
Abstract
The purpose of this research is to examine the correlation between blood urea nitrogen (BUN) and severe abdominal aortic calcification (AAC) among American adults aged 40 years and older. A total of 2757 participants in the NHANES from 2013 to 2014 were included in the final analysis. BUN was measured by means of the enzymatic conductivity rate method. AAC scores were quantified by the Kauppila scoring system, and severe AAC was defined as an AAC score ≥ 6. Multivariable logistic regression and restricted cubic splines were used in the analyses. In the multivariable logistic regression model, the highest BUN level (log 2-transformed) was associated with an increased risk of severe AAC [odds ratio (OR) = 1.77, 95% CI 1.17, 2.71]. The restricted cubic spline plot displayed a reverse l-shaped association between BUN (log2-transformed) and severe AAC (p for nonlinearity < 0.001). In addition,the interactions of BUN were not discover. In general, there is a positive correlation between BUN and the risk of severe AAC.
Similar content being viewed by others
Introduction
Utilizing standard lateral lumbar radiographs to evaluate abdominal aortic calcification (AAC), it is identified as a marker for asymptomatic atherosclerotic conditions and functions as an independent forecaster for ensuing vascular diseases and mortalities1. According to previous study, atherosclerosis, a disease of the large arteries, is the primary cause of heart disease and stroke2,3. It is the fundamental reason for approximately half of all fatalities4. Nonetheless, there is presently no effective therapy for serious AAC. To assess personalized cardiovascular risk, recognizing atherosclerosis in its subclinical phase is crucial5.
Blood urea nitrogen (BUN) is a laboratory test that measures the amount of nitrogen in the blood that comes from urea, a waste product formed by the liver6. Elevated BUN levels are often seen in individuals with chronic kidney disease (CKD), which is frequently associated with cardiovascular disease (CVD)7,8. Numerous studies indicate that the BUN/creatinine ratio, which functions independently of both BUN and creatinine, is a well-established predictor of adverse outcomes in patients with CVD9,10. In addition, some research suggests that in Chinese communities, a higher BUN level may be linked to a higher risk of incident coronary artery disease(CAD)11. Moreover, most previous studies were investigated among patients with heart failure12, acute coronary syndrome13, or stroke14. However, no cross-sectional study has examined the relationship between BUN and severe AAC among a general population.
Hence, we carried out this research to examine the correlations between BUN and severe AAC, utilizing data from the National Health and Nutritional Examination Survey (NHANES) for the years 2013–2014.
Methods
Ethics statement
The studies involving human participants were ethically approved by The National Center for Health Statistics (NCHS) Ethics Review Board. Prior to data collection, all participants provided written informed consent. All methods were conducted in accordance with the relevant guidelines and regulations of the NCHS Institutional Review Board.
Study population
NHANES is a survey that employs a complex multistage probability sampling design and oversamples minority populations to ensure accurate representation of the US population. Individual participants are assigned appropriate sampling weights, and continuous NHANES data have been accessible since 1999, released every 2 years15.
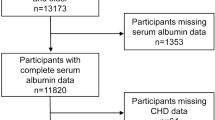
Our investigation of the potential correlation between BUN and severe AAC was grounded on data from the 2013–2014 NHANES cycle. This is because only this specific cycle contains information on both BUN and AAC scores. Furthermore, individuals under the age of 40 were not considered in our analysis because that AAC scores were determined through dual-energy X-ray absorptiometry (DXA) scans, which were not conducted on participants below this age during the relevant NHANES cycle in 2013–2014. Our analysis was limited to individuals aged 40 years or older who had complete data on both blood urea nitrogen and abdominal aortic calcification (AAC) scores. Initially, a total of 10,175 participants were included in the study. However, after excluding individuals under the age of 40 (n = 6360), those with incomplete BUN data (n = 288), missing AAC scores (n = 509), or incomplete data on other covariates (n = 247) and estimated glomerular filtration rate (eGFR) < 15 ml/min/1.73 m2 (n = 14), such as demographics and blood biochemical indexes, the final sample size for analysis was reduced to 2757 participants (Fig. 1).

Flowchart of participants included in the analysis.
The protocol for NHANES received clearance and endorsement from the National Center for Health Statistics’ Ethics Review Board. All participants provided written informed consent before any data collection commenced.
Exposure and outcome definitions
The AAC score was determined by evaluating lateral lumbar spine images acquired from DXA (Densitometer Discovery A, Hologic, Marlborough, MA, USA), executed by trained NHANES affiliated personnel during a single assessment in a mobile examination center (MEC). Utilizing the Kauppila scoring method, which has been extensively cited and employed for evaluating calcified vessel severity, professional technologists assigned a total AAC score for each participant with scores ranging from 0 to 2416. Previous research has also identified severe AAC as an important outcome measure, defined by a total AAC score ≥ 6, indicating the presence of significant aortic calcification lesions1,17.
Blood urea nitrogen samples should to be procured from non-hemolyzed specimens, and there is no need for fasting. If samples are stored beyond 24 h, they should be preserved at temperatures between − 15 °C and − 20 °C, with only one thawing instance permitted. Inadequate samples may consist of insufficient volume (< 0.6 mL), hemolysis, incorrect labeling, or extended exposure of serum or plasma to cells.
Covariates
A standardized survey was utilized to gather demographic data, encompassing respondents’ age (< 60 and ≥ 60), race (Mexican American, Other Hispanic, non-Hispanic White, non-Hispanic Black, and other), educational level (Less Than 9th Grade, 9–11th Grade, High School Grad/GED, Some College or AA degree, and College Graduate or above), body mass index (BMI),alcohol use (drinker, nondrinker),smoking status (yes/no), alanine aminotransferase (ALT), aspartate aminotransferase (AST), serum vitamin B12, eGFR, hypertension(yes/no), diabetes status(yes/no) and income-to-poverty ratio (PIR). Individuals who reported consuming a minimum of 12 alcoholic beverages in any given year were categorized as drinkers. Individuals who had consumed a minimum of 100 cigarettes throughout their lives were categorized as smokers. The criteria for diabetes encompassed the use of hypoglycemic medications or a medical diagnosis, in addition to satisfying specific laboratory benchmarks, such as a hemoglobin A1c concentration of ≥ 6.5% and/or a fasting plasma glucose concentration of ≥ 126 mg/dL18. The definition of hypertension included taking medications for high blood pressure, having a medical diagnosis of hypertension, or having average systolic blood pressure readings greater than or equal to 140 mmHg, and/or diastolic blood pressure readings greater than or equal to 90 mmHg19. Using BMI cutoff points, subjects were divided into three groups: underweight (< 18.5 kg/m2), normal weight (18.5–25 kg/m2), over weight (25–30 kg/m2), and obesity (≥ 30 kg/m2). The chronic kidney disease epidemiology collaboration creatinine equation20 was used to determine the eGFR. The measurement methodologies for the research variables are fully described on the publically available website: www.cdc.gov/nchs/nhanes/.
Statistical analysis
In light of the intricate, multistage, probability sampling approach used in the NHANES survey, oversampling occurred for representative participants of specific civilian, noninstitutionalized US subpopulations. Consequently, we incorporated sample weights that had been established in the NHANES analysis. To generate unbiased national estimates, the study utilized the sample weight.
The categorical data were described by frequency (n) and percentage (%), and continuous data were described by the mean ± standard deviation (SD). BUN was skewed distributed and log 2-transformed to improve the normality of the data. We divided the BUN(log 2-transformed) concentration into four categories and study participants were categorized, based on quartiles of BUN. In relation to BUN quartiles, general attributes were compared utilizing the Wilcoxon rank-sum test for continuous variables, and the chi-square test for categorical variables. Three separate multivariate logistic regression models were applied to examine the independent connection between BUN and severe AAC. Model 1 was the unadjusted version. Model 2 incorporated age, sex, and ethnicity. Model 3 extended upon Model 2 by adding body mass index (BMI), education level, alcohol consumption, smoking status, diabetes, ALT, AST, serum vitamin B12, PIR, eGFR and hypertension as additional variables. Subgroup analysis categorized by age, gender, hypertension, smoking status, and diabetes, was conducted using stratified multivariate regression analysis. Additionally, an interaction term was introduced to examine the heterogeneity in the associations among the subgroups. The nonlinear association between BUN and severe AAC was analyzed using restricted cubic splines (RCS) to address potential nonlinearities.
All analyses were conducted using table one and the foreign package from R (version 4.2.2) and GraphPad Prism (version 9.0.0). Statistical significance was determined by two-sided p values of less than 0.05.
Results
Baseline characteristics of the enrolled participants
The essential traits of the research participants are displayed in Table 1. Of the participants, 303 (9.6%) had severe AAC. Participants with severe AAC were older, more likely to be female, white, and smokers than those without the condition. In addition, there was a greater frequency of diabetes, hypertension, elevated serum vitamin B12 levels, elevated BUN, and decreased eGFR in these individuals.
Association of blood urea nitrogen with severe abdominal aortic calcification
We used three logistic regression models to show the relationship between BUN and severe AAC in Table 2: The BUN index was categorized based on quartiles, and when comparing participants in the lowest quartile to those in the highest quartile, higher odds for extensive AAC were found across all three models (Model 1: OR = 3.54, 95% CI 2.53–5.03; Model 2: OR = 1.92, 95% CI 1.33–2.82; Model 3: OR = 1.77, 95% CI 1.17–2.71; all p-value < 0.05).In the fully adjusted model (model 3), we found that compared with the first quartile (Q1),the prevalence of severe AAC in the highest quartile group (Q4) increased by 77%.
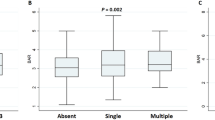
As shown in Fig. 2, the restricted cubic spline plot displayed a reverse l-shaped association between blood urea nitrogen (log 2-transformed) and severe AAC (p for nonlinearity < 0.001). We further conducted a threshold effect analysis of the association between BUN (log 2-transformed) and severe AAC (Table 3) after adjustment for multiple potential covariates. We fit the l-line logistic regression model and 2-piecewise logistic regression model to test the relationship between BUN and severe AAC. The results indicated that the 2-piecewise logistic regression model was superior to the l-line logistic regression model for fitting the association between blood urea nitrogen and severe AAC (p for the log likelihood ratio test < 0.05). We identified an inflection point of 3.79 mg/dl for log 2-transformed blood urea nitrogen. When blood urea nitrogen was > 3.79 mg/dl (Log2- transformed), each onefold increase in blood urea nitrogen was significantly associated with a 87% increase in the prevalence of severe AAC (OR 1.87, 95% CI 1.13, 3.09).

Association between BUN level and severe AAC. Adjusted for age group, sex, race, education level, PIR, BMI, alcohol use, smoking status, hypertension, diabetes, serum vitamin B12, ALT, eGFR and AST. The solid and shaded areas represent the odds ratios and corresponding 95% confidence intervals. OR odds ratio, AAC abdominal aortic calcification, BUN blood urea nitrogen, PIR poverty income ratio, BMI body mass index, ALT alanine aminotransferase, AST aspartate aminotransferase, eGFR estimated glomerular filtration rate.
Subgroup analyses
Subgroup analyses stratified by age, sex, smoking status, hypertension, and diabetes was subsequently performed and are illustrated in Fig. 3. We discovered that in all multivariate logistic regression models, the relationship between BUN and severe AAC in females remained statistically significant. No notable interactions have come to our attention (all P for interaction > 0.05).

Subgroup analysis for the association between BUN and severe AAC.
Discussion
Within a nationally representative US cohort, we identified an association between BUN levels and the risk of severe AAC. A notable positive relationship was found between overall BUN concentrations and severe AAC. In this study, the smooth fitting curve between BUN and severe AAC was reverse L-shaped and the inflection point was > 3.79 mg/dL (Log2- transformed).
There is substantial clinical significance to these findings. First, a subclinical characteristic of CVD is AAC. Our findings offer a fresh method for assessing the risk of severe AAC in the general population. We suggested that people with high BUN levels would benefit from regular cardiac health monitoring to lower their chance of developing CVD in the future. Second, when assessing the risk of CVD in middle-aged and older persons, particularly in females, BUN level should be included in addition to conventional CVD risk factors.
A prevalent functional indicator of renal function is blood urea nitrogen. A growing body of research indicates that BUN is a reasonably common routine test that can accurately identify high-risk individuals with acute coronary syndrome (ACS) so that any unfavorable vascular events are closely monitored20. Moreover, earlier research has shown that eGFR had little bearing on the relationships found between BUN level and coronary heart disease11 or other cardiovascular outcomes13. More significantly, logistic regression analysis demonstrated that, once the effects of other variables (such as age, gender, comorbidities, cardiac enzymes, etc.) on the outcome were eliminated, patients whose BUN levels were higher than our observed cut-off values were nearly 20 times more likely to suffer adverse cardiovascular events that resulted in mortality21,22,23. Prior research revealed that, after adjusting for eGFR levels, a higher BUN level was linked to a 17% increased risk of coronary heart disease11. Consistent with previous research, we discovered noteworthy correlations between elevated BUN and the likelihood of severe AAC, even after accounting for eGFR. These conclusions held true even after excluding individuals whose eGFR was less than 15 ml/min/1.73 m2. In order to confirm our results and determine the appropriate normal range of BUN for the prevention of AAC, bigger sample sizes will be needed in future research.
While BUN is acknowledged as a possible risk factor for cardiovascular disease, the specific mechanisms have yet to be fully understood. One plausible biological pathway that connects increased BUN levels and AAC could involve disruptions in glucose balance24,25. BUN not only indicates kidney performance but is also associated with the stimulation of neurohormones26. Increased BUN reabsorption may be the outcome of elevated vasopressin levels in patients with heart failure. It might be connected to atherosclerosis because oxidative stress damages the arterial wall and causes myocardial ischemia or infarction in the end27. In addition, the enhancement in urea reabsorption can be attributed to the stimulation of the sympathetic nervous system and the activation of the renin–angiotensin–aldosterone system which is known to have a connection with cardiovascular risk28.
Our investigation possesses numerous advantages. First, it utilizes data from NHANES, an extensive, countrywide, population-based sample gathered through a uniform methodology. Furthermore, we accounted for potential confounding factors, with the choice of these variables primarily derived from earlier research evaluating the association between AAC and other relevant exposures, thus ensuring the dependability of our findings.
Nonetheless, certain limitations must be acknowledged. Although we adjusted for some potential covariates, it was not possible to entirely eliminate the impact of other potential confounders, such as diuretics, hormones, and medication usage, which might affect calcification. Moreover, our sample solely consisted of participants from one country, making it less applicable to the global population with diverse ethnic backgrounds. Last, the subject reported disease history could be subject to recall errors.
Conclusions
In general, there is a positive correlation between BUN and the risk of severe AAC. In addition to traditional CVD risk factors, BUN level should be taken into consideration. Such findings require further prospective studies to provide more evidence.
Data availability
The datasets generated and analyzed during the current study are available in the National Health and Nutrition Examination Survey (NHANES), www.cdc.gov/nchs/nhanes/.
References
Wilson, P. W. et al. Abdominal aortic calcific deposits are an important predictor of vascular morbidity and mortality. Circulation 103, 1529 (2001).
Imaoka, Y. et al. Impact of abdominal aortic calcification among liver transplantation recipients. Liver Transplant. 25, 79 (2019).
van der Meer, I. M. et al. Predictive value of noninvasive measures of atherosclerosis for incident myocardial infarction: The Rotterdam study. Circulation 109, 1089 (2004).
Lusis, A. J. Atherosclerosis. Nature 407, 233 (2000).
Li, Y. W. & Chen, W. L. Clinical relevance of serum uric acid and abdominal aortic-calcification in a national survey. Clin. Cardiol. 43, 1194 (2020).
Peng, R. et al. Blood urea nitrogen, blood urea nitrogen to creatinine ratio and incident stroke: The Dongfeng-Tongji cohort. Atherosclerosis 333, 1 (2021).
Konishi, H. et al. Association of low glomerular filtration rate with the incidence of stroke in patients following complete coronary revascularization. Circ. J. 75, 2372 (2011).
Sarnak, M. J. et al. Kidney disease as a risk factor for development of cardiovascular disease: A statement from the American Heart Association Councils on kidney in cardiovascular disease, high blood pressure research, clinical cardiology, and epidemiology and prevention. Hypertension 42, 1050 (2003).
Matsue, Y. et al. Blood urea nitrogen-to-creatinine ratio in the general population and in patients with acute heart failure. Heart 103, 407 (2017).
Lin, H. J. et al. Elevated blood urea nitrogen-to-creatinine ratio increased the risk of hospitalization and all-cause death in patients with chronic heart failure. Clin. Res. Cardiol. 98, 487 (2009).
Jiang, H. et al. Associations of estimated glomerular filtration rate and blood urea nitrogen with incident coronary heart disease: the Dongfeng-Tongji Cohort Study. Sci. Rep. 7, 9987 (2017).
Aronson, D., Mittleman, M. A. & Burger, A. J. Elevated blood urea nitrogen level as a predictor of mortality in patients admitted for decompensated heart failure. Am. J. Med. 116, 466 (2004).
Kirtane, A. J. et al. Serum blood urea nitrogen as an independent marker of subsequent mortality among patients with acute coronary syndromes and normal to mildly reduced glomerular filtration rates. J. Am. Coll. Cardiol. 45, 1781 (2005).
You, S. et al. Prognostic significance of blood urea nitrogen in acute ischemic stroke. Circ. J. 82, 572 (2018).
Johnson, C. L. et al. National health and nutrition examination survey: Analytic guidelines, 1999–2010. Vital Health Stat. 2, 1 (2013).
Kauppila, L. I. et al. New indices to classify location, severity and progression of calcific lesions in the abdominal aorta: A 25-year follow-up study. Atherosclerosis 132, 245 (1997).
Lewis, J. R. et al. Long-term atherosclerotic vascular disease risk and prognosis in elderly women with abdominal aortic calcification on lateral spine images captured during bone density testing: A prospective study. J. Bone Miner. Res. 33, 1001 (2018).
Menke, A., Casagrande, S., Geiss, L. & Cowie, C. C. Prevalence of and trends in diabetes among adults in the United States, 1988–2012. JAMA 314, 1021 (2015).
Chobanian, A. V. et al. Seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension 42, 1206 (2003).
Levey, A. S. et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 150, 604 (2009).
Adam, A. M. et al. Efficacy of serum blood urea nitrogen, creatinine and electrolytes in the diagnosis and mortality risk assessment of patients with acute coronary syndrome. Indian Heart J. 70, 353 (2018).
Aono, T. et al. Normal ranges of blood urea nitrogen and serum creatinine levels in the community-dwelling elderly subjects aged 70 years or over–correlation between age and renal function. Nihon Ronen Igakkai Zasshi 31, 232 (1994).
Fehrman-Ekholm, I. & Skeppholm, L. Renal function in the elderly (>70 years old) measured by means of iohexol clearance, serum creatinine, serum urea and estimated clearance. Scand. J. Urol. Nephrol. 38, 73 (2004).
Koppe, L. et al. Urea impairs beta cell glycolysis and insulin secretion in chronic kidney disease. J. Clin. Investig. 126, 3598 (2016).
D’Apolito, M. et al. Urea-induced ROS generation causes insulin resistance in mice with chronic renal failure. J. Clin. Investig. 120, 203 (2010).
Liu, E. Q. & Zeng, C. L. Blood urea nitrogen and in-hospital mortality in critically ill patients with cardiogenic shock: Analysis of the MIMIC-III database. Biomed. Res. Int. 2021, 5948636 (2021).
Himmelfarb, J., Stenvinkel, P., Ikizler, T. A. & Hakim, R. M. The elephant in uremia: Oxidant stress as a unifying concept of cardiovascular disease in uremia. Kidney Int. 62, 1524 (2002).
Usberti, M. et al. Effects of angiotensin II on plasma ADH, prostaglandin synthesis, and water excretion in normal humans. Am. J. Physiol. 248, F254 (1985).
Acknowledgements
We express our gratitude to the data gathering group and the NHANES administrators for making relevant information accessible via the NHANES website.
Funding
This work was supported by the Shandong Province Traditional Chinese Medicine Science and Technology Project (Grant Nos.M-2022159).
Author information
Authors and Affiliations
Contributions
K.X. was involved in designing the study, collecting data, conducting statistical analysis, and creating the initial manuscript draft. S.S.X. critically reviewed the manuscript and offered valuable insights. All authors contributed to the article and approved the final version submitted for publication.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Xue, K., Xing, S. Blood urea nitrogen concentration is associated with severe abdominal aortic calcification in adults: a cross-sectional investigation. Sci Rep 13, 19834 (2023). https://doi.org/10.1038/s41598-023-47109-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-47109-5
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
