
Abstract
Several studies have shown that dysmenorrhea increased the risk of depression. However, the association between dysmenorrhea and postpartum depression (PPD) is unclear. The purpose of this study is to evaluate the effects of dysmenorrhea on the development of PPD among Chinese women. A case-control study was performed on parturients who delivered from January 1, 2016, to December 31, 2016, at Bao an Maternal and Child Health Hospital in Shenzhen, China. The Edinburgh Postnatal Depression Scale (EPDS) was used to screen for maternal postpartum depression. Logistic regression models were used to examine the association between dysmenorrhea and the risk of PPD. A total of 360 women including 120 cases and 240 controls were enrolled. Our study showed that parturients with PPD had a higher percentage of dysmenorrhea than women without PPD (64.2% vs 47.9%, P = 0.004). In univariate analysis, we observed that dysmenorrhea increased the risk for PPD (OR = 1.95; 95% CI: 1.24–3.06; P = 0.004). In the fully adjusted model, dysmenorrhea was still significantly associated with an increased risk of PPD (OR = 2.45; 95% CI: 1.36–4.54; P = 0.003). Our data confirmed that dysmenorrhea may be a risk factor for PPD. Therefore, screening for postpartum depression should be considered in parturients with a history of dysmenorrhea.
Similar content being viewed by others

Introduction
Postpartum depression (PPD) is a disabling but treatable maternal mental disorder that affects 0.5–60% of women worldwide and leads to substantial morbidity and mortality in mothers and children1,2. Mothers who suffer from PPD are also more likely to develop depression in the future3,4. PPD is often associated with a high risk of suicide, poor marital relationships, infanticide, and poor child development5,6,7,8. Accumulative evidence suggests that domestic violence, history of depression, stressful life events, marital dissatisfaction, lack of emotional or social support, anger experience and expression, and foetal or neonatal health problems increase the risk of developing PPD9,10,11,12,13. However, many risk factors remain unknown or poorly understood.
Dysmenorrhea, or menstrual pain, is a severe, painful, cramping sensation in the lower abdomen that is often accompanied by other symptoms, such as sweating, headaches, nausea, vomiting, diarrhoea, and tremulousness, all occurring just before or during menses14. Dysmenorrhea is also the most common gynaecological complaint and has a major impact on quality of life, work productivity, and health care utilization15,16,17. Several studies have indicated that dysmenorrhea is strongly linked with depression among adolescents18,19,20,21. A published study conducted by Bahrami et al. found that individuals in the dysmenorrhea group had significantly higher depression scores than normal controls22. Similar results were observed in Balık’s study, which concluded that adolescent girls with dysmenorrhea have an increased risk of depression19. PPD and major depression share many common risk factors unrelated to pregnancy, such as history of depression, domestic violence, stressful life events, emotional stress, and poor socioeconomic status. However, it is unclear whether dysmenorrhea can also affect the development of PPD. Hence, we hypothesized that dysmenorrhea is related to the development of PPD and increases the risk of PPD.
Based on above reasons, we performed this case-control study to investigate the possible association between dysmenorrhea and the risk of PPD 6 weeks after childbirth in a hospital-based sample of Chinese women.
Results
Demographic, socioeconomic, and pregnancy-related characteristics
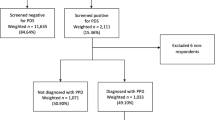
Originally, 136 PPD cases and 272 controls were invited to participate this study, but only 120 cases and 240 controls were enrolled (a response rate of 88.2%) and completed the questionnaires. The socio-demographic characteristics and pregnancy-related factors of the two groups are presented in Table 1. Between the two groups, some demographic characteristics such as age at birth, education level, employment status, BMI, or family monthly income per capita were not significantly different. However, the proportion of primipara in the case group (68.3% vs 56.3%, P = 0.027) was higher than that in the control group.
Women with PPD were significantly more likely to experience depression (35.0% vs 2.9%, P < 0.001) and anxiety (55.0% vs 13.8%, P < 0.001) during pregnancy than other women. The patients with PPD were also more likely to have a stressful life event experience (17.5% vs 5.0%, P < 0.001) compared with those in the control group. Additionally, there was a significantly higher incidence of low birth weight in the PPD patients (10.0% vs 1.3%, P < 0.001). In the case group, 77 (64.2%) women also reported a history of dysmenorrhea, which was significantly higher than the corresponding figure in the control group (64.2% vs 47.9%, P = 0.004). However, there was no significant difference in the other pregnancy-related factors, including planned pregnancy, mode of delivery, preterm birth, infant gender, or breastfeeding status, between the case group and the control group at 6 weeks.
SSRS scores
As shown in Table 2, compared with the control group, PPD patients scored significantly lower on the objective support (8.38 ± 2.97 vs 9.68 ± 2.87, respectively; P < 0.001), subjective support (20.82 ± 4.41 vs 24.20 ± 4.02, respectively; P < 0.001), and support usage (7.03 ± 1.62 vs 8.17 ± 3.67, respectively; P < 0.001) subscales.
However, the significant differences in primipara did not pass the Bonferroni corrections (Bonferroni corrected P < 0.05/18 = 0.002).
Multivariable logistic regression analysis for the association of dysmenorrhea and PPD
As shown in Table 3, dysmenorrhea was significantly associated with a higher risk of PPD in model 1 (OR = 1.95; 95% CI: 1.24–3.06; P = 0.004). After adjustment for other covariates including age, education level, BMI, employment status, parity, and family monthly income per capita, dysmenorrhea was still associated with an 85% increase in the risk of PPD (model 2: OR = 1.85; 95% CI: 1.16–2.95; P = 0.010). Considering the effects of pregnancy-related risk factors on the outcome variable, we further added those variables into the multivariable logistic regression model. As a result, the association between dysmenorrhea and the risk of PPD remained significant (model 3: OR = 2.19; 95% CI: 1.25–3.85; P = 0.006). Finally, the social support scores including those of objective support, subjective support and support usage were included in the model as continuous variables on the basis of model 3. In the fully adjusted model, women with a history of dysmenorrhea had higher prevalence of PPD compared to women without a record of dysmenorrhea (model 4: OR = 2.45; 95% CI: 1.36–4.54; P = 0.003).
Discussion
To the best of our knowledge, this is the first study to investigate the association between dysmenorrhea and the risk of PPD in a Chinese Han population. Moreover, our study found a higher risk of PPD in women with dysmenorrhea.
Little previous evidence was available on the association between dysmenorrhea and the risk of PPD; however, a number of previous studies reported that dysmenorrhea was associated with a high risk of depression18,19,20,21,22. One previous study indicated that women who had a history of dysmenorrhea were more likely to suffer from depression or had a higher score for depression compared with women without menstrual pain18. Additionally, Coleman and his colleagues also found that severe menstrual pain was an important risk factor strongly associated with depression20. Our study suggests that parturient women with dysmenorrhea have a high risk of PPD; this result is consistent with the findings from a Japanese study that included 11,341 PPD patients and 71,148 controls23. Their study demonstrated that parturients with dysmenorrhea had 1.13 times higher risk of developing PPD (OR, 1.13; 95% CI: 1.06–1.21), after adjustment for socio-demographic factors, health behavioural factors, psychiatric illness history, psychosocial factors, obstetrical factors and birth outcome factors23. However, an American study by Swenson showed that there was no significant difference in the distribution of dysmenorrhea between women with and without a positive PPD test24. Possible reasons for this difference include the different criteria used for the diagnosis of PPD and the different study designs adopted by investigators.
Based on the underlying cause of developing dysmenorrhea, dysmenorrhea is commonly classified into two categories: primary and secondary dysmenorrhea. Primary dysmenorrhea, characterized by menstrual pain without organic disease, is considered to be caused by excess secretion of prostaglandin associated with changes in oestrogen and progesterone levels25. A great number of studies have reported that changes in ovarian hormones are associated with a high risk of depression26,27. Preclinical and clinical studies have shown that oestrogen modulates the expression of genes that code for tryptophan hydroxylase, the serotonin transporter, and the 5-HT1a auto-receptor28,29. Hence, the fluctuation of oestrogen could cause an alteration in serotonin neurotransmission, which then leads to mood disorders26. Binding to receptors that are localized in the region of the brain that is involved emotional and cognitive regulation, progesterone also regulates neurotransmitter synthesis, release, and transport30,31, and further causes dysfunctional mood regulation32. In addition to the effects of hormones, in recent years, many studies have confirmed that depressive disorders are associated with increased concentrations of many pro-inflammatory cytokines, including tumour necrosis factor α (TNF-α) and interleukins (ILs)33,34,35,36. These pro-inflammatory cytokines lead to a deficit in serotonin and melatonin through the kynurenine pathway35, which is considered one of the main reasons for depression. Furthermore, a study by Ma and colleagues demonstrated that the genes encoding pro-inflammatory cytokines (IL1B, TNF, IL6, and IL8) were up-regulated in peripheral blood mononuclear cells (PBMCs) of primary dysmenorrhoeic young women during the menstrual phase37. Therefore, dysmenorrhea may lead to the development of PPD though an increase in pro-inflammatory cytokines.
Secondary dysmenorrhea is menstrual pain associated with an identifiable disease. Endometriosis is the most common cause of secondary dysmenorrhea, and its development is likely dependent on sex hormones, especially oestrogen25. A high level of localized oestrogen is frequently observed in endometriosis patients38. Clinical studies demonstrate that oestrogen can affect serotonin synthesis, receptor production, or degradation28,29, and the effects of oestrogen on serotonin are commonly considered to be important for mood.
This study is the first to investigate the relationship between dysmenorrhea and PPD among the Chinese Han population. Another strength of this research is that the potential confounding variables including socio-demographic factors and pregnancy-related risk factors, were considered in the multiple regression model. There is no denying that the present study has several limitations. First, a case-control study design cannot assess direct causality between dysmenorrhea and PPD. Second, we were not able to separate secondary from primary dysmenorrhea because we lacked information on conditions leading to secondary dysmenorrhea. Third, the EPDS is just a screening tool and not a diagnostic tool, although the measurement of PPD with the EPDS has been widely used and validated in China.
In conclusion, our study indicated that dysmenorrhea was independently associated with PPD. The risk of PPD was clearly higher in women who had history of dysmenorrhea. Therefore, screening for postpartum depression should be considered for postpartum women with persistent dysmenorrhea.
Methods
Study design and population
The present study was a case-control study carried out from January 1, 2016, to December 31, 2016, at Bao an Maternal and Child Health Hospital, Shenzhen, China. All women delivered in this hospital, were more than 18 years old, and were screened for postpartum depression using the Edinburgh Postnatal Depression Scale (EPDS), at a routine follow-up appointment 6 weeks after delivery. As described in a previous report, women with an EPDS score ≥10 were considered to have postpartum depression and were eligible for joining the case group39. PPD patients were consecutively recruited from postnatal obstetric clinics. Inclusion criteria for the case group were having a confirmed diagnosis of clinical PPD using EPDS, agreeing to participate in this survey and signing an informed consent form. However, those with severe physical illness (including infectious disease, cardiovascular disease, gastrointestinal disorder, endocrine disorder, urinary disease, and benign or malignant tumours), disability, psychotic disorders, or substance abuse problems were excluded from the study. The intent of this study was to have 2 controls for every case, and controls were randomly selected from patients who attended postnatal obstetrics clinics. Only those with an EPDS score <10 were invited to participate and assigned to the control group. The inclusion/exclusion criteria for the control group were almost identical to that of the case group, besides the absence of PPD.
Data collection and procedures
Well-qualified investigators were assigned to collect the data for this study. Some obstetricians and nurses of Bao an Maternal and Child Health Hospital served as the investigators of this study. All investigators participated in the training conducted by the first author before starting data collection. After training, the investigators carried out face-to-face interviews with the participants using a structured questionnaire, which was specially designed based on existing the literature and expert consultation. The questionnaire was used to collect data regarding socio-demographic characteristics (age, education level, employment status, height, weight, and family monthly income per capita), and the pregnancy-related risk factors (planned pregnancy, depression and anxiety during pregnancy, stressful life events, mode of delivery, gestational weeks, birth weight, gender of foetus, and infant feeding method). The accuracy of these data was then checked with the participants’ medical records. In the interviews, women were also asked whether they had a history of dysmenorrhea.
Measures
Social support
The Chinese version of the Social Support Rating Scale (SSRS) developed by Xiao ShuiYuan in 1994, was used to assess the individuals’ social support status. The SSRS consists of 10 items involving three dimensions, namely, objective support (3 items), subjective support (4 items), and support utilization (3 items)40. The total score on the SSRS ranges from 12 to 66, including objective support (range: 1–22), subjective support (range: 8–32) and support usage (range: 3–12). Higher SSRS scores indicate better social support. This tool has been proven to have good reliability and validity. Cronbach’s alpha coefficients for the total scale and subscales ranged from 0.825 to 0.89640,41.
Postpartum depression
The Edinburgh Postnatal Depression Scale (EPDS) has been widely used to evaluate maternal postpartum depression. The EPDS has 10 items, and each item is scored on a 4-point scale ranging from 0 to 3. Total scores range from 0 to 30, with higher scores reflecting an increased risk of PPD. The validity and reliability of the Chinese version of the EPDS have been reported, with a sensitivity of 0.82 and a specificity of 0.8642. In the present study, a total score of 10 or higher was defined as PPD, consistent with previous research39.
Ethics statement
All study procedures were approved by the Institutional Review Board of Tongji Medical College, Huazhong University of Science and Technology and Bao an Maternal and Child Health Hospital, Jinan University. The methodology was carried out in accordance with the approved guidelines. Written informed consent was obtained from all participants.
Statistical analysis
Categorical data are presented as numbers and percentages (%), continuous variables are described as the mean ± standard deviation (SD). Student’s t-tests were used to test continuous variables and chi-square tests were used to compare categorical data. We used Bonferroni corrections to adjust for multiple testing. The adjusted odds ratios (ORs) with 95% confidence intervals (95% CI) were used to measure the independent association between PPD development and dysmenorrhea. The statistical power to detect the difference in dysmenorrhea between the case group and control group was calculated by Power and Sample Size Calculation v3.1.2. We calculated that the power for our sample size to detect an OR of 1.50 was 0.981. The significance level was set at 5%, and all tests were two-sided. All analyses were performed using SPSS software version 18.0 (SPSS, Chicago, IL, USA).
Data availability
All data generated or analysed during this study are included in this published article.
References
Norhayati, M. N., Hazlina, N. H., Asrenee, A. R. & Emilin, W. M. Magnitude and risk factors for postpartum symptoms: a literature review. J Affect Disord 175, 34–52 (2015).
Gavin, N. I. et al. Perinatal depression: a systematic review of prevalence and incidence. Obstet Gynecol 106, 1071–1083 (2005).
Werner, E., Miller, M., Osborne, L. M., Kuzava, S. & Monk, C. Preventing postpartum depression: review and recommendations. Arch Womens Ment Health 18, 41–60 (2015).
Honjo, K. et al. Association between family members and risk of postpartum depression in Japan: Does “who they live with” matter? -The Japan environment and Children’s study. Soc Sci Med 217, 65–72 (2018).
Miksic, S. et al. Depression and Suicidality during Pregnancy. Psychiatr Danub 30, 85–90 (2018).
Lindahl, V., Pearson, J. L. & Colpe, L. Prevalence of suicidality during pregnancy and the postpartum. Arch Womens Ment Health 8, 77–87 (2005).
Guintivano, J. et al. Adverse life events, psychiatric history, and biological predictors of postpartum depression in an ethnically diverse sample of postpartum women. Psychol Med 48, 1190–1200 (2018).
Junge, C. et al. The Impact of Perinatal Depression on Children’s Social-Emotional Development: A Longitudinal Study. Matern Child Health J 21, 607–615 (2017).
Robertson-Blackmore, E. et al. Antecedent trauma exposure and risk of depression in the perinatal period. J Clin Psychiatry 74, e942–948 (2013).
Mercier, R. J., Garrett, J., Thorp, J. & Siega-Riz, A. M. Pregnancy intention and postpartum depression: secondary data analysis from a prospective cohort. BJOG 120, 1116–1122 (2013).
Howard, L. M., Oram, S., Galley, H., Trevillion, K. & Feder, G. Domestic violence and perinatal mental disorders: a systematic review and meta-analysis. PLoS Med 10, e1001452 (2013).
Tang, L., Zhu, R. & Zhang, X. Postpartum Depression and Social Support in China: A Cultural Perspective. J Health Commun 21, 1055–1061 (2016).
Bruno, A. et al. Inside-out: the role of anger experience and expression in the development of postpartum mood disorders. J Matern Fetal Neonatal Med 31, 3033–3038 (2018).
Ju, H., Jones, M. & Mishra, G. The prevalence and risk factors of dysmenorrhea. Epidemiol Rev 36, 104–113 (2014).
Nguyen, A. M., Humphrey, L., Kitchen, H., Rehman, T. & Norquist, J. M. A qualitative study to develop a patient-reported outcome for dysmenorrhea. Qual Life Res 24, 181–191 (2015).
Chen, C. X., Shieh, C., Draucker, C. B. & Carpenter, J. S. Reasons women do not seek health care for dysmenorrhea. J Clin Nurs 27, e301–e308 (2018).
Iacovides, S., Avidon, I. & Baker, F. C. What we know about primary dysmenorrhea today: a critical review. Hum Reprod Update 21, 762–778 (2015).
Gagua, T., Tkeshelashvili, B., Gagua, D. & McHedlishvili, N. Assessment of anxiety and depression in adolescents with primary dysmenorrhea: a case-control study. J Pediatr Adolesc Gynecol 26, 350–354 (2013).
Balik, G., Ustuner, I., Kagitci, M. & Sahin, F. K. Is there a relationship between mood disorders and dysmenorrhea? J Pediatr Adolesc Gynecol 27, 371–374 (2014).
Coleman, R., Morison, L., Paine, K., Powell, R. A. & Walraven, G. Women’s reproductive health and depression: a community survey in the Gambia, West Africa. Soc Psychiatry Psychiatr Epidemiol 41, 720–727 (2006).
Dorn, L. D. et al. Menstrual symptoms in adolescent girls: association with smoking, depressive symptoms, and anxiety. J Adolesc Health 44, 237–243 (2009).
Bahrami, A. et al. Neuropsychological function in relation to dysmenorrhea in adolescents. Eur J Obstet Gynecol Reprod Biol 215, 224–229 (2017).
Muchanga, S. M. J. et al. Preconception gynecological risk factors of postpartum depression among Japanese women: The Japan Environment and Children’s Study (JECS). J Affect Disord 217, 34–41 (2017).
Swenson, C. W., DePorre, J. A., Haefner, J. K., Berger, M. B. & Fenner, D. E. Postpartum depression screening and pelvic floor symptoms among women referred to a specialty postpartum perineal clinic. Am J Obstet Gynecol 218, 335 e331–335 e336 (2018).
Proctor, M. & Farquhar, C. Diagnosis and management of dysmenorrhoea. BMJ 332, 1134–1138 (2006).
Lokuge, S., Frey, B. N., Foster, J. A., Soares, C. N. & Steiner, M. Depression in women: windows of vulnerability and new insights into the link between estrogen and serotonin. J Clin Psychiatry 72, e1563–1569 (2011).
Studd, J. Personal view: Hormones and depression in women. Climacteric 18, 3–5 (2015).
Maki, P. M. & Dumas, J. Mechanisms of action of estrogen in the brain: insights from human neuroimaging and psychopharmacologic studies. Semin Reprod Med 27, 250–259 (2009).
Bethea, C. L., Lu, N. Z., Gundlah, C. & Streicher, J. M. Diverse actions of ovarian steroids in the serotonin neural system. Front Neuroendocrinol 23, 41–100 (2002).
Finocchi, C. & Ferrari, M. Female reproductive steroids and neuronal excitability. Neurol Sci 32(Suppl 1), S31–35 (2011).
Schiller, C. E., Meltzer-Brody, S. & Rubinow, D. R. The role of reproductive hormones in postpartum depression. CNS Spectr 20, 48–59 (2015).
Wharton, W., Gleason, C. E., Olson, S. R., Carlsson, C. M. & Asthana, S. Neurobiological Underpinnings of the Estrogen - Mood Relationship. Curr Psychiatry Rev 8, 247–256 (2012).
Maes, M. Major depression and activation of the inflammatory response system. Adv Exp Med Biol 461, 25–46 (1999).
Catena-Dell’Osso, M., Rotella, F., Dell’Osso, A., Fagiolini, A. & Marazziti, D. Inflammation, serotonin and major depression. Curr Drug Targets 14, 571–577 (2013).
Galecki, P. & Talarowska, M. Inflammatory theory of depression. Psychiatr Pol 52, 437–447 (2018).
Young, J. J., Bruno, D. & Pomara, N. A review of the relationship between proinflammatory cytokines and major depressive disorder. J Affect Disord 169, 15–20 (2014).
Ma, H. et al. Altered cytokine gene expression in peripheral blood monocytes across the menstrual cycle in primary dysmenorrhea: a case-control study. PLoS One 8, e55200 (2013).
Chen, P., Wang, D. B. & Liang, Y. M. Evaluation of estrogen in endometriosis patients: Regulation of GATA-3 in endometrial cells and effects on Th2 cytokines. J Obstet Gynaecol Res 42, 669–677 (2016).
Xiong, R., Deng, A., Wan, B. & Liu, Y. Prevalence and factors associated with postpartum depression in women from single-child families. Int J Gynaecol Obstet 141, 194–199 (2018).
Tong, X. et al. Social support for people with epilepsy in China. Epilepsy Behav 64, 224–232 (2016).
Liu, J. et al. Investigation of reliability and validity of the social support scale. Journal of Xinjiang Medical University 31, 1–3 (In Chinese) (2018).
Lee, D. T. et al. Detecting postnatal depression in Chinese women. Validation of the Chinese version of the Edinburgh Postnatal Depression Scale. Br J Psychiatry 172, 433–437 (1998).
Acknowledgements
This study was funded by the National Natural Science Foundation of China [Grant Number NSFC-81573166] and the Fundamental Research Funds for the Central Universities [HUST: 2016YXMS216]. The funders had no role in study design, data collection and analysis and preparation of the manuscript. We are particularly grateful to the patients agreed to participating in our study. We also acknowledge the interviewers from Bao an Maternal and Child Health Hospital, Shenzhen, China for their assistance. We are particularly grateful to the patients who agreed to participate in our study. We also acknowledge the interviewers from Bao an Maternal and Child Health Hospital, Shenzhen, China, for their assistance.
Author information
Authors and Affiliations
Contributions
All authors contributed significantly to this work. L.M. participated all preparation of this manuscript. J.L. and S.P. contributed to statistical analysis. Y.C. and T.W. took part in the sample collection. L.M. drafted the article; S.P. and Y.D. contributed to the critical revision of the article. All authors reviewed the manuscript and approved the final draft.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Meng, L., Li, J., Cheng, Y. et al. Dysmenorrhea increased the risk of postpartum depression in Chinese Han parturients. Sci Rep 9, 16579 (2019). https://doi.org/10.1038/s41598-019-53059-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-53059-8
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
