
Abstract
Hypertrophic cardiomyopathy (HCM) is one of the most common hereditary heart diseases and is associated with a high risk of sudden cardiac death. HCM is characterized by pronounced hypertrophy of cardiomyocytes, fiber disarray and development of fibrosis and can be divided into a non-obstructive (HNCM) and obstructive form (HOCM) therefore requiring personalized therapeutic therapies. In the present study, we investigated the expression patterns of several circulating circular RNAs (circRNAs) as potential biomarkers in patients with HCM. We included 64 patients with HCM and 53 healthy controls to the study and quantitatively measured the expression of a set of circRNAs already known to be associated with cardiac diseases (circDNAJC6) and/or being highly abundant in blood (circTMEM56 and circMBOAT2). Abundancy of circRNAs was then correlated to relevant clinical parameters. Serum expression levels of circRNAs DNAJC6, TMEM56 and MBOAT2 were downregulated in patients with HCM. The inverse association between circRNA levels and HCM remained unchanged even after adjusting for confounding factors. All circRNAs, evaluated separately or in combination, showed a robust discrimination capacity when comparing control subjects with HCM, HNCM or HOCM patients (AUC from 0.722 to 0.949). Two circRNAs, circTMEM56 and circDNAJC6, significantly negatively correlated with echocardiographic parameters for HOCM. Collectively, circulating circRNAs DNAJC6, TMEM56 and MBOAT2 can distinguish between healthy and HCM patients. In addition, circTMEM56 and circDNAJC6 could serve as indicators of disease severity in patients with HOCM. Thus, circRNAs emerge as novel biomarkers for HCM facilitating the clinical decision making in a personalized manner.
Similar content being viewed by others

Introduction
Hypertrophic cardiomyopathy (HCM) is one of the most commonly inherited cardiovascular diseases caused by mutations in genes encoding key cardiac sarcomeric proteins1. Its prevalence has been originally described with 1:500. Taking into account not only clinical manifestation but also pathogenic genetic mutations, the prevalence of HCM may increase up to 1:200, affecting as many as 20 million people worldwide recently estimated by epidemiological studies2,3. Only about 10 percent of patients are clinically identified, the remaining 90 percent display an unidentified cohort awaiting therapy1. HCM is characterized by myocardial hypertrophy and can be subdivided into (A) non-obstructive (HNCM) and (B) obstructive appearance (HOCM). Pathophysiologically, HCM is not only characterized by hypertrophy of cardiomyocytes, but also fiber disarray and progression of ventricular fibrosis. HOCM differs from HNCM clinically by the presence of a pathological increased gradient in the left ventricular outflow tract caused by the asymmetric septum hypertrophy. Such discrepancy also establishes alternative treatment regimen for these two forms of HCM. Of note, hypertrophic cardiomyopathy has various manifestations from asymptomatic status or mild clinical symptoms up to heart failure and sudden cardiac death4. Despite the given clinical relevance of HCM there is a lack of biomarkers that can simplify the clinical management of patients suffering from HCM.
Non-coding RNAs represent a potential class of disease-associated biomarkers investigating small non-coding RNAs such as microRNAs (miRNAs) and long non-coding RNAs (lncRNAs), respectively5. In the past, we and others provided evidence that miRNAs as well as lncRNAs are associated with HCM in blood and heart tissue6,7,8,9. In the world of RNA, circular RNAs (circRNAs) exhibit a subclass of non-coding RNAs resulting from back-splicing of exons. They are single stranded RNAs with a covalently closed circular structure and can be found nuclease-resistant in tissues as well as in fluids. The stability of circRNAs makes them ideal candidates for biomarker discovery. At the molecular level, circRNAs regulate gene expression at the transcriptional and posttranscriptional stage and are involved in multi-facetted biological processes, indeed contributing to several diseases10,11. Here, we identified circulating circRNAs as potential biomarkers for HCM consequently differentiating between patients with obstructive and non-obstructive hypertrophic cardiomyopathy as well as healthy subjects.
Results
The present study included 64 patients with hypertrophic cardiomyopathy and 53 healthy control individuals. Among HCM patients there were 33 patients without and 31 with obstruction in the left ventricular outflow tract highlighted in the detailed patient characteristics (Table 1). Patients were chosen according to the diagnostic criteria based on the recent European guidelines for the diagnosis and management of hypertrophic cardiomyopathies4. There was no difference in the NYHA classification, numbers of syncopes, arrhythmias, positive family history and co-morbidities between HOCM and HNCM patients. At the medication level, there was no difference for HOCM and HNCM patients for beta blockers, ACE inhibitors and diuretics, but the use of AT receptor antagonists was significantly higher in HNCM patients. Comparing echocardiographic acquisition, there were no differences between left ventricular end-diastolic dimensions, size of left atrium and the thickness of the left ventricular wall between HOCM and HNCM patients. However patients with HOCM showed a significantly higher gradient in the left ventricular outflow tract due to the pathophysiology of HOCM. The incidence of mitral regurgitation was different between HOCM and HNCM group, whereby there were more minor regurgitations in the HNCM group and more medium regurgitations in the HOCM group.
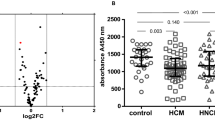
In line to previously published data we investigated the concentration of several circRNAs known to be abundant in peripheral blood12,13 and were able to detect 3 circRNAs (circDNAJC6, circMBOAT2 and circTMEM56) in serum via quantitative Real-time PCR (detailed information about circRNAs isoforms are given in Supplemental Table S1). The expression levels of circRNAs DNAJC6, MBOAT2 and TMEM56 were significantly higher in control subjects than in patients with HCM (Fig. 1A–C). The inverse association between circRNA levels and the presence of HCM remained unchanged even after adjusting for age and sex (Table 2). Analyzing both groups HOCM and HNCM revealed similar levels of the circRNA set (Fig. 1A–C). To further underline these results, we performed an additional ROC curve analysis indicating that all circRNAs, separately or in combination, demonstrated a strong discrimination value when comparing control subjects with HCM, HNCM or HOCM patients [area under the ROC curve (AUC) from 0.722 to 0.949] (Fig. 2A–C and Suppl. Fig. S2A–C). As expected, circRNAs showed a low AUC for the comparison between HOCM and HNCM (AUC from 0.532 to 0.583) (Suppl. Fig. S1A–C). Nonetheless, the discrimination for HNCM vs HOCM was improved when combining the three circRNAs (AUC = 0.650) (Suppl. Fig. S2D).

Expression levels of circular RNAs were measured in serum of patients in the study groups: (A) circDNAJC6; (B) circMBOAT2; (C) circTEM56. Differences between groups were analyzed using Kruskal–Wallis test and/or Mann–Whitney U test. Data represent the medians (IQR), minimum and maximum. P‐values describe the significance level of differences for each comparison. HCM: hypertrophic cardiomyopathy; HNCM: non-obstructive hypertrophic cardiomyopathy; HOCM: obstructive hypertrophic cardiomyopathy.

ROC curve analyses of circulating circular RNAs. (A) circDNAJC6; (B) circMBOAT2; (C) circTMEM56. Data are presented as the area under the ROC curve (AUC) and 95% confidence intervals (CI). HCM: hypertrophic cardiomyopathy; HNCM: non-obstructive hypertrophic cardiomyopathy; HOCM: obstructive hypertrophic cardiomyopathy.
We also performed correlation analyses to explore the potential association of HCM with different echocardiographic parameters that are the main characteristics for HOCM. As shown in Fig. 3, we observed a direct significant correlation between circRNAs circDNAJC6 and circTMEM56 and left ventricular outflow tract gradient (LVOT gr.max.) as well as thickness of interventicular septum (IVS) in this patient group. No correlations were observed between circRNAs and echocardiographic parameters in the whole HCM population or HNCM subgroup (data not shown). Taken together, the expression level of circRNAs is negatively correlated with LVOT gradient and IVS thickness in patients with HOCM indicating the severity of this obstructive cardiac disease and helping to improve early discovery.

Correlations between circulating circular RNAs and echocardiographic parameters in patients with obstructive hypertrophic cardiomyopathy (HOCM). (A) circDNAJC6 vs LVOT gr. Max.; (B) circTEME56 vs IVS. Correlations between variables were analyzed using Spearman’s rho coefficient. LVOT gr. Max.: maximum gradient in left ventricular outflow tract. IVS: interventricular septum.
Discussion
Herein, we quantitatively explored for the first time circulating circRNAs in patients with HCM. The major finding of our study is that abundancy of circulating circRNAs circTMEM56, circDNAJC6 and circMBOAT2 is significantly lower in patients with HCM than in healthy controls. Importantly, the three circRNAs show a good performance as biomarkers of HCM, as suggested by their discrimination value. In addition, the level of circRNAs circTMEM56 and circDNAJC6 is negatively correlated to the severity of left ventricular obstruction and thickness of interventricular septum in HOCM group. A separate classification between HNCM and HOCM can only be made by a combinatorial approach, as the individual circRNAs do not show a significant difference between these subgroups of HCM.
Noteworthy, circRNAs have emerged as an interesting class of biomarkers being highly conserved and resistant to cellular influences of RNAses14. Several global profiling studies identified and characterized multiple circRNAs in different tissues as well as in peripheral blood12,13,15. circRNAs can act on gene expression in different ways, e.g. functioning as miRNA-sponges or regulating transcription16,17,18. On the opposite, circRNAs can be regulated by RNA binding proteins like Rbm20 in dilated cardiomyopathy19 or Quaking in doxorubicin-induced cardiomyopathy20. There is growing evidence that circRNAs can be secreted from diseased tissue into the extracellular space via exosomes13,21. Iparraguirre et al. examined the role of circulating circRNAs in autoimmune diseases and reported that circRNA ANXA2 from peripheral blood can be used as a biomarker for multiple sclerosis12. Endogenous circRNAs are also implicated in cancer development and can serve as biomarkers. In non- small cell lung cancer a circRNA derived from exons of the FARSA gene and called circFARSA, was observed to be enriched in cancerous tissues. Next to that circFARSA was more abundant in patients’ plasma than controls, therefore demonstrating evidence of its role as a potential noninvasive biomarker for malignancy of non-small cell lung cancer11. Switching to the field of cardiovascular diseases, circRNA CDR1as is upregulated in hypoxic cardiomyocytes and in myocardial infarction in mice22. Another circRNA MICRA was shown to be less abundant in peripheral blood of patients with myocardial infarction and in line low levels of MICRA are associated with the higher risk of left ventricular dysfunction23,24. The circRNA molecule circFOXO3 is involved in doxorubicin-induced senescence and promotes cardiac senescence by modulating cytoprotective proteins in different cellular compartments25. Experimental evidence exists that circRNAs are also implicated in cardiac fibrosis, e.g. circRNA_000203 and circRNA_01056726,27 both leading to increased levels of pro-fibrotic proteins by sponging corresponding miRNAs. At the clinical stage focusing on dilated cardiomyopathy (DCM) mutations in RNA binding protein Rbm20 are associated with loss of circRNAs from titin gene and result in the development of dilative phenotype19. Siede et al. have recently shown that several circRNAs, e.g. circDNAJC6, can be dynamically expressed in dilated hearts and human induced pluripotent stem cell derived cardiomyocytes subjected to disease development and stress response28. In contrast, little is known about circRNAs in HCM. Following up the observation of decreased circDNAJC6 levels in bioptic material from patients with DCM28, we examined the expression level of this circRNA in serum of patients with HCM. Our data indicate that DNAJC6 expression was lower in HMC group compared to controls and negatively correlates with the maximum gradient in LVOT. We examined the correlation of more circRNAs with HCM characteristics determined via echocardiography. While there was no correlation in the HNCM group between circRNAs and echocardiographic parameters, circTMEM56 and circDNAJC6 significantly negatively correlated with echocardiographic parameters characteristic for HOCM (LVOT grad. max and IVS). Therefore, HOCM patients with the lowest circRNA expression level had significantly higher LVOT grad. max. and IVS. Thus, both circRNAs circTMEM56 and circDNAJC6 may serve as an indicator of disease severity in patients with HOCM. Further studies now should investigate the importance of the interaction between circRNAs and clinical severity of HOCM in order to facilitate therapeutic decisions, e.g. implantation of cardioverter/defibrillator (ICD) or myocardial reduction therapy (TASH or myectomy).
According to the current clinical guidelines genetic testing of patients is recommended as a class I indication in the presence of symptoms and signs of disease to confirm the diagnosis4. This may contribute to facilitate clinical risk stratification29. Due to the still limited therapeutic consequences of genetic testing and according to our clinical experience the willingness of patients to perform genetic testing is low. We thus cannot supply genetic association information of cardiomyopathy and circRNA abundancy and extension of genetic analysis is a major goal for upcoming studies.
The strength of the present study is the fact that we not only compared healthy subjects with HCM patients in general, but also differentiate between HNCM and HOCM to further identify a correlation between circRNAs and disease severity. Nevertheless, results of this medium-size study needs to be replicated by larger and independent study cohorts.
In conclusion, this is the first study indicating the abundancy of disease-relevant circulating circRNAs in HCM and highlighting the importance of a set of circRNAs as possible novel indicators of HCM.
Methods
Patient data
Patients with HNCM/HOCM were enrolled at the Special Outpatient Clinic for HCM, Department of Cardiology and Angiology (Hannover Medical School). We obtained written informed consent from all patients and the study was approved by the local ethical committee of Hannover Medical School.
The diagnosis of HCM was based on the recent European guidelines for the diagnosis and management of hypertrophic cardiomyopathies4 and mainly included presence of a hypertrophic cardiac septum (≥15 mm) or combined presence of a hypertrophic cardiac septum (≥13 mm) and positive family history and/or ECG abnormalities. To differentiate between non-obstructive and obstructive subtype, HOCM was defined by a left ventricular outflow tract gradient ≥ 30 mmHg. All methods were carried out in accordance with relevant guidelines and regulations.
Blood from healthy do nors (controls) was obtained from the Hannover Medical School blood donation service.
RNA isolation from patient serum
As described previously6,7,30, collected serum blood samples were centrifuged at 2000 × g for 10 minutes at room temperature. After separation of corpuscular components, the liquid supernatant was stored at −80 °C in RNase/DNase free tubes. RNA was isolated with the miRNeasy Mini Kit (Qiagen) according to the manual. For normalization Caenorhabditis elegans miR-39-3p was added as a spike-in RNA during the process6,7,30.
Reverse transcription and real-time PCR of circRNAs
Isolated RNA was transcribed to complementary DNA (cDNA) using cDNA Synthesis Kit (Biozym) according to manufacturer’s manuals and as described previously6,7. TaqMan MircoRNA Reverse Transcription Kit (Applied Biosystems) was applied to synthesize cDNA of cel-miR-39-3p working as control. According to the literature12,13 specific primers for circ_0005402, circ_0035560, ANXA2, MBOAT2, TMEM56 and DNAJC6 were validated and afterwards quantitative real-time PCR was performed amplifying the cDNA of the four last mentioned circRNAs using iQSYBR Green Supermix (Bio-Rad). For amplifying cel-miR-39 with quantitative real-time PCR, a specific TagMan MicroRNA assay and ViiA7 machine (Applied Biosystems) was used.
Following primers were used in this study:
circ_0005402 forward | TTTCGGACACATCTGGTGAC |
circ_0035560 forward | CACCTGGAGACGGTGATTTT |
rev-circ_universal | CCGCTCAGCATCAAAGTTAGT |
MBOAT2 forward | AGTGCAAGATAAAGGCCCAAA |
MBOAT2 reverse | TGATCATCATAGGAGTGGAGAACA |
TMEM56 forward | CATCATTGTGCGTCCCTGTATG |
TMEM56 reverse | GCTGAGACTATTGAAACCTGGAGA |
DNAJC6 forward | CCAGACATCTTGACCACTACACA |
DNAJC6 reverse | ATGTGTCTTTGAGGGTGTCTTT |
Statistical analysis
Comprehensive statistical evaluation was performed as described previously31,32.
In specific we used the statistical software package R (www.r-project.org) for statistical analyses. Descriptive statistics were used to summarize the characteristics of the study population. Kolmogorov-Smirnov test was used to test normality. Data were presented as the means ± standard deviation (SD) for continuous variables with normal distributions, medians (interquartile range) for continuous variables with skewed distributions and as frequencies (percentage) for categorical variables. Continuous variables were compared between groups using Student´s t test, Krukal–Wallis test or Mann–Whitney U test. Categorical variables were compared between groups using Fisher’s exact test or chi-squared test. Spearman’s rho coefficient was used to assess the correlation between continuous variables. Logistic regression analyses were performed to examine in detail the association between circRNAs and HCM, HNCM or HOCM. To establish whether the observed association could be influenced by potential cofounding factors, the models were adjusted by age and sex. The results were presented as odds ratio (OR) and 95% confidence intervals (CI). Receiver operating characteristic (ROC) curves were constructed for circRNAs using the area under the ROC curve (AUC) as the global discrimination value measure. P-value < 0.05 was considered statistically significant.
Data availability
All data generated or analyzed during this study are included in this published article and its Supplementary Information files.
References
Maron, B. J. Clinical Course and Management of Hypertrophic Cardiomyopathy. N Engl J Med. 379, 655–668 (2018).
Maron, B. J., Rowin, E. J. & Maron, M. S. Global Burden of Hypertrophic Cardiomyopathy. JACC Heart Fail. 6, 376–378 (2018).
Semsarian, C., Ingles, J., Maron, M. S. & Maron, B. J. New perspectives on the prevalence of hypertrophic cardiomyopathy. J Am Coll Cardiol. 65, 1249–1254 (2015).
Authors/Task Force members, Elliott, P. M. et al. ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur Heart J. 2014(35), 2733–2779 (2014).
de Gonzalo-Calvo, D. et al. Circulating non-coding RNAs in biomarker-guided cardiovascular therapy: a novel tool for personalized medicine? Eur Heart J. 40, 1643–1650 (2019).
Kitow, J. et al. Mitochondrial long noncoding RNAs as blood based biomarkers for cardiac remodeling in patients with hypertrophic cardiomyopathy. Am J Physiol Heart Circ Physiol. 311, H707–12 (2016).
Derda, A. A. et al. Blood-based microRNA signatures differentiate various forms of cardiac hypertrophy. Int J Cardiol. 196, 115–122 (2015).
Song, L. et al. MiR-451 is decreased in hypertrophic cardiomyopathy and regulates autophagy by targeting TSC1. J Cell Mol Med. 18, 2266–2274 (2014).
Roncarati, R. et al. Circulating miR-29a, among other up-regulated microRNAs, is the only biomarker for both hypertrophy and fibrosis in patients with hypertrophic cardiomyopathy. J Am Coll Cardiol. 63, 920–927 (2014).
Altesha, M. A., Ni, T., Khan, A., Liu, K. & Zheng, X. Circular RNA in cardiovascular disease. J Cell Physiol. 234, 5588–5600 (2019).
Hang, D. et al. A novel plasma circular RNA circFARSA is a potential biomarker for non-small cell lung cancer. Cancer Med. 7, 2783–2791 (2018).
Iparraguirre, L. et al. Circular RNA profiling reveals that circular RNAs from ANXA2 can be used as new biomarkers for multiple sclerosis. Hum Mol Genet. 26, 3564–3572 (2017).
Memczak, S., Papavasileiou, P., Peters, O. & Rajewsky, N. Identification and Characterization of Circular RNAs As a New Class of Putative Biomarkers in Human Blood. PLoS One. 10, e0141214 (2015).
Jeck, W. R. et al. Circular RNAs are abundant, conserved, and associated with ALU repeats. RNA. 19, 141–157 (2013).
Werfel, S. et al. Characterization of circular RNAs in human, mouse and rat hearts. J Mol Cell Cardiol. 98, 103–107 (2016).
Hansen, T. B. et al. Natural RNA circles function as efficient microRNA sponges. Nature. 495, 384–388 (2013).
Memczak, S. et al. Circular RNAs are a large class of animal RNAs with regulatory potency. Nature. 495, 333–338 (2013).
Li, Z. et al. Exon-intron circular RNAs regulate transcription in the nucleus. Nat Struct Mol Biol. 22, 256–264 (2015).
Khan, M. A. et al. RBM20 Regulates Circular RNA Production From the Titin Gene. Circ Res. 119, 996–1003 (2016).
Gupta, S. K. et al. Quaking Inhibits Doxorubicin-Mediated Cardiotoxicity Through Regulation of Cardiac Circular RNA Expression. Circ Res. 122, 246–254 (2018).
Li, Y. et al. Circular RNA is enriched and stable in exosomes: a promising biomarker for cancer diagnosis. Cell Res. 25, 981–984 (2015).
Geng, H. H. et al. The Circular RNA Cdr1as Promotes Myocardial Infarction by Mediating the Regulation of miR-7a on Its Target Genes Expression. PLoS One. 11, e0151753 (2016).
Vausort, M. et al. Myocardial Infarction-Associated Circular RNA Predicting Left Ventricular Dysfunction. J Am Coll Cardiol. 68, 1247–1248 (2016).
Salgado-Somoza, A., Zhang, L., Vausort, M. & Devaux, Y. The circular RNA MICRA for risk stratification after myocardial infarction. Int J Cardiol Heart Vasc. 17, 33–36 (2017).
Du, W. W. et al. Foxo3 circular RNA promotes cardiac senescence by modulating multiple factors associated with stress and senescence responses. Eur Heart J. 38, 1402–1412 (2017).
Tang, C. M. et al. CircRNA_000203 enhances the expression of fibrosis-associated genes by derepressing targets of miR-26b-5p, Col1a2 and CTGF, in cardiac fibroblasts. Sci Rep. 7, 40342 (2017).
Zhou, B. & Yu, J. W. A novel identified circular RNA, circRNA_010567, promotes myocardial fibrosis via suppressing miR-141 by targeting TGF-beta1. Biochem Biophys Res Commun. 487, 769–775 (2017).
Siede, D. et al. Identification of circular RNAs with host gene-independent expression in human model systems for cardiac differentiation and disease. J Mol Cell Cardiol. 109, 48–56 (2017).
Monserrat, L. Perspectives on current recommendations for genetic testing in HCM. Glob. Cardiol. Sci. Pract. 3, 23 (2018).
Bauters, C. et al. Circulating miR-133a and miR-423-5p fail as biomarkers for left ventricular remodeling after myocardial infarction. Int.J.Cardiol. 168(3), 1837–1840 (2013).
Chatterjee, S. et al. Leukocyte telomere length correlates with hypertrophic cardiomyopathy severity. Sci Rep. 8, 11227–018-29072-8 (2018).
de Gonzalo-Calvo, D. et al. Serum microRNA-1 and microRNA-133a levels reflect myocardial steatosis in uncomplicated type 2 diabetes. Sci Rep. 7, 47–017-00070-6 (2017).
Acknowledgements
The authors acknowledge the Blood Donation Service at Hannover Medical School for collecting control blood samples. This work was supported by Junge Akademie, MHH (to K.S.), ERC grant Longheart (to T.T.) and Deutsche Forschungsgemeinschaft, TRR_267 (to T.T.) and KFO311 (to T.T. and J.B. (D.d.G.C. was a recipient of a Juan de la Cierva-Incorporación grant from the Ministry of Science Innovation and Universities (IJCI-2016-29393). CIBER Cardiovascular (CB16/11/00403 to DdG-C) is a project from Carlos III Health Institute.
Author information
Authors and Affiliations
Contributions
K.S., J.F. and T.T. perceived the original idea. A.L.W., A.P. and J.F. performed measurements and analysis. K.S., J.B., C.Z. and U.B. enrolled HCM patients at the Special Outpatient Clinic for HCM and performed echocardiography. D.d.G.C. performed statistical analysis. K.S., J.F., D.d.G.C., A.L.W. and T.T. wrote the manuscript. A.A.D. enrolled HCM patients at the Special Outpatient Clinic for HCM.
Corresponding author
Ethics declarations
Competing interests
T.T. has filed patents in the field of non-coding RNAs and is founder and holds shares of Cardior Pharmaceuticals GmbH. D.d.G.C. have licensed a patent on microRNAs as biomarkers. Other authors have no conflicts of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sonnenschein, K., Wilczek, A.L., de Gonzalo-Calvo, D. et al. Serum circular RNAs act as blood-based biomarkers for hypertrophic obstructive cardiomyopathy. Sci Rep 9, 20350 (2019). https://doi.org/10.1038/s41598-019-56617-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-56617-2
This article is cited by
-
The effects of exercise on epigenetic modifications: focus on DNA methylation, histone modifications and non-coding RNAs
Human Cell (2024)
-
CircZNF609 regulates pulmonary fibrosis via miR-145-5p/KLF4 axis and its translation function
Cellular & Molecular Biology Letters (2023)
-
Non-Coding RNA-Mediated Gene Regulation in Cardiovascular Disorders: Current Insights and Future Directions
Journal of Cardiovascular Translational Research (2023)
-
Predictive biomarkers for the early detection and management of heart failure
Heart Failure Reviews (2023)
-
Non-coding RNAs regulating mitochondrial function in cardiovascular diseases
Journal of Molecular Medicine (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
