, our study has limitations that warrant consideration. The small sample size and the regional confinement to Hebei Province may limit the generalizability of our findings. Additionally, the cross-sectional design precludes the ability to observe dynamic changes over time in the relationship between serum NfL, inflammatory markers, and cognitive function. The absence of neuroimaging data also means that we could not explore the association between serum NfL levels and brain structural changes.
Conclusion
This study underscores the potential of serum NfL as a biomarker for the early detection of MCI and AD, with elevated levels observed in affected individuals compared to healthy controls. The positive correlations between serum NfL and inflammatory cytokines IL-1β, IL-6, as well as Aβ40, highlight the multifaceted nature of AD pathology. While the combination of serum NfL with p-tau217 and the BNT enhances the predictive accuracy for MCI, the addition of inflammatory markers does not yield further improvement. These findings suggest that serum NfL, particularly when combined with other specific biomarkers, could serve as a valuable tool in the early identification of AD, thereby informing potential therapeutic strategies and interventions.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Lewczuk, P. et al. Plasma neurofilament light as a potential biomarker of neurodegeneration in Alzheimer’s disease. Alzheimers Res. Ther. 10(1), 71 (2018).
Patterson, C., World Alzheimer Report 2018The state of the art of dementia research: New frontiers. 48 (2018).
Ren, R. et al. The China Alzheimer Report 2022. Gen Psychiatr 35(1), e100751 (2022).
Teunissen, C. E. et al. Blood-based biomarkers for Alzheimer’s disease: Towards clinical implementation. Lancet Neurol. 21(1), 66–77 (2022).
Teunissen, C. E. & Khalil, M. Neurofilaments as biomarkers in multiple sclerosis. Multiple Sclerosis J. 18(5), 552–556 (2012).
Hampel, H. et al. Blood-based biomarkers for Alzheimer disease: Mapping the road to the clinic. Nat. Rev. Neurol. 14(11), 639–652 (2018).
Zetterberg, H. et al. Association of cerebrospinal fluid neurofilament light concentration with Alzheimer disease progression. JAMA Neurol. 73(1), 60–67 (2016).
Skillback, T. et al. CSF neurofilament light differs in neurodegenerative diseases and predicts severity and survival. Neurology 83(21), 1945–1953 (2014).
Rolstad, S. et al. Differential impact of neurofilament light subunit on cognition and functional outcome in memory clinic patients with and without vascular burden. J. Alzheimers Dis. 45(3), 873–881 (2015).
Egle, M. et al. Neurofilament light chain predicts future dementia risk in cerebral small vessel disease. J. Neurol. Neurosurg. Psychiatry 92(6), 582–589 (2021).
Osborn, K. E. et al. Cerebrospinal fluid and plasma neurofilament light relate to abnormal cognition. Alzheimers Dement. (Amst.) 11, 700–709 (2019).
Moreno, B. et al. Systemic inflammation induces axon injury during brain inflammation. Ann. Neurol. 70(6), 932–942 (2011).
Bourassa, K. & Sbarra, D. A. Body mass and cognitive decline are indirectly associated via inflammation among aging adults. Brain Behav. Immun. 60, 63–70 (2017).
Holmes, C. et al. Systemic inflammation and disease progression in Alzheimer disease. Neurology 73(10), 768–774 (2009).
Pillai, J. A. et al. Inflammatory pathway analytes predicting rapid cognitive decline in MCI stage of Alzheimer’s disease. Ann. Clin. Transl. Neurol. 7(7), 1225–1239 (2020).
Delaby, C. et al. NFL strongly correlates with TNF-R1 in the plasma of AD patients, but not with cognitive decline. Sci. Rep. 11(1), 10283 (2021).
Weaver, D. F. Alzheimer’s disease as an innate autoimmune disease (AD(2) ): A new molecular paradigm. Alzheimers Dement. 19, 1086–1098 (2022).
Zhang, Z. et al. The distribution characteristics of the results of mini-mental state examination for urban and rural residents aged 55 or above in Beijing. Chin. J. Neurol. 03, 4 (1999).
Yuan, Z. et al. The status of mild cognitive impairment in Chinese elderly and its influencing factors. J. Jining Med. Univ. 03(45), 6 (2022).
Fen, F. et al. The application of activity of daily living scale in dementia screening. J. Clin. Psychiatry 04, 2 (2004).
Tang, M. et al. Community-based follow-up study of mild cognitive impairment and dementia in the elderly. Chin. J. Psychiatry 04, 4 (2000).
Dubois, B. et al. Research criteria for the diagnosis of Alzheimer’s disease: Revising the NINCDS-ADRDA criteria. Lancet Neurol. 6(8), 734–746 (2007).
Yang, C. C. et al. Cross-cultural effect on suboptimal effort detection: an example of the digit span subtest of the WAIS-III in Taiwan. Arch. Clin. Neuropsychol. 27(8), 869–878 (2012).
Mariotto, S. et al. Serum and cerebrospinal neurofilament light chain levels in patients with acquired peripheral neuropathies. J. Peripher. Nerv. Syst. 23(3), 174–177 (2018).
Altmann, P. et al. Seven day pre-analytical stability of serum and plasma neurofilament light chain. Sci. Rep. 11(1), 11034 (2021).
Karantali, E. et al. The role of neurofilament light chain in frontotemporal dementia: A meta-analysis. Aging Clin. Exp. Res. 33(4), 869–881 (2021).
Moore, E. E. et al. Neurofilament relates to white matter microstructure in older adults. Neurobiol. Aging 70, 233–241 (2018).
Giacomucci, G. et al. Plasma neurofilament light chain as a biomarker of Alzheimer’s disease in subjective cognitive decline and mild cognitive impairment. J. Neurol. 269(8), 4270–4280 (2022).
Mattsson, N. et al. Association of plasma neurofilament light with neurodegeneration in patients with Alzheimer disease. JAMA Neurol. 74(5), 557–566 (2017).
Lin, Y. S. et al. Levels of plasma neurofilament light chain and cognitive function in patients with Alzheimer or Parkinson disease. Sci. Rep. 8(1), 17368 (2018).
Weston, P. S. J. et al. Longitudinal measurement of serum neurofilament light in presymptomatic familial Alzheimer’s disease. Alzheimers Res. Ther. 11(1), 19 (2019).
Mattsson, N. et al. Association between longitudinal plasma neurofilament light and neurodegeneration in patients with Alzheimer disease. JAMA Neurol. 76(7), 791–799 (2019).
Yao, W. et al. Inflammation disrupts cognitive integrity via plasma neurofilament light chain coupling brain networks in Alzheimer’s disease. J. Alzheimers Dis. 89(2), 505–518 (2022).
Shi, Y. et al. Potential value of plasma amyloid-beta, total tau, and neurofilament light for identification of early Alzheimer’s disease. ACS Chem. Neurosci. 10(8), 3479–3485 (2019).
Janelidze, S. et al. Plasma beta-amyloid in Alzheimer’s disease and vascular disease. Sci. Rep. 6, 26801 (2016).
Ramanathan, A. et al. Impaired vascular-mediated clearance of brain amyloid beta in Alzheimer’s disease: The role, regulation and restoration of LRP1. Front. Aging Neurosci. 7, 136 (2015).
Kawarabayashi, T. et al. Age-dependent changes in brain, CSF, and plasma amyloid (beta) protein in the Tg2576 transgenic mouse model of Alzheimer’s disease. J. Neurosci. 21(2), 372–381 (2001).
Baldacci, F., et al., Aging and sex impact plasma NFL and t‐Tau trajectories in individuals at risk for Alzheimer’s disease. Alzheimer's Dementia, 16(S4) (2020).
Kuhle, J. et al. Comparison of three analytical platforms for quantification of the neurofilament light chain in blood samples: ELISA, electrochemiluminescence immunoassay and Simoa. Clin. Chem. Lab. Med. 54(10), 1655–1661 (2016).
Sailimu, M. et al. The role of neurofilament light chain protein in the early diagnosis of Alzheimer’s disease. J. Chongqing Med. Univ. 46(11), 5 (2021).
Hsiao, T.-C. et al. Serum neurofilament light polypeptide is a biomarker for inflammation in cerebrospinal fluid caused by fine particulate matter. Aerosol Air Qual. Res. 20(7), 1665–1674 (2020).
Casoli, T. et al. Peripheral inflammatory biomarkers of Alzheimer’s disease: The role of platelets. Biogerontology 11(5), 627–633 (2010).
Heneka, M. T. et al. Neuroinflammatory processes in Alzheimer’s disease. J. Neural Transm. (Vienna) 117(8), 919–947 (2010).
McNaull, B. B. et al. Inflammation and anti-inflammatory strategies for Alzheimer’s disease–a mini-review. Gerontology 56(1), 3–14 (2010).
Pan, M. H., Lai, C. S. & Ho, C. T. Anti-inflammatory activity of natural dietary flavonoids. Food Funct. 1(1), 15–31 (2010).
Lerche, S. et al. CSF and Serum levels of inflammatory markers in PD: Sparse Correlation, sex differences and association with neurodegenerative biomarkers. Front. Neurol. 13, 834580 (2022).
Sass, D. et al. Sex differences in behavioral symptoms and the levels of circulating GFAP, Tau, and NfL in Patients with traumatic brain injury. Front. Pharmacol. 12, 746491 (2021).
Acknowledgements
This study was supported by the Special Fund Project of the Central Government to Guide the Local Science and Technology Development of Hebei Province [Grant Numbers 199477138G], Science and Technology Program of Hebei Province [Grant Numbers SG2021189], The government funded clinical medicine excellent talents training project of Hebei Province [Grant Numbers ZF2024136]. X. Jing and L. Wang contributed equally to this work.
Author information
Authors and Affiliations
Contributions
J.X.: Investigation, Formal analysis, Data curation, Writing-original draft. W.L.: Investigation, Writing-original draft. S.M.: Investigation, Funding acquisition. G.H.: Investigation. L.W.: Investigation. H.Y.: Investigation. H.A.: Investigation. W.X.: Conceptualization. A.C.: Conceptualization, Funding acquisition, Writing –review & editing.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jing, X., Wang, L., Song, M. et al. Serum neurofilament light chain and inflammatory cytokines as biomarkers for early detection of mild cognitive impairment. Sci Rep 14, 9072 (2024). https://doi.org/10.1038/s41598-024-59530-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-59530-5
Keywords
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
