
Abstract
The aim of this study was to determine inter-instrument reliability between Takei and Jamar dynamometers in school children. Fifty-six five grade participants aged eleven to twelve (n = 32 boys, n = 24 girls) performed handgrip strength test on two different occasions, with a 5-day gap between them, as test–retest. The Pearson correlation coefficient showed very large to almost perfect correlation between both devices (r = 0.76–0.91) which was graphically confirmed by Bland–Altman method. Test–retest also showed high reliability (ICC = 0.78–0.85) for Jamar and Takei. Trivial, nonsignificant differences (p > 0.05) were observed between for test–retest trials for Takei left hand (ES = 0.04), right hand (ES = 0.12) and Jamar left hand (ES = 0.15). According to the results, both the Jamar and Takei dynamometers are valid and reliable for measuring schoolchildren, and both devices may be used to assess a student's handgrip strength for this age group.
Similar content being viewed by others

Introduction
Strength training has been shown to be a secure and efficient way to condition children, as long as the right exercise standards are followed1. Yet, reports show increases in some components of muscular fitness, but there are studies in children that shows declines in handgrip strength2,3. Low muscle strength is independently associated with a poorer metabolic profile during adolescence and with disease and all-cause mortality in adulthood4. Quantitative muscle strength measurement is indispensable in the evaluation of subjects, due to the monitoring of children's development5. Maximum voluntary handgrip strength (HGS) can assist researchers in identifying kids and teenagers at risk for serious public health issues such an increased chance of developing cardiovascular illnesses and poorer skeletal health in the future6. Considering the low levels of strength observed in children globally and the future health problems that may be developed consequently, HGS seems to be especially important to start measuring in children to track their trajectory as they develop6,7.
Two of the most discussed dynamometers within the current literature are the Jamar and the Takei8. The Takei dynamometer is characterized as a digital dynamometer, yet Jamar dynamometer is found to be a hydraulic tool9,10. The Jamar dynamometer is comprised of an adjustable anatomical rigid handle, hydraulic system, and analog display, which is regarded as the gold standard and frequently used as a benchmark in validity-reliability research, has a high test–retest reliability11. In grip strength, measurements conducted in the extended and 90° flexed positions of the elbow joint while standing, grip strength in elbow extension was found to be significantly higher than in elbow flexion11. Studies showed that Jamar hand dynamometer can be used in measuring children aged ten to twelve years12,13. Study carried out by Wołkow14 has demonstrated that children and adolescents have three distinct sensitive phases of the development of their motor abilities: between the ages of 8 and 9 years, 10 to 12 years, and 13 to 14 years. The research findings support this assertion by giving conflicting findings. A more balanced growth without abrupt accelerations or leaps was found to be a significant characteristic in the development of young judokas' motor abilities15,16. However, another research17 noticed an unusual trend in the rate of improvement in some motor abilities that was not seen in strength measures. After peaking between the ages of 11 and 12, the pace of development declines with age. The reliability of a Jamar dynamometer and the Martin Vigorimeter was compared for the measurement of grip strength in children12. As expected, smaller children needed a wider grip to use the Jamar dynamometer, but both can be used to measure children under twelve years old.
Similar to the Jamar, the Takei has also been found to be a valid and reliable tool to measure power grip. It uses an adjustable rectified and complacent handle shape, electromechanical system and a digital or analog display8. Several studies confirmed that Takei can be used to measure handgrip strength in children aged ten to fifteen years old18,19,20. We can see that Takei dynamometer is more used in measuring children, where Takei is used in a study involving 2125 children and adolescents21. Also, the preschool children aged 2–5 years old were tested with different dynamometers and observed that the Takei was the most reliable among the dynamometers, in addition, the Takei dynamometer showed the best validity22.
Considering previous studies, both dynamometers, Jamar and Takei, have shown validity and reliability in the child population8,11. Takei has already proven to be a valid instrument for measuring HGS in children and adolescents18,19,20. Also, Takei was constantly mentioned as the best, the most valid and most used, so it was necessary to check and compare the two dynanometers at school age. Considering the fact that Jamar is proven as the gold standard11, it is good to determine the inter-instrument reliability differences between these two devices and thereby confirm the fact about the validity of the device. Also, it is important to determine the validity of both devices, since it has already been confirmed that the Takei is easier to use on a child sample 8, since a smaller grip width is required, which can be a disturbing biological factor in testing children. For this reason, it is necessary to compare these two devices on a sample of school children aged 11–12 years. Although there is already research on this topic, this represents evidence-based data of the importance of using both dynometers Therefore, the aim of this study was to to examine inter-instrument reliability between Takei and Jamar dynamometers.
Methods
Participants
Fifty-six children (24 girls) aged from 11 to 13 years old (12.2 ± 0.4), from elementary school in Zagreb were tested (Table 1). Before testing, all participants were familiarized with the protocol and gave voluntary consent to participate in the study. Inclusion criteria considered healthy children that were attending school. For exclusion criteria kids that had current or recent injuries on their hands or previous hand surgery, that complaints of weakness or pain, were not included in this study. Prior to testing, written informed consent was obtained from the parents for each child. Additionally, children were asked if they participate in sports, if yes, in which sport, for how long and how many practices do they have weekly. This study was approved by the Committee on Ethics of Scientific Research at the Faculty of Kinesiology in Zagreb. We confirm that all methods were performed in accordance with the relevant guidelines and regulations of the Declaration of Helsinki. The study is part of the institutional project: The influence of wrestling training on selected tests of motor skills and body composition in Croatian wrestlers (reference number: 8835/2022).
Testing procedures
The measurements were conducted during a physical education class in the school hall, at an ideal temperature. Both measurements occurred around 1 p.m. The tests were conducted on two separate occasions, with a 5-day gap between them, and all the equipment, preparations, administration time, and processing methods remained consistent for both measurements. While searching the literature, we were unable to identify any material suggesting that there was a gold standard for the period between two handgrip strength tests. The information on the period between two testing sessions (test–retest) varied among the examined studies11,23,24,25. In line with studies that used a similar design and lasted a week, and due to the fact that school suggested the most suitable time for retest, we have chosen to have a 5-day period between testing sessions. Prior to the testing, a 5 min warm-up was provided, and the tests were demonstrated to the children. Following the protocol described below, the participants were given an opportunity to practice the tests. The handgrip test scores were recorded by a researcher who had extensive experience in conducting and evaluating physical fitness tests.
Each child was given a brief demonstration and verbal instructions for the handgrip test using the Takei handgrip dynamometer (Takei Scientific Instruments Co. Ltd, Tokyo, Japan), which, if necessary was adjusted according to the child’s hand size. The participants stood with their arms by their sides and their elbows fully extended during this. Two times of alternate measurements were made without a break. The participant was instructed to squeeze the dynamometer for 3 s for each measurement8. The peak value of strength was recorded, and the better result was used in the analysis.
The Jamar dynamometer (Paterson Medical, Green Bay, WI, USA) was placed in the right and left hand and was held loosely around the readout dial by the examiner to prevent dropping26. Two maximum contractions were taken for each hand. The better result of each hand was used for analysis. All participants were examined in the sitting position27.
Statistical data processing
The central tendency and variability of the data were represented using means and standard deviations (SD), along with 90% confidence interval limits (90% CI). The normality of the data was assessed using the Shapiro–Wilk test. Paired sample t-tests were conducted to determine if there was a significant difference between the Jamar and Takei test–retest measurements for both hands. Standardized differences in means were calculated to assess the magnitude of the change within and between the tests. The effect size (ES) magnitudes of change were categorized as trivial (> 0.2), small (0.2–0.5), moderate (0.5–0.8), large (0.8–1.60), and very large (> 1.60)28. The reliability of the mean change between trials was evaluated using the intraclass correlation coefficient (ICC), typical error (TE) and coefficient of variation (CV%). ICC values of 0.1, 0.3, 0.5, 0.7, 0.9, and 1.0 were classified as low, moderate, high, very high, nearly perfect, and perfect, respectively. Good reliability was defined as a CV < 5% and ICC > 0.6929. The degree of association between Jamar and Takei measurements was assessed using Pearson's product-moment correlation (r). Correlation values were interpreted as indicating small (r = 0.1–0.3), moderate (r = 0.3–0.5), large (r = 0.5–0.7), very large (r = 0.7–0.9), and almost perfect (r = 0.9–1.0) associations between variables and tests. Statistical significance was indicated in cases where p-value was less than 0.05. Additionally, the agreement between Jamar and Takei dynamometers data was then examined graphically using Bland and Altman’s plots in which the difference between both devices was plotted against the mean of the two devices30.
Results
Reliability
Test–retest reliability statistics for outcomes measures attained from Jamar and Takei both left and right hands are displayed in Table 2. Trivial, nonsignificant differences (p > 0.05) between the test–retest trials for Takei left hand (ES = 0.04), right hand (ES = 0.12) and Jamar left hand (ES = 0.15) were observed. Jamar right hand showed small differences (ES = 0.24). Furthermore, Jamar left hand (CV = 1.07%, ICC = 0.79), right hand (CV = 1.07%, ICC = 0.85) possessed good reliability ratings across test–retest trials. Takei left hand (CV = 0.98%, ICC = 0.78), right hand (CV = 0.99%, ICC = 0.83) also showed good reliability ratings across test–retest trials. Absolute reliability (CV) was considered as acceptable.
Pearson correlation
The mean ± SD for each outcome measure taken from Jamar and Takei left and right hand is shown in Table 3. Pearson correlation coefficients demonstrating the criterion validity between the Jamar and Takei were very large to almost perfect for right hand T1 (r = 0.84), right hand T2 (r = 0.91), and left hand T1 (r = 0.76), left hand T2 (r = 0.84) (Table 2). Differences between outcome measures observed in left hand T1, right hand T1 and right hand T2 were trivial (from 1.5 to 4.25%; ES = from 0.06 to 0.16) while small effect size was found in left hand T2 (5.40%; ES = 0.22).
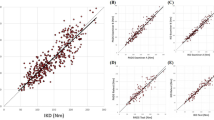
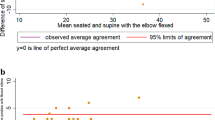
The Bland–Altman method
The Bland–Altman method graphically showed the reliability patterns, and confirmed the results obtained from intraclass correlation in terms of systematic error (bias or mean intertrial differences) and random error (95% limits of agreement). This method also showed differences between the mean of test–retest of both hands grip strength using Jamar and Takei devices. Mean differences and most data points were within the limits of agreement (Figs. 1 and 2).

Bland–Altman plots of the handgrip strength test, for the left and right hand using Takei and Jamar dynamometer. The central line characterizes the mean difference between test and retest values (systematic bias); the upper and lower lines characterize the upper and lower 95% limits of agreement.

Bland–Altman plots of the handgrip strength test, between Takei and Jamar dynamometer for left and right hand on test (T1) and retest (T2). The central line characterizes the mean difference between test and retest values (systematic bias); the upper and lower lines characterize the upper and lower 95% limits of agreement.
Discussion
This study aimed to examine reliability of Jamar and Takei dynamometers in school children. The authors pointed out that younger and middle school age groups can demonstrate the best rate of development of motor abilities31. For this reason, they advise differentiating training at that specific time period in order to develop specific talents thoroughly while adhering to the basic requirements of the organism. The rate of biological growth has a major role in determining sensitive times. This makes it even more crucial to differentiate training methods appropriately14. Motor abilities, which have developed as a whole biological system with several subsystems as a result of the training, have significant interactions with one another. This kind of development is typical of the ontogenesis's pre-pubescence stage. The structure of motor abilities (namely, strength) changes significantly at the age of 12 years which makes it unique17. The main findings revealed that both dynamometers showed non-significant differences between test–retest trials performed with left and right hand. In addition, Jamar and Takei for both hands possessed good reliability ratings across test–retest trials. Absolute reliability was considered as acceptable. Pearson correlation coefficients demonstrated very large to almost perfect correlation between the Jamar and Takei dynamometers.
The results of our study (ICC = 0.79–0.85) are consistent with earlier research12 that found that handgrip strength in school children had strong test–retest reliability (ICC = 0.92–0.96) utilizing various hand dynamometer kinds and testing procedures. Our findings also collaborate with previous research32 where test–retest reliability was high for both preferred (ICC = 0.94–0.98) and non-preferred (ICC = 0.96–0.98). In accordance to obtained results are results of other study33 where intraclass correlation coefficient (ICC) showed correlation of 0.76–0.94. The present results showed high test–retest reliability values (ICC = 0.79–0.85) and the absence of significant differences between test and retest suggest that the familiarization process was sufficient to give the young athletes confidence in using the hand dynamometer and the isometric evaluation. Good to excellent test–retest reliability was shown for handgrip in school children (ICC = 0.90 and ICC = 0.94)34. In contrast to our study, Clerke et al.35 observed that adolescents (13–17 years old) had small but significant differences (p ≤ 0.05) in handgrip strength between tests. This divergence in results can be seen as of consequence of maturation and due to natural biological growth and increases in hand size. The Jamar and Takei dynamometers were shown to be valid by Pearson correlation coefficients, which ranged from very high to almost perfect correlation (r = 0.76–0.91) for left as well as right hand. The similar magnitude of correlation was observed in our study and other research11. This study showed very strong positive correlation between two dynamometers (r = 0.91–0.94). In contrast to our results are results from study36 which demonstrated very weak correlation (r = 0.07–0.08) using Pearson correlation coefficient.
The reliability of the handgrip strength assessment may be impacted by several variables, including the type of dynamometer (Jamar vs. Takei), the body posture (standing vs. seated), and the position of the elbow joint. The Jamar and Takei hand dynamometer were applied in this study to assess handgrip strength. Preschoolers were evaluated between the ages of two and five, using various dynamometers as part of their study, and they found that the Takei dynamometer had the highest reliability and validity22. Jamar dynamometer, which has been consider as the gold standard for measuring grip strength in both adults and children, is a commonly used tool36. Higher reliability of maximum handgrip strength may potentially result from different elbow position or body posture. In study32, it was concluded that sitting position, with elbow position at 90° is the most frequently testing protocol for the assessment of grip strength.
Moreover, our results indicated that Jamar and Takei dynamometers are both valid and reliable in measuring school children and that both devices can be included in the testing of student’s handgrip for this age group. There are some limitations and issues connected to our study. Results are limited to school children. It is uncertain whether these findings can be applied to different age groups or individuals with different levels of physical activity. The age of 11 marks a crucial phase in a child's development, characterized by significant biological changes and the onset of puberty. Therefore, physical activity becomes highly significant17. As a limitation is also that we excluded parameters that can affect the results, such as body mass (BM), body mass index (BMI) and fat-free mass (FFT), as potential predictors of changes in handgrip strength between two measurements (Supplementary File 1).
Conclusion
Based on the results of present study, it can be concluded that Takai and Jamar dynamometers possessed good reliability ratings across test–retest trials, for both left and right hand in school children. Furthermore, these dynamometers were proved to be valid for assessment of handgrip strength. In order to measure handgrip strength in school children with normal development and who are not athletes, sports and health professionals can use this type of dynamometer as a reliable and valid measurement tool.
Data availability
All data generated or analysed during this study are included in this published article (and its supplementary information file).
References
Faigenbaum, A. D., Milliken, L. A. & Westcott, W. L. Maximal strength testing in healthy children. J. Strength Cond. Res. 17(1), 162–166 (2003).
Tremblay, M. S. et al. Fitness of Canadian children and youth: Results from the 2007–2009 Canadian health measures survey. Health Rep. 21(1), 7 (2010).
Moliner-Urdiales, D. et al. Secular trends in health-related physical fitness in Spanish adolescents: The AVENA and HELENA studies. J. Sci. Med. Sport 13(6), 584–588 (2010).
Cohen, D. et al. Ten-year secular changes in muscular fitness in English children. Acta Paediatr. 100(10), e175–e177. https://doi.org/10.1111/j.1651-2227.2011.02318.x (2011).
Ozaki, H. et al. The measurement of strength in children: Is the peak value truly maximal?. Children 8(1), 9. https://doi.org/10.3390/children8010009 (2020).
Abe, A., Yamasaki, S., Tahara, R., Loenneke, J. P. & Abe, T. Comparison of handgrip strength values in young children when using two different types of dynamometers. Am. J. Hum. Biol. 34(9), e23771. https://doi.org/10.1002/ajhb.23771 (2022).
Bull, F. C. et al. World Health Organization 2020 guidelines on physical activity and sedentary behavior. Br. J. Sports Med. 54, 1451–1462. https://doi.org/10.1136/bjsports-2020-102955 (2020).
Gatt, I., Smith-Moore, S., Steggles, C. & Loosemore, M. The Takei handheld dynamometer: An effective clinical outcome measure tool for hand and wrist function in boxing. Hand (New York, N.Y.) 13(3), 319–324. https://doi.org/10.1177/1558944717707831 (2018).
Güçlüöver, A. et al. Determination the validity of the new developed sport experts® hand grip dynamometer, measuring continuity of force, and comparison with current Takei and baseline® dynamometers. J. Sports Med. Phys. Fit. 55, 1318–1321 (2015).
Innes, E. V. Handgrip strength testing: A review of the literature. Aust. Occup. Ther. J. 46(3), 120–140 (1999).
Uysal, S. C., Tonak, H. A. & Kitis, A. Validity, reliability and test-retest study of Grip strength measurement in two positions with two dynamometers: Jamar® plus and K-force® grip. Hand Surg. Rehabil. 41(3), 305–310. https://doi.org/10.1016/j.hansur.2022.02.007 (2022).
Zuidam, J. M., Selles, R. W., Stam, H. J. & Hovius, S. E. Age-specific reliability of two grip-strength dynamometers when used by children. JBJS 90(5), 1053–1059. https://doi.org/10.2106/JBJS.G.00469 (2008).
Sherriff, A. et al. Age-and sex-standardised lean and fat indices derived from bioelectrical impedance analysis for ages 7–11 years: Functional associations with cardio-respiratory fitness and grip strength. Br. J. Nutr. 101(12), 1753–1760. https://doi.org/10.1017/S0007114508135814 (2008).
Wołkow, L. W. Sportiwnaja Podgotowka Dietiej i Podrostkow (Wieża, 1998).
Jagiello, W., Kalina, R. M. & Tkachuk, W. Age peculiarities of speed and endurance development in young judo athletes. Biol. Sport 18(4), 281–295 (2001).
Jagiełlo, W. & Kalina, R. M. Properties of motor development in young judokas. J. Hum. Kinet. 17, 113–120 (2007).
Jagiełło, W., Kalina, R. M. & Tkaczuk, W. Development of strength abilities in children and youths. Biol. Sport 21(4), 351–368 (2004).
Cohen, D. D. et al. Handgrip strength in English schoolchildren. Acta Paediatr. 99(7), 1065–1072. https://doi.org/10.1111/j.1651-2227.2010.01723.x (2010).
Stevenson, D. A. et al. Peripheral muscle weakness in RASopathies. Muscle Nerve 46(3), 394–399. https://doi.org/10.1002/mus.23324 (2012).
de Souza, M. A., Benedicto, M. M. B., Pizzato, T. M. & Mattiello-Sverzut, A. C. Normative data for hand grip strength in healthy children measured with a bulb dynamometer: A cross-sectional study. Physiotherapy 100(4), 313–318. https://doi.org/10.1016/j.physio.2013.11.004 (2014).
Serrano, M. M. et al. Dinamometría en niños y jóvenes de entre 6 y 18 años: valores de referencia, asociación con tamaño y composición corporal. An. Pediatr. 70(4), 340–348 (2009).
Ortega, F. B. et al. Systematic review and proposal of a field-based physical fitness-test battery in preschool children: The PREFIT battery. Sports Med. 45, 533–555. https://doi.org/10.1007/s40279-014-0281-8 (2015).
Hogrel, J. Y. Grip strength measured by high precision dynamometry in healthy subjects from 5 to 80 years. BMC Musculoskelet. Disord. 16(1), 1–12 (2015).
Svensson, E., Waling, K. & Häger-Ross, C. Grip strength in children: Test–retest reliability using Grippit. Acta Paediatr. 97(9), 1226–1231 (2008).
Gąsior, J. S. et al. Test-retest reliability of handgrip strength measurement in children and preadolescents. Int. J. Environ. Res. Public Health 17(21), 8026. https://doi.org/10.3390/ijerph17218026 (2020).
Mathiowetz, V., Weber, K., Volland, G. & Kashman, N. Reliability and validity of grip and pinch strength evaluations. J. Hand Surg. 9(2), 222–226. https://doi.org/10.1016/S0363-5023(84)80146-X (1984).
American Society of Hand Therapists. Clinical Assessment Recommendations 2nd edn. (American Society of Hand Therapists, 1992).
Hopkins, W. G., Schabort, E. J. & Hawley, J. A. Reliability of power in physical performance tests. Sports Med. 31, 211–234 (2001).
Buchheit, M., Lefebvre, B., Laursen, P. B. & Ahmaidi, S. Reliability, usefulness, and validity of the 30–15 intermittent ice test in young elite ice hockey players. J. Strength Cond. Res. 25(5), 1457–1464. https://doi.org/10.1519/JSC.0b013e3181d686b7 (2011).
Bland, J. M. & Altman, D. Statistical methods for assessing agreement between two methods of clinical measurement. The Lancet 327(8476), 307–310. https://doi.org/10.1016/S0140-6736(86)90837-8 (1986).
Jaskólski, E., Jagiełło, W. & Volkov, L. Biologiczne i Pedagogiczne Podstawy Systemu Szkolenia Sportowego (COS, 2005).
Gerodimos, V. Reliability of handgrip strength test in basketball players. J. Hum. Kinet. 31, 25. https://doi.org/10.2478/v10078-012-0003-y (2012).
Gerodimos, V. & Karatrantou, K. Reliability of maximal handgrip strength test in pre-pubertal and pubertal wrestlers. Pediatr. Exerc. Sci. 25(2), 308–322. https://doi.org/10.1123/pes.25.2.308 (2013).
Thams, L., Hvid, L. G., Damsgaard, C. T. & Hansen, M. Test-retest reliability of muscle strength and physical function tests in 6–9-year-old children. Meas. Phys. Educ. Exerc. Sci. 25(4), 379–387 (2021).
Clerke, A. M., Clerke, J. P. & Adams, R. D. Effects of hand shape on maximal isometric grip strength and its reliability in teenagers. J. Hand Ther. 18(1), 19–29. https://doi.org/10.1197/j.jht.2004.10.007 (2005).
Roberts, H. C. et al. A review of the measurements of grip strength in clinical and epidemiological studies: Towards a standardises approach. Age Ageing 40(4), 423–429. https://doi.org/10.1093/ageing/afr051 (2011).
Funding
This study received no external funding.
Author information
Authors and Affiliations
Contributions
Conceptualization, N.T. and G.K.; methodology, D.R. and T.I.; software, D.R.; validation, N.T. and D.P.; formal analysis, R.H. and T.I.; investigation, R.H.; resources, D.P.; data curation, T.I.; writing—original draft preparation, T.I. and D.R.; writing—review and editing, R.H. and G.K.; visualization, D.R.; supervision, N.T., D.P. and G.K.; project administration, R.H. and D.P.. All authors have read and agreed to the published version of the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Trajković, N., Rančić, D., Ilić, T. et al. Measuring handgrip strength in school children: inter-instrument reliability between Takei and Jamar. Sci Rep 14, 1074 (2024). https://doi.org/10.1038/s41598-024-51368-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-51368-1
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
