
Abstract
Inspiratory muscles pre-activation (IMPA) has been studied to improve subsequent performance in swimming. However, the effects of IMPA on various parameters in swimmers are still unknown. Therefore, this study aimed to investigate the effects of IMPA on the mechanical parameters, physiological responses, and their possible correlations with swimming performance. A total of 14 young swimmers (aged 16 ± 0 years) underwent a 30-s all-out tethered swimming test, preceded or not by IMPA, a load of 40% of the maximal inspiratory pressure (MIP), and with a volume of 2 sets of 15 repetitions. The mechanical (strength, impulse, and fatigue index) and physiological parameters (skin temperature and lactatemia) and the assessment of perceived exertion and dyspnea were monitored in both protocols. The IMPA used did not increase the swimming force, and skin temperature, decrease blood lactate concentration, or subjective perception of exertion and dyspnea after the high-intensity tethered swimming exercises. Positive correlations were found between mean force and blood lactate (without IMPA: r = 0.62, P = 0.02; with IMPA: r = 0.65, P = 0.01). The impulse was positively correlated with blood lactate (without IMPA: r = 0.71, P < 0.01; with IMPA: r = 0.56, P = 0.03). Our results suggest that new IMPA protocols, possibly with increased volume, should be developed in order to improve the performance of young swimmers.
Similar content being viewed by others


Introduction
The Pre-activation (PA) strategy potentially promotes muscle activation by increasing body temperature to better prepare the body for a subsequent activity, which can improve performance1,2. The inspiratory muscles pre-activation (IMPA) protocol, which has been the subject of many studies in the field of sports, is a potential way of preceding main efforts and improving physical and sport performance3,4,5,6,7. Special attention has been given to this strategy since during high-intensity exercises there is an increase in inspiratory muscles (IMs) activity, leading to hyperventilation, early fatigue and a concomitant decrease in performance8, which appears to be minimized when IMPA is used, mainly due to the delay in the inspiratory muscle metaboreflex9,10.
In the case of swimming, the IMs are susceptible to adaptations that increase the forced and vital inspiratory volume as a result of the mechanicals movement of the upper limbs for propulsion and immersion of the face in the water, enhancing resistance to fatigue and/or swimming performance10,11,12. Considering that these muscles are very active and to can contribute to the maintenance and quality of swimming12, IMPA could be applied in this sport, as it can minimize the effects of double mechanical demand of IMs, improving ventilation and spinal stabilization13. However, most studies in this field have focused on IMs training14,15,16,17,18 and, to the best of our knowledge, only one investigated IMPA5, obtaining positive results of this intervention on performance.
To date, the literature lacks positive results on the potential effects of IMPA on physiological parameters in different sports3,4,7,19,20,21, with no studies dedicated to swimming. Taking into account that IMPA can attenuate energy expenditure and heat dissipation through IMs metaboreflex22,23, the assessment of blood lactate responses, rating of perceived exertion, and especially skin temperature (ST) could help verify possible changes in physiological parameters.
With the technological advances, it is now possible to obtain thermographic records of athletes' skin in their own training and competition environment is a non-invasive and rapid way24,25, assisting in sports to monitoring26,27. In addition, blood lactate as a physiological parameter and subjective perceived exertion and dyspnea as psychophysiological measures are widely used after physical exertion as markers to determine the level of exertion and recovery, as they are practical to collect and quick to obtain results28,29,30,31. Therefore, this gap could be minimized by analyzing these parameters at different times after the application of IMPA with physical effort in swimming.
A protocol that has been widely used to study the physiological and mechanical aspects of high-intensity, short-duration exercises is the 30-s all-out32,33. Classically proposed by Bar-or34 on a cycle ergometer (Wingate test), this test has been applied to other types of exercise such as running35,36 and swimming37,38. In the last modality can be applied with the adoption of a sensorized swimming system, which can provide force data and determine impulse and fatigue index accurately, respecting the individuality and specific motor gesture required by the sport39,40.
Finally, the 30-s all-out effort is characterized by a predominantly anaerobic stimulus that increases physiological responses such as heart rate and blood lactate production37,38. And after this high-intensity test, there is a significant participation of the aerobic metabolism in the recovery process, which ends up restoring energy stores41. In this sense, the adoption of the 30-s all-out swimming test seems promising to assess the possible impact of IMPA on the subsequent performance of swimmers, with refined measurements and a high frequency of signal acquisition.
In summary, the present study establishes a connection among knowledge about IMPA, physiological measurements and mechanical swimming performance with gaps in the modulation of skin temperature in target regions possibly due to IMPA. Through the use of precise tools, we aim to investigate the effects of IMPA on mechanical and physiological parameters, and their possible correlations with tethered swimming performance. Our hypothesis is, that IMPA will enhance swimming performance, consequently increasing force and swimming impulse and reducing the fatigue index during the 30-s all-out test. We also speculate that IMPA, combined with swimming warm-up, will increase skin temperature and reduce in the sensation of dyspnea responses that we expect to be positively correlated with performance.
Methods
Participants
Fourteen young athletes of both genders (8 males, aged 16 ± 0 years; and 6 females, aged 15 ± 0 years), at competitive levels ranging from regional and state championships in São Paulo, Brazil, to the Brazilian Youth and Junior Swimming Championships (FINA points—SCM: 356 ± 19; LCM: 386 ± 25) participated in the study. Sample size was calculated by G*power software (G*Power version 3.1.9.7 Uiversität Kiel, Germany), that suggested 10 participants to obtain a significant statistical power (sample power 0.95 and α 0.05). As inclusion criteria, we considered athletes with swimming training (at least 2 years) who performed an average of 16 h of training per week, participated in competitions (at least at the regional level), and without history of pulmonary diseases. All procedures were approved by the Research Ethics Committee of the School of Medical Sciences of UNICAMP (protocol no. 39132120.2.0000.5404). The participants and their legal guardians were informed about the procedures and signed the Informed Consent and Assent Form, free and clear. The subjects were instructed not to consume alcoholic beverages or caffeine, not to perform strenuous physical exercises and to maintain a balanced diet throughout the experimental protocol described here in.
Study design
All protocols were conducted in the athletes' own training environment. The swimmers were submitted to three assessment sessions, separated by an interval of 24 to 48 h. The first one consisted of the explanation of the research objectives, the application of questionnaires about the participants’ sports history and physical activity level, and the familiarization with equipment (manovacuometer and POWERbreathe® breathing exerciser). Afterwards, they were submitted to anthropometric measurements and assessment of both maximal inspiratory pressure (MIP) and global strength index (S-Index), as detailed below. Lastly, the athletes were familiarized with the ergometer in the pool. In the two subsequent visits, they underwent the all-out tethered swimming test, preceded or not by IMPA at a load equivalent to 40% of the individual MIP (2 sets of 15 repetitions, with 1 a minute interval between sets) (Fig. 1). In both conditions, the swimmers performed a warm-up (WU) with specific swimming gestures (400 m crawl, at intensities from low to moderate), followed by a 5-min passive recovery prior to the tests. The swimming force, impulse, and fatigue index (FI) were collected in these two sessions. The thermographic records were obtained in the last minute of rest, right after the warm-up, before the IMPA protocol, and in the 1st minute of the end of the tethered swimming test. Blood samples were collected at rest, immediately after the all-out effort and at minutes 3, 5, 7 and 10 of passive recovery. Rating of perceived exertion (RPE) and rating of perceived dyspnea (RPD) were also measured at rest, after WU, after all-out, and at minutes 5 and 10 of passive recovery. All procedures were performed at the same time of day, in a 25 m indoor pool with water temperature maintained at 25 °C, following the rules of the International Swimming Federation (FINA).

Experimental design used in the study (timeline configuration for the exercise and inspiratory muscle pre-activation (IMPA) session). Randomly, each subject underwent two experimental sessions, one in the control condition and the other with IMPA. Temporal representation of the interventions performed before, during and after the tethered swimming exercise during which the force recordings occurred. Thermographic records (skin temperature - ST), blood lactate samples and rating of perceived exertion (RPE) and dyspnea (RPD) were obtained during all the assessment sessions in the time windows shown.
Anthropometric parameters and body composition
For the anthropometric and body composition analysis, the body mass (kg) was measured using a portable digital scale (Multilaser®) with a maximum capacity of 180 kg and precision of (100 g), along with measurements height (cm), body circumferences (cm), wingspan (cm) and humeral and femoral biepicondyle diameters (cm) with the aid of a bone caliper and a Cescorf® flexible anthropometric tape measure. The body fat percentage (%) was estimated following the proposal of Jackson and Pollock42 for men and Jackson et al.43 for women, where the sum of the seven body folds refers to the sum of the thickness of the pectoral middle axillary skinfolds, triceps, subscapular, abdomen, supra iliac and middle thigh skinfolds for men and, the sum of the thickness of the triceps, thigh, and supra iliac skinfolds (measured by a Cescorf®, adipometer, mm) for women. All measurements were performed by the same evaluator in triplicate, taking the median of the three measurements.
Maximal inspiratory pressure and S-index determination
The respiratory muscle strength was assessed by MIP (cmH2O) using a manovacuometer (± 300 cmH2O, GER-AR, São Paulo, SP, Brazil). This non-invasive device has a plastic mouthpiece connected to a small hole (2 mm) to prevent glottic closure. This assessment was conducted by a trained researcher who demonstrated the correct performance of the respiratory maneuver. In the sitting position, the measurement was started from the residual volume and signaled for the athletes to perform a strong and fast inspiration in the total lung capacity. Their nose was occluded throughout the effort. To obtain the best value, all subjects performed three to five attempts, with a 1-min interval between measurements and MIP. The highest value was the one that did not exceed 10% of the difference between attempts21. The S-Index (cmH2O), was assessed with the aid of an inspiratory device (PowerBreathe K5, IMT Technologies Ltd., UK) in the orthostatic position and with nasal occlusion. Thirty dynamic inspirations were performed with open air flow with the participant exhaling slowly and inhaling the greatest capacity of air quickly and deeply. The peak and mean S-Index corresponded to the highest and average values in the 30 inspirations, respectively21. This measurement is derived from mean peak inspiratory flow (PIF) and volume measurements. The MIP and S-Index (mean and peak) measurements are also presented relatized to the athletes' body mass.
30-second all-out tethered swimming test
The protocol for determining the mechanical parameters followed the instructions suggested by Papoti et al.40, using a tethered swimming system also applied in canoeing44. This apparatus consists of a suction cup, a load cell, an elastic cable, a signal amplifier, and software for digital acquisition. The load cell (CSL/ZL250, MK Controle e Instrumentação Ltda™, Brazil), coupled to the suction cup (Vonder™) was attached to the rear exit goal, always maintaining the same goal, by nylon clamps, attached to the elastic cable (Altaflex) laced on the swimmer. In both protocols (with or without IMPA), the force signals obtained through load cell deformation were amplified (MKTC5-10®, MK™ control and instrumentation) and processed in a signal conditioning module (USB-6008® National Instruments™). The signals were captured at a frequency of 1000 Hz and transmitted to specific digital acquisition software (LabView Signal Express®, National Instruments™). The system was calibrated before the tests using a dynamometer (Crown®, 20kgf, Oswaldo Filizola Ltda™) in which the load cell was placed in the vertical position and subjected to different force. Regression equations obtained in the calibration procedure were used to convert signals (mv) to force units (N). After the acquisition, the mechanical data, i.e., the variations of force (N), the impulse (N.s), calculated by the area under the curve of the trapezoidal method, and the fatigue index (%), calculated by the equation (maximum force − minimum force)/maximum force × 100, were treated using Microsoft Excel® software.
Inspiratory muscles pre-activation (IMPA) by airflow restriction
After determining the MIP using a manovacuometer and identifying the S-Index, IMPA was performed with the aid of an inspiratory muscle exerciser (POWERbreathe—model K5). The IMPA protocol with airflow restriction was based on the study by Cirino et al.21 and Marostegan et al.36. The swimmers performed 2 sets of 15 maximum inspirations, with a 1-min interval between the sets and were encouraged to maintain a diaphragmatic inspiratory muscle pattern. The IMPA was performed in the standing position and outside the pool, at 40% of the MIP. Two minutes after the intervention, the athletes were submitted to the tethered swimming test.
Infrared thermography
Temperature records were obtained by a FLIR® thermographic camera, model One Pro for IOS (19,200 pixels), which has thermal sensitivity to measure temperatures ranging from − 20 to 400 °C, at a resolution of 0.1° W. A specific space was allocated for the thermographic camera to always be positioned in the same place. The recordings were made at an average ambient temperature of 20 °C (2 °C), recorded at the time of collection24,25,27. To minimize extrinsic interference, the camera was turned on 30 min before the beginning of the recordings and the participants were kept at rest for a period of 5 min in the recording location, wearing only bathing suits (swimming trunks and sunkini) so that the physiological responses remained stable and the thermal equilibrium was reached. To acquire the images, the athletes were instructed to stand at 2.5–3 m from the thermographic camera (the distance variation depended on the athlete's height). Two images (front and back views) were captured for each moment analyzed in JPG format (640 × 480 pixels) with skin temperature extraction. The skin temperature was quantified by regions of interest, namely, thorax (chest, abdomen and back), upper limbs (biceps brachii and triceps brachii), lower limbs (quadriceps, ischiotibials and triceps surae) and face, using FLIR® Thermal Studio Starter software (version 1.90.10). All records were collected by a single researcher.
Blood lactate concentration and, rating of perceived exertion and dyspnea
For the analysis of blood lactate concentrations, blood samples (25 µL) were collect from the earlobe, using heparinized and calibrated capillaries. The samples were stored in Eppendorf tubes (1.5 ml) containing 50 μl of 1% sodium fluoride (NaF) and analyzed in an electrochemical Lactate Analyzer (YSI-2300-STAT-Plus™, Yellow Springs, OH, USA Ohio, USA). The Rating of Perceived Exertion (RPE)30 and Rating of Perceived Dyspnea (RPD)45 were also applied.
Statistical analysis
All results obtained are expressed as mean ± standard error of the mean (SEM). The normality and homogeneity of the data were tested by Shapiro–Wilk Levene's tests, respectively. Parametric statistics was employed and the normal distribution of data was observed. Two-way ANOVA for repeated measures followed by Newman–Keuls post-hoc was adopted to analyze the effects of pre-activation (with and without IMPA) and time on skin temperature in the body regions of interest, blood lactate, RPE, RPD, and strength scores. Student's t-test was used for dependent samples to identify the effect of IMPA on the physiological responses in the post all-out moment and the mechanical outcomes (peak force, mean force, impulse, fatigue index in, absolute values and relativized to body mass). Person's product-moment test was employed to verify the correlation between physiological responses and the results obtained in the tethered test performed with or without IMPA. The effect size (ES) and Power (1 − β) were calculated for each paired comparison and two-way ANOVA for repeated measures analyzes from variances. The ES was classified small, medium, and large when ≤ 0.49, 0.5 to 0.79, and ≥ 0.8, respectively. The statistical analyses were performed using STATISTICA® (7.0 version). In all cases, the significance level was set at P < 0.05.
Ethics approval and consent to participate
This study was conducted in agreement with the ethical recommendations of the Declaration of Helsinki and all experiments were approved by the Research Ethics Committee of The School of Medical Sciences (protocol number 39132120.2.0000.5404). After having received information about the experimental procedures and risks, all individual participants (and their legal guardians when under 18 years old) signed an informed consent form declaring to be aware about the study design, the exercise conditions, and the publication of results, and that no details about the individuals would be reported in the manuscript.
Results
The results of the anthropometric, body composition and inspiratory parameters for male and female swimmers are listed in Table 1, together with the total group results (male and female, n = 14).
Mechanical parameters
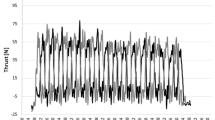
The results of relativized force (N.kg−1) for the total number of participants (n = 14) are illustrated in Fig. 2A, which shows the relativized mean force in each second during the all-out tethered swimming test (30 s) for both sessions (without and with IMPA). No significant differences were found between the relativized force values of the sessions with and without IMPA during the all-out tethered swimming test.

(A) Force relativized to body mass (N kg−1) during the tethered swimming trials (all-out) with and without IMPA. The impulse (N s) is represented in grey by the area over the curve of the trapezoidal method. (B) Table of the mechanical parameters with and without IMPA. Values taken as mean and statistical difference in interaction with P < 0.05 (n = 14).
Figure 2B compares the mechanical data results (i.e., mean absolute force, peak absolute force, relative mean force, relative peak force, impulse, and fatigue index) between the sessions performed without and with IMPA. No difference was observed between the sessions for any of the mechanical variables studied.
Physiological parameters
Table 2 presents the physiological and perceptual results measured immediately after the exercise sessions performed without and with IMPA. For all variables reported, total skin temperature, blood lactate, and rating of perceived exertion and dyspnea showed no significant differences between the sessions.
The skin temperature results observed in the lower and upper limbs are shown in Figs. 3 and 4, respectively. There was no effect of IMPA on total skin temperature (F = 0.24; P > 0.05) and no interaction between the skin temperature values at different times for both conditions (with and without IMPA), except for the left ischiotibial (LI) temperature (F = 2.85; P= 0.04), which indicates that the thermal variation over time was different between the sessions. However, the post hoc result reveals, that the difference was evidenced immediately before IMPA application in the post all-out moment in both conditions, viewed separately (without IMPA: P < 0.05; with IMPA: P< 0.01). The effect of time on skin temperature was observed in different lower and upper muscle limbs (Figs. 3 and 4, respectively).

Lower limb skin temperature (mean ± standard error of the mean) at four collected time points (at rest, after warm-up, before IMPA and after the all-out swimming test) in different conditions (with and without IMPA). A, D = significant difference compared to rest; b, e = significant difference compared to the time after WU; and C, F = significant difference compared to the time before IMPA application; (G) anterior and posterior views of the lower limb skin temperature in the anatomical position; P < 0.05.

Upper limb skin temperature expressed as mean ± standard error of the mean at four collected times (at rest, after warm-up, before IMPA and after the all-out swimming test in different conditions (with and without IMPA). A, D = significant difference compared to rest; b, e = significant difference compared to the moment after WU; and C, F = significant difference compared to the moment before IMPA application; (I) anterior and posterior views of the upper limb skin temperature in the anatomical position; P < 0.05.
Finally, the results of the rating of perceived exertion, rating of perceived dyspnea and lactatemia are displayed in Fig. 5. There were no statistical differences between the conditions (without and with IMPA) for these responses and no interaction between this effect and time. The exception is the effect of time found when comparing moments within the same session.

Physiological and psychophysiological parameters before and after the all-out tethered swimming test. (A) Rating of perceived exertion and (B) rating perceived dyspnea without and with IMPA: a, e = significant difference in relation to rest; b, f = significant difference in relation to the moment after WU; c, g = significant difference in relation to the moment after the all-out swimming test; and d, h = significant difference in relation to minute 5. (C) Blood lactate (mM) without and with IMPA: a, f = significant difference with respect to rest; b, g = significant difference with respect to minute 1; c = significant difference with respect to minute 3; d = significant difference with respect to minute 5; and e = significant difference with respect to minute 7. Results expressed as mean and standard error of the mean; P < 0.05.
Correlations between mechanical and physiological parameters
Person's product-moment test was used to identify possible significant correlations between mechanical and physiological responses (Table 3). The results indicated significant correlations between mean force and blood lactate responses for all sessions and RPE for the session without IMPA, in addition to significant correlations between impulse and lactate for all sessions. Nonetheless, no significant correlation was found between fatigue index and the other physiological parameters assessed at the end of the tethered swimming test.
Discussion
Our study analyzed the effects of IMPA on the physiological (ST, lactacidemia, RPE and RPD) and mechanical (strength, impulse, and FI) parameters in an all-out swimming test. Contrasting with our hypothesis, IMPA did not improve the performance of young swimmers subjected to a tethered swimming test, since no significant differences were observed, both in the mechanical parameters during the test and in the physiological responses after the protocol (ST in different regions of the body, total ST, lactacidemia, RPE and RPD). Significant correlations between force and blood lactate were identified. There was also a significant correlation between impulse and blood lactate concentrations in both tests (preceded or not by IMPA).
Swimming predominantly involves the activation of the upper body muscles, thus requiring greater muscle force to maintain the swimming quality46. Based on this idea, with the application of IMPA the demand for swimming force would be attenuated by the increase in blood flow to the locomotor muscles during the activity, which was not demonstrated herein. Our results differ from those reported in studies conducted with the same PA protocol in running36 and handball10. What distinguishes this sport from those performed on the ground is the position of the body, in which the subject remains horizontal throughout the activity. In addition, hydrostatic pressure acts on the chest wall, resulting in higher inspiratory pressures without requiring the individual to increase the work of the diaphragm12.
Considering the above, our hypothesis may not have been confirmed due to the increase in pleural pressure and lung volume, as the individual may simply be floating in the water, causing changes in their physical responses in order to adapt to an environment that is not natural for the body12. It should also be noted that, although important for the refined acquisition of mechanical signals, in this study the athletes were tethered to an elastic cable, which also increases the load imposed during swimming. This differs from the work developed by Wilson et al.5, who reported positive effects of IMPA on the swimmers' performance, but in freestyle swimming. In our case, it is possible that swimming in a tethered position may have contributed, albeit involuntarily, to an elevated inspiratory pressure during the stroke—an effect that was not overridden with the application of the IMPA protocol.
Furthermore, in the case of tethered swimming, the physical demands of the test are associated with the predominant use of alactic and lactic anaerobic capacities since the effort is maximal, characterized by high intensity and short duration (30 s all-out)47. During high-intensity efforts, the body increases the cardiac output, which in turn elevates the pulmonary vascular pressure and restricts O2 transport, increasing IM fatigue. The inspiratory metaboreflex ultimately impairs the redistribution of blood to the most active muscles during exercise48,49. According to the literature, the attenuation of the IM metaboreflex with IMPA would improve performance by reducing energy expenditure and heat dissipation22,23, which was not observed in our results.
In addition to performance-related variables, studies conducted in sports other than swimming reported positive effects on physiological responses when different IMPA protocols were used3,4,6,20,36. In these studies, the only parameters evaluated that were similar to those used herein were RPE and RPD, and in our specific case, there were no differences between the two experimental conditions (without and with IMPA). The RPE examined showed an inverse correlation with mean force for the session without IMPA since the participants who showed lower force scores reported higher RPE values. Moreover, the greater the perceived intensity of breathlessness, the greater the maximum force used by the IMs to breathe in proportional values50, resulting in higher blood flow to deliver O2 and maintain or increase IM strength, and consequently compromising blood flow to the locomotor muscles51. Lastly, there was no correlation between swimming force and RPE and RPD in the session with IMPA, suggesting that the IMPA proposed herein slowed, perhaps in a simple way, the increase in blood flow to the IMs because these muscles were already activated.
In our study, even though lactacidemia was not influenced by the application of IMPA, a positive and significant correlation was found between blood lactate and force and impulse, confirming that the individuals who performed better in the tethered test stimulated the lactic anaerobic pathway in a more pronounced way. These results are consistent with those found in the literature, evidencing that post-exercise blood lactate is a critical marker of the level of exertion and recovery and that this response is directly related to the physical effort exerted28,29. Other studies also failed to show positive effects of IMPA on the physiological variables analyzed3,4,7,19,20,21. On the other hand, from the qualitative results it was possible to observe positive responses when the athletes were asked about their performance in the tests. Several reported "greater ease of swimming", "longer apnea time during swimming", "faster recovery from fatigue at rest" and "less breathlessness" when the efforts were performed in the IMPA session. These reports are similar to those found in other studies using respiratory equipment for IM training, in which the participants reported "less feeling of dyspnea" and "less chest tightness during exercise"20,52.
Regarding the results obtained from skin temperature measurements analyzed in a segmented manner in specific regions, we again did not observe the effect of IMPA, contrary to our expectations. Greater heat production is strongly related to increased activity of the muscles during effort and exercise intensity25,53,54. Additionally, a proportional increase in muscle temperature can be associated with an enhancement in performance, favoring muscle metabolism and increasing the speed of nerve impulse transmission to the muscles, strength, and agility1,55. On the other hand, during physical activity the skin temperature does not respond in the same way as the muscle temperature54,55. During swimming, there is a decrease in temperature compared to the responses before the beginning of swimming due to the contact of the body with water and an abrupt increase in temperature when the swimmer leaves the water56. This behavior was observed in our study in the different skin regions analyzed (Figs. 4 and 5), but without any changes caused by the respiratory intervention before the swimming effort.
One factor that may limit the assessment of temperature in the swimming modality is the clothing worn by the athletes. In the present study, although the athletes used towels to dry themselves after the test so that the thermographic images could be taken, the swimwear and/or sunkini evaluated remained damp, with the residual water running down the body. Despite this limitation and the non-identification of the effects of IMPA on skin temperature responses, we suggest the inclusion of this measure in future investigations involving swimming so as to allow these findings to be further explored in a sporting context53.
Another limiting factor of our study is that the intervention chosen (2 × 15 at 40% of the individual MIP with a 1-min rest interval between sets) did not positively modify the dependent variables studied for the target sport. The choice of protocol was based on the positive PA findings in other sports21,36,57, as well as its easy applicability and short execution time. The vast majority of studies in the current literature use a volume of 2 sets of 30 repetitions, with positive effects on physiological, inspiratory, and mechanical parameters9,12. The load used in our protocol (40% of the MIP) was in line with previous studies that selected this inspiratory load because it represents the highest intensity at which inspiratory muscle fatigue is not induced9,58.
In contrast, Wilson et al.5 applied IMPA in conjunction with a swimming-specific warm-up (without an interval between the overall warm-up and IMPA) with a volume of 2 sets of 30 repetitions to evaluate professional swimmers who performed IMPA and then a 100 m freestyle test compared to a control group. On this occasion, the authors found a reduction in the 100 m test time when the swimmers performed the effort post to the IMPA protocol. Considering that the IMs of swimmers are already highly demanded during swimming12, resulting in increased IM strength and lung size compared to land-based athletes59, the shorter IMPA strategy (2 × 15 repetitions) may not have been characterized as a sufficient stimulus to induce a brief but effective effort of the IM to improve swimming performance based on an anaerobic stimulus.
Like other investigations7,60, our study did not find positive effects of IMPA on performance and physiological responses. Nevertheless, our study is the pioneer in the application of IMPA in tethered swimming, in an attempt to associate mechanical and physiological variables in order to expand knowledge of the effects of this warm-up strategy. We also made progress in skin temperature monitoring, which requires specific equipment for detection. In conclusion, IMPA can be incorporated into training routines and competitions since it is a mobile, easy to use, non-invasive, legal, and safe protocol. Therefore, we emphasize the importance of further studies using IMPA in swimming, so as to expand the application of this stimulus to different categories, including before other longer swimming trials, both in tethered and freestyle, thus contributing to the scientific advancement of this modality and improving the performance of swimmers.
Conclusions
Our results indicate that the inspiratory warm-up protocol (2 sets of 15 repetitions with a 1 min interval) at 40% of the MIP did not improve the force of swimmers in a high-intensity (30 s all-out) tethered swimming protocol. In addition, IMPA, at least as applied here, did not increase skin temperature, reduce blood lactate concentrations, or rating of perceived exertion and dyspnea immediately after the tethered swimming test. On the other hand, positive reports of the use of inspiratory muscles pre-activation were signaled by the athletes, reinforcing the importance of further studies using this strategy in swimming.
Data availability
All relevant data are in the manuscript. For additional information, the data will be made available upon request by contacting the corresponding author (Fulvia B Manchado-Gobatto).
References
Bishop, D. Warm up II: Performance changes following active warm up and how to structure the warm up. Sports Med. 33, 483–498 (2003).
Silva, L. M., Neiva, H. P., Marques, M. C., Izquierdo, M. & Marinho, D. A. Effects of warm-up, post-warm-up, and re-warm-up strategies on explosive efforts in team sports: A systematic review. Sports Med. 48, 2285–2299 (2018).
Lin, H. et al. Specific inspiratory muscle warm-up enhances badminton footwork performance. Appl. Physiol. Nutr. Metab. 32, 1082–1088 (2007).
Cheng, C.-F. et al. Inspiratory muscle warm-up attenuates muscle deoxygenation during cycling exercise in women athletes. Respir. Physiol. Neurobiol. 186, 296–302 (2013).
Wilson, E. E. et al. Respiratory muscle specific warm-up and elite swimming performance. Br. J. Sports Med 48, 789–791 (2014).
Özdal, M., Bostanci, Ö., Dağlioğlu, Ö., Ağaoğlu, S. A. & Kabadayi, M. Effect of respiratory warm-up on anaerobic power. J. Phys. Ther. Sci. 28, 2097–2098 (2016).
Barnes, K. R. & Ludge, A. R. Inspiratory muscle warm-up improves 3,200-m running performance in distance runners. J. Strength Cond. Res. 35, 1739–1747 (2021).
F. Rodriguez, R., J. Aughey, R. & Billaut, F. in Respir. Physiol. (IntechOpen, 2020).
Cirino, C. et al. Effects of inspiratory muscle warm-up on physical exercise: a systematic review. Biology (Basel) 12, 333 (2023).
Burtch, A. R. et al. Controlled frequency breathing reduces inspiratory muscle fatigue. J. Strength Cond. Res. 31, 1273–1281 (2017).
Noriega-Sánchez, S. A. et al. Forced inspiratory volume in the first second as predictor of front-crawl performance in young sprint swimmers. J. Strength Cond. Res. 29, 188–194 (2015).
Leahy, M. G. et al. The mechanics of breathing during swimming. Med. Sci. Sports Exerc. 51, 1467–1476 (2019).
Hodges, P. W., Butler, J. E., McKenzie, D. K. & Gandevia, S. C. Contraction of the human diaphragm during rapid postural adjustments. J. Physiol. 505, 539–548 (1997).
Muranaka, M., Suzuki, Y., Ando, R. & Sengoku, Y. Change in short distance swimming performance following inspiratory muscle fatigue. J. Sports Med. Phys. Fitness 61, 1433–1440 (2021).
Ohya, T. et al. Effect of moderate- or high-intensity inspiratory muscle strength training on maximal inspiratory mouth pressure and swimming performance in highly trained competitive swimmers. Int. J. Sports Physiol. Perform. 17, 343–349 (2021).
Cunha, M. et al. The effect of inspiratory muscle training on swimming performance, inspiratory muscle strength, lung function, and perceived breathlessness in elite swimmers: a randomized controlled trial. Porto Biomed. J. 4, e49 (2019).
Kilding, A. E., Brown, S. & McConnell, A. K. Inspiratory muscle training improves 100 and 200 m swimming performance. Eur. J. Appl. Physiol. 108, 505–511 (2010).
Yañez-Sepulveda, R. et al. Inspiratory muscle training improves the swimming performance of competitive young male sprint swimmers. J. Sports Med. Phys. Fitness 61, 1348–1353 (2021).
Arend, M., Kivastik, J. & Mäestu, J. Maximal inspiratory pressure is influenced by intensity of the warm-up protocol. Respir. Physiol. Neurobiol. 230, 11–15 (2016).
Tong, T. K. & Fu, F. H. Effect of specific inspiratory muscle warm-up on intense intermittent run to exhaustion. Eur. J. Appl. Physiol. 97, 673–680 (2006).
Cirino, C. et al. Complex network model indicates a positive effect of inspiratory muscles pre-activation on performance parameters in a judo match. Sci. Rep. 11, 11148 (2021).
Mcconnell, A. K. & Lomax, M. The influence of inspiratory muscle work history and specific inspiratory muscle training upon human limb muscle fatigue. J. Physiol. 577, 445–457 (2006).
Volianitis, S. et al. Inspiratory muscle training improves rowing performance. Med. Sci. Sports Exerc. 33, 803–809 (2001).
Adamczyk, J. G., Krasowska, I., Boguszewski, D. & Reaburn, P. The use of thermal imaging to assess the effectiveness of ice massage and cold-water immersion as methods for supporting post-exercise recovery. J. Therm. Biol. 60, 20–25 (2016).
Fernández-Cuevas, I. et al. Classification of factors influencing the use of infrared thermography in humans: A review. Infrared Phys. Technol. 71, 28–55 (2015).
Brito, C. J. et al. Immune response related with skin thermal pattern in judokas: A new application for infrared thermography?. J. Strength Cond. Res. 34, 2886–2894 (2020).
Gómez-Carmona, P., Fernández-Cuevas, I., Sillero-Quintana, M., Arnaiz-Lastras, J. & Navandar, A. Infrared thermography protocol on reducing the incidence of soccer injuries. J. Sport Rehabil. 29, 1222–1227 (2020).
Bosquet, L., Léger, L. & Legros, P. Blood lactate response to overtraining in male endurance athletes. Eur. J. Appl. Physiol. 84, 107–114 (2001).
Feijen, S., Tate, A., Kuppens, K., Barry, L. A. & Struyf, F. Monitoring the swimmer’s training load: A narrative review of monitoring strategies applied in research. Scand. J. Med. Sci. Sports 30, 2037–2043 (2020).
Foster, C. et al. A new approach to monitoring exercise training. J. Strength Cond. Res. 15, 109–115 (2001).
Halson, S. L. Monitoring training load to understand fatigue in athletes. Sports Med. 44, 139–147 (2014).
Ayalon, A., Inbar, O. & Bar-Or, O. Relationship among measurement of explosive strength and anaerobic power. Int. J. Sports Sci. 1, 572–575 (1974).
Dotan, R. & Bar-Or, O. Load optimization for the wingate anaerobic test. Eur. J. Appl. Physiol. Occup. Physiol. 51, 409–417 (1983).
Bar-Or, O. The wingate anaerobic test an update on methodology, reliability and validity. Sports Med. 4, 381–394 (1987).
Breda, F. L. et al. Complex networks analysis reinforces centrality hematological role on aerobic–anaerobic performances of the Brazilian Paralympic endurance team after altitude training. Sci. Rep. 12, 1148 (2022).
Marostegan, A. B. et al. Effects of different inspiratory muscle warm-up loads on mechanical, physiological and muscle oxygenation responses during high-intensity running and recovery. Sci. Rep. 12, 11223 (2022).
Maglischo, C. W., Maglischo, E. W., Sharp, R. L., Zier, D. J. & Katz, A. Tethered and nontethered crawl swimming, in ISBS - Conference Proceedings Archive (1984).
Papoti, M., Martins, L. E. B., Cunha, S. A., Zagatto, A. M. & Gobatto, C. A. Effects of taper on swimming force and swimmer performance after an experimental ten-week training program. J. Strength Cond. Res. 21, 538 (2007).
Gobatto, C. A., Gomes De Arau Araujo, G., Santhiago, V., Papo Papoti, M. & Manchado-Gobatto, F. B. Validation of non-exhaustive test to determine the aerobic capacity in swimming. J. Sports Med. Phys. Fitness 58, 407–413 (2018).
Papoti, M. et al. Tethered swimming for the evaluation and prescription of resistance training in young swimmers. Int. J. Sports Med. 38, 125–133 (2017).
Tomlin, D. L. & Wenger, H. A. The relationship between aerobic fitness and recovery from high intensity intermittent exercise. Sports Med. 31, 1–11 (2001).
Jackson, A. S. & Pollock, M. L. Generalized equations for predicting body density of men. Br. J. Nutr. 40, 497–504 (1978).
Jackson, A. S., Pollock, M. L. & Ward, A. Generalized equations for predicting body density of women. Med. Sci. Sports Exerc. 12, 175–182 (1980).
Ferrari, H. G. et al. Aerobic evaluation in elite slalom kayakers using a tethered canoe system: A new proposal. Int. J. Sports Physiol. Perform. 12, 864–871 (2017).
Burdon, J. G., Juniper, E. F., Killian, K. J., Hargreave, F. E. & Campbell, E. J. The perception of breathlessness in asthma. Am. Rev. Respir. Dis. 126, 825–828 (1982).
Crowley, E., Harrison, A. J. & Lyons, M. The impact of resistance training on swimming performance: A systematic review. Sports Med. 47, 2285–2307 (2017).
Campos, E. Z. et al. Anaerobic contribution determined in swimming distances: Relation with performance. Front. Physiol. 8, 755 (2017).
Dempsey, J. A. Respiratory determinants of exercise limitation: focus on phrenic afferents and the lung vasculature. Clin. Chest Med. 40, 331–342 (2019).
Harms, C. A., Wetter, T. J., St. Croix, C. M., Pegelow, D. F. & Dempsey, J. A. Effects of respiratory muscle work on exercise performance. J. Appl. Physiol. (1985) 89, 131–138 (2000).
Redline, S., Gottfried, S. B. & Altose, M. D. Effects of changes in inspiratory muscle strength on the sensation of respiratory force. J. Appl. Physiol. 70, 240–245 (1991).
Romer, L. M., Lovering, A. T., Haverkamp, H. C., Pegelow, D. F. & Dempsey, J. A. Effect of inspiratory muscle work on peripheral fatigue of locomotor muscles in healthy humans. J. Physiol. 571, 425–439 (2006).
Goosey-Tolfrey, V., Foden, E., Perret, C. & Degens, H. Effects of inspiratory muscle training on respiratory function and repetitive sprint performance in wheelchair basketball players. Br. J. Sports Med 44, 665–668 (2010).
Hillen, B., Pfirrmann, D., Nägele, M. & Simon, P. Infrared thermography in exercise physiology: the dawning of exercise radiomics. Sports Med. 50, 263–282 (2020).
Priego Quesada, J. I. et al. Effects of the cycling workload on core and local skin temperatures. Exp. Therm. Fluid Sci. 77, 91–99 (2016).
Jimenez-Perez, I., Gil-Calvo, M., Vardasca, R., Fernandes, R. J. & Vilas-Boas, J. P. Pre-exercise skin temperature evolution is not related with 100 m front crawl performance. J. Therm. Biol. 98, 102926 (2021).
Galbraith, A. & Willmott, A. Transition phase clothing strategies and their effect on body temperature and 100-m swimming performance. Eur. J. Sport Sci. 18, 182–189 (2018).
Manchado-Gobatto, F. B. et al. Complex network model reveals the impact of inspiratory muscle pre-activation on interactions among physiological responses and muscle oxygenation during running and passive recovery. Biology (Basel) 11, 963 (2022).
Hawkes, E. Z., Nowicky, A. V. & McConnell, A. K. Diaphragm and intercostal surface EMG and muscle performance after acute inspiratory muscle loading. Respir. Physiol. Neurobiol. 155, 213–219 (2007).
Lazovic-Popovic, B. et al. Superior lung capacity in swimmers: Some questions, more answers!. Pulmonology 22, 151–156 (2016).
Merola, P. K. et al. High load inspiratory muscle warm-up has no impact on Special Judo Fitness Test performance. Ido Mov. Cult. 19, 66–74 (2019).
Acknowledgements
The authors would like to thank the head coach for accepting the invitation, the swimmers for their voluntary participation and the research team for their cooperation in carrying out the study.
Funding
The authors would like to thank the São Paulo Research Foundation—FAPESP (2012/06355-2, 2018/05821-6, 2019/05115-7, 2019/20894-2, 2019/20930-9, 2020/11946-6), the National Council for Scientific and Technological Development—CNPq (308117/2018-2, 309832/2021-7, 409521/2021-3, 312781/2023, 406765/2023), FAEPEX—UNICAMP (2583/20), the Coordination for the Improvement of Higher Education Personnel—CAPES (Finance Code 001) for their financial support. We also wish to thank the participants of our study.
Author information
Authors and Affiliations
Contributions
L.S.A., C.A.G. and F.B.M.-G. contributed to the proposition of ideas and research design. L.S.A., A.B.M., P.P.M.S. and J.B.O. conducted the experiments. L.S.A. performed to data analysis, wrote the main text of the manuscript, and created figures and tables. L.S.A., A.B.M., P.P.M.S., C.C., J.B.O., M.P., C.A.G. and F.B.M.-G. were responsible for data interpretation, data analysis review and discussion of results. C.A.G. and F.B.M.-G. obtained the financial support. All authors have read and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors below declare that they have no conflicts of interest that are relevant to the content of this article. The authors also certify that they have no affiliations with or involvement in any organization or entity with any financial or non-financial interest in the subject matter or materials discussed in this manuscript.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Soares de Araujo, L., Marostegan, A.B., Menezes Scariot, P.P. et al. Inspiratory muscles pre-activation in young swimmers submitted to a tethered swimming test: effects on mechanical, physiological, and skin temperature parameters. Sci Rep 14, 5975 (2024). https://doi.org/10.1038/s41598-024-52312-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-52312-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
