
Abstract
Qualitative similarities between hip fracture trends in different countries suggests variations of the same epidemic. We tested a single statistical shape to describe time trends in Europe, while allowing for country-level variability. Using data from 14 countries, we modelled incidence rates over time using linear mixed-effects models, including the fixed effects of calendar year and age. Random effects were tested to quantify country-level variability in background rates, timing of trend reversal and tempo of reversal. Mixture models were applied to identify clusters of countries defined by common behavioural features. A quadratic function of time, with random effects for background rates and timing of trend reversal, adjusted well to the observed data. Predicted trend reversal occurred on average in 1999 in women (peak incidence about 600 per 100 000) and 2000 in men (about 300 per 100 000). Mixture modelling of country-level effects suggested three clusters for women and two for men. In both sexes, Scandinavia showed higher rates but earlier trend reversals, whereas later trend reversals but lower peak incidences were found in Southern Europe and most of Central Europe. Our finding of a similar overall reversal pattern suggests that different countries show variations of a shared hip fracture epidemic.
Similar content being viewed by others
Introduction
Due to pathophysiology, prognosis and healthcare implications, age-related hip fractures are socially the most relevant outcome of bone fragility. In Belgium, a country with intermediate incidence, the remaining risk of hip fracture was about 20% in women aged 601 and a 24% functional decline in the year after fracture was estimated2. Mortality is also a major concern: in the UK, for instance, one-year case-fatality remained over 20% from 2000 to 20103. In comparative terms, fragility fractures account for more disability-adjusted life years than most common cancers in Europe4.
Since hip fractures almost inevitably involve hospital admission, incidence estimated from healthcare is particularly valid to compare the burden of bone fragility between populations and within the same population over time. Some European countries have a long tradition of describing secular trends of hip fractures, and evidence of increasing rates during the 1970s was found in the UK5, Sweden6, Finland7 and the Netherlands8. Subsequent increases were seen up to the 1990s in other countries, namely Austria9, Denmark10, Germany11, 12, Iceland13, Norway14, and Spain15. More recently, however, a reversal of age-specific trends was detected, first in the UK5 and Scandinavia7, 14, 16, 17, and subsequently in many other settings9, 18,19,20. As countries gained improved access to hospital records, publications on the subject grew substantially. Two comprehensive reviews21, 22 show that trend reversals in hip fracture incidence are common in European countries, even though the timing has varied between settings21. Candidate explanations for trend reversals are multiple, and include planned efforts targeting bone fragility as well as macro-level changes that may have caused decreasing fracture trends as an unpredicted effect22.
Qualitative similarities between countries led us to hypothesize that a single shape could describe the hip fracture epidemic in Europe. Specifically, there seems to be considerable country-level evidence that secular trends can be modelled as a quadratic function of time, i.e. a first period of increasing rates but decreasing acceleration followed by a short stagnation with null acceleration and finally a later period of decreasing rates with increasingly negative acceleration. Nevertheless, within a common overall pattern, specific features of trend reversals may differ between countries, namely background fracture rates, timing and tempo of reversal. The hypothesis that different countries have followed different variations of the same hip fracture epidemic is a starting point for testing mechanistic explanations and, ultimately for future policy modelling, as shown by previous successful approaches to other conditions23.
In the present work, we aimed to model recent hip fracture secular trends in different European countries and to identify clusters of countries with similar behavioural features over time.
Methods
Selection of time series and data extraction
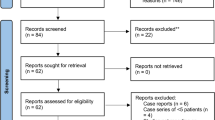
Studies were identified by searching Medline from inception to December 2015 for articles reporting trends of hip fracture incidence rates in European countries (Fig. 1). References were screened by two reviewers (AM, RL). In addition to the subject-matter filters detailed below, we applied the following formal exclusion criteria: i) articles not written in English, Portuguese, Spanish, French or Italian, ii) articles from populations outside the World Health Organization European Region, iii) non-eligible publication types (editorials, comments, guidelines, case reports and reviews), iv) studies that did not report incidence estimates, and v) studies that presented data for only one time point. Since we aimed to extract and model recent age- and sex-specific hip fracture incidence trends for different European countries, we defined methodological strategies to address the following specific issues:
-
(a)
Validity of estimates: we selected only studies that calculated incidence rates by using as numerator the number of cases ascertained through hospital records in a defined time frame and as denominator the whole population in the catchment area, i.e. we excluded studies that presented incidence estimates obtained by following closed cohorts or through repeated surveys of hospitals;
-
(b)
Replicability: we chose papers that provided sex- and age-specific incidence rates as part of their results or supplementary materials. In the case where estimates were provided in the graphical form, authors were contacted and asked to provide the raw incidence rates. All papers that did not present estimates that could be directly used as inputs for the model were excluded, even if they examined incidence trends. This included, for instance, papers that presented only age-standardized or model-predicted estimates;
-
(c)
Geographic coverage: to improve comparability of target populations between countries, studies were eligible only if they covered the whole population of each country; those with regional coverage were excluded;
-
(d)
Homogeneity: eligible papers used official hospital and demographic statistics to compute rates and that had national coverage. As such, it is very probable, and indeed desirable, that publications regarding the same country during the same time period have worked on the same raw data or its subsets. Further differences are likely due to specific methodological options such as diagnosis codes considered eligible, correction for readmissions or age-groups considered. Therefore, to avoid repetitions that would cause an artefactual increase in statistical power without adding information, we opted to use a single time series per country. The selection of the study to include was independent of the conclusion of that individual study with regard to the trend examined and was guided by model quality criteria defined on item e);
-
(e)
Modelling quality: to improve model fit, when time series overlapped within the same country and year, we defined the following selection criteria, in order of preference: 1) wider time span, 2) more recent estimates and 3) shorter intervals between estimates. This implied that whenever there was more than one time series per country we started by excluding the series with the shortest time span. If time spans had the same width, we excluded the oldest series. In case calendar periods also overlapped, we excluded the one with the largest intervals between time points.

Flowchart of articles for data extraction. Abbreviations: WHO: World Health Organization, AUT: Austria, DNK: Denmark, EST: Estonia, FIN: Finland, FRA: France, DEU: Germany, ITA: Italy, NLD: the Netherlands, NOR: Norway, PRT: Portugal, ESP: Spain, SWE: Sweden, CHE: Switzerland, GBR: UK-England.
We identified eligible papers for the following 14 countries: Austria9, Denmark17, Estonia24, Finland7, France25, Germany12, Italy26, the Netherlands27, Norway28, Portugal29, Spain30, Sweden31, Switzerland18, and the UK – England32. Series differed between countries in time span, periodicity and age groups considered, but no data imputation was conducted (Table 1). From each paper, we extracted sex- and age-specific incidence rates of hip fracture for that country in each year. Estimates referred to the age groups defined in each paper and we indexed each rate to the midpoint of the corresponding age category.
Modelling of the effects of age and calendar year
We started by building a model to describe the overall effects of calendar year and age using pooled data from all countries. Following our a priori hypothesis, the natural logarithms (log) of sex-specific fracture rates were modelled as a quadratic function of the calendar year. The well-known (fixed) effect of age was included as the fractional polynomial that best predicted the observed curvature. Both age and calendar year were standardized to zero mean and unit variance. The fixed-effects component of the models were of the form:
with residuals ε following a standard normal distribution. The existence of a significant variability at the country level among the rates was tested through the inclusion of random effects, fitted by restricted maximum likelihood33.
Random effects were considered: at the intercept level, to represent background fracture rates; on the linear effect of calendar year, to represent timing of trend reversal; and on the quadratic effect of calendar year, to represent tempo of trend reversal. For the evaluation of the goodness-of-fit and comparisons between models four indices were used: the Bayesian Information Criterion (BIC), the correlation coefficient between predicted and observed values, the Relative Squared Error (RSE) and the Relative Absolute Error (RAE). The RSE (resp. RAE) is defined as the ratio between the total squared (resp. absolute) error associated with the model prediction and the total squared (resp. absolute) error of the simple predictor of the average of the observed values34. The predicted values for the calendar year of trend reversal (h) and the maximum incidence rate (k), for the sample mean age, were computed as the coordinates of the vertex of each country-specific parabola:
Model-based country clustering
Once the models were obtained, the country specific features exhibited by the models random coefficients were clustered by Gaussian mixture models35. The aim was to group countries according to their fitted features over time. Gaussian mixture modelling is a probabilistic method to identify homogeneous subgroups within a population assuming that the observed data come from a mixture of a finite number of Gaussian distributions. The characteristics (orientation, volume and shape) of the distributions are estimated from the data and can be allowed to vary between clusters or constrained to be the same for all clusters36. For each sex, we selected a cluster solution from among the three with the lowest BIC (Supplementary material)37. The interpretation of the clusters was based on the values of the peak incidence rates and timing of trend reversal.
Data analysis was carried out with the software R 2.14.138 using the packages mfp39, nlme40, and mclust41 for model fitting by fractional polynomials, mixed-modelling and model-based clustering, respectively.
Results
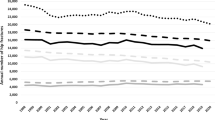
Figure 2 shows the predicted average trajectories of hip fracture incidence rates over calendar year and age. From the fixed effects model component, the predicted year of trend reversal was on average 1999 in women (at a peak incidence rate of about 600 per 100 000) and 2000 in men (about 300 per 100 000 men). Plots of age effects (Fig. 2) confirmed the dramatic increase in incidence rates with ageing, occurring at a faster rate in women. Observed and predicted fracture rates in each country are shown as Supplementary material.

Predicted fixed effects of calendar year and age on hip fracture incidence in women (dashed line) and men (solid line). To plot predicted values, the effect of calendar year was modelled for the average age in the sample (74 years) and the effect of age modelled for the average calendar year (2000).
When modelling country-level random effects (Table 2), we found that including random terms for the intercept and year slope improved the variability explained: compared to a model with fixed effects only, Model 1 (random intercept) explained 47.6% of the residual variability in women and 56.6% in men, whereas in Model 2 (random intercept and year slope), these proportions were 48.6% and 57.4%, respectively. Improvements from Model 1 to 2 were significant, as assessed through the likelihood ratio test. Adding a random quadratic effect of year did not improve the model’s predictive ability. Goodness-of-fit indices also suggested good adjustment of Model 2 to the observed data, with no substantial improvement in Model 3. In practical terms, this indicates that countries differed regarding background fracture rates and timing of trend reversal, whereas the tempo of trend reversal did not show significant intercountry variability.
Table 3 presents the predicted peak hip fracture incidence rates and calendar years of trend reversal by country, including extrapolated estimates for countries where the reversal was predicted outside of the time span covered by empirical data. Predicted peak fracture rates were lowest in Portugal (376.0 per 100 000 women and 156.9 per 100 000 men) and highest in Sweden (1389.8 per 100 000 women and 742.4 per 100 000 men). In terms of timing, the earliest trend reversals were predicted between 1986 and 1987 among women in Sweden and Denmark, whereas in men the earliest reversals were predicted between 1990 and 1992 in Switzerland, Denmark and Sweden.
After extracting country-level random coefficients and applying mixture models, we found appropriate cluster solutions with three country groups for women and two groups for men. The distributions of coefficients for background rates (k) and timing of reversal (h) are presented in Fig. 3, together with maps showing the geographical distribution of country clusters.

Distribution of calendar year of trend reversal (boxplots on the left) and peak incidence rates (boxplots on the right) in country clusters and the geographical distribution of countries in each cluster (panel a: women; panel b: men). Maps generated with ArcGIS version 10.3, by the Environmental Systems Research Institute (ESRI).
In women, clusters were characterized by:
-
(1)
A later trend reversal and an intermediate peak incidence: Austria, Finland, and Switzerland, where fractures peaked on average in the mid-1990s with incidence rates between 600 and 700 per 100 000 women.
-
(2)
An earlier trend reversal and a higher peak incidence: Denmark, Norway and Sweden, where fracture rates peaked on average in the late 1980s with average incidence rates above 1000 per 100 000 women.
-
(3)
A later trend reversal and a lower peak incidence: Estonia, France, Germany, Italy, the Netherlands, Portugal, Spain, and the UK (England), where rates peaked on average in the mid-1990s with levels below 600 per 100 000 women.
Among men, clusters were:
-
(1)
A later trend reversal and a lower peak incidence: Austria, Finland, France, Germany, Italy, the Netherlands, Portugal, Spain, and the UK (England), where fractures peaked on average in the early 2000s with an average incidence below 300 per 100 000 men.
-
(2)
An earlier trend reversal and a higher peak incidence: Denmark, Estonia, Norway, Sweden, and Switzerland, where fracture rates peaked on average in the mid-1990s with an average incidence above 500 per 100 000 men.
Discussion
We found that recent time trends of hip fracture incidence in 14 European countries can be described within the same overall pattern of secular trend reversal: rates have evolved approximately as a quadratic function of time with significant intercountry variability in the timing of reversal and peak fracture rates.
Previous evidence syntheses involving different countries examined specific aspects of the hip fracture epidemic within each country using aggregate measures such as annual percent change21, 22. These approaches are quite useful to examine break points, but are mostly interpretable at the country level and do not allow for quantitatively assessing whether the trend is generalizable to different settings. In the present work, we extracted sex- and age-specific rates for each country, and tested an overall quantitative behaviour, while allowing for country-level variability. To the best of our knowledge, this is the first study to bring together two key features of hip fracture epidemiology: background fracture rates and timing of trend reversal. Another important contribution was the identification of clusters from model-based statistical similarities rather than by imposing geographical proximity.
Our main modelling assumption was that trends could be described as a quadratic function of time in all countries. This option allowed to estimate a reversal timing for each country even when country-specific empirical data did not capture an equivalent time frame, in terms of epidemiological meaning, in all settings. However, oscillations that would produce the same or different adjustment to the model may have occurred outside of the time span considered or between two time points modelled. As such, reversal timing predicted at the country-level – which, as described in Table 3, was extrapolated beyond the time span covered by observed data for a number of countries – should be interpreted with caution and bearing in mind the a priori assumption of a single shape for all countries. Nevertheless, the option for a quadratic function seems plausible both mechanistically and empirically. As a multifactorial outcome resulting from multiple influences throughout life42, we expect the risk of fragility fracture to show smooth rather than abrupt changes over time. Empirically, our assumption is supported both by the fit indices of our mixed-effects model and by the fact that most papers included in our analysis either focus on describing trend reversals or show data where a previous or concurrent reversal is plausible even if not specifically tested. A further validation is the external replication of reversals in studies not included, e.g. outside of the European region43, 44 or using alternative methodological approaches45. Regarding the effect of age, we opted to use categories as defined in each publication and their midpoint as the index age. This was based on an assumption of constant risk within each age group, which might be unrealistic, especially when classes are wide. However, most countries used 5-year age groups, where such an assumption is more likely to hold. In addition, our estimates of age effect on fracture incidence seem consistent with a wealth of previous knowledge21, 46.
We found that the behaviour of hip fracture incidence over time could be explained as a function of timing and background rates and that the tempo of reversal was not a key source of variability. It should be noted that country-level effects represent variability not only of background fracture rates and timing of trend reversal – which were our main focus – but also of methodological options in each paper whose data we used, since estimates may not be homogeneous between countries regarding coverage, case definition or additional eligibility criteria. However, hip fractures in high-income countries are rarely managed without hospital admission, which is in favour of comparable coverage between countries. Regarding case definition, all papers adopted ICD coding, but both the 9th and 10th revisions were used and not all eligible codes overlapped between studies. In addition, some estimates were corrected for multiple admissions, while others were not. Despite that, we have no reason to suspect substantial variations in the validity of estimates over time within each country. Since our main goal was to capture the overall shape of the trend in each country, rather than to produce country comparisons at each time point, we do not believe that these issues have seriously affected our main findings. Indeed, our cluster grouping of countries is largely compatible with previous stratification on the basis of background rates47, especially regarding Scandinavia and Southern Europe, which supports that our model does distinguish the relative burden between settings. A particularly clear example reflected in our cluster solution is that of Estonia, where men have incidence rates close to those of Scandinavia, while women show rates similar to those observed in Southern Europe24. A specific case where the present model was not consistent with long-term historical data was the UK. Indeed, fracture rates were reported to have levelled off before 1985, with a breakpoint in 19785. We obtained a predicted peak rate at a much later date, which results from our choice of a later time series where such a breakpoint would, by definition, not be captured32. An interpretation may be that, up to the 1980s, the UK had an epidemic closer to that observed in Scandinavia, which later stabilized at lower levels, producing a recent behaviour more similar to that observed in Central and Southern Europe, with a second, smoother breakpoint captured by our cluster assignment. An interesting explanation for the cluster structure we propose (where there is statistical dependence between peak rates and timing of reversal) might be a lower threshold for trend reversal in countries with higher incidence. It seems indeed plausible that the fraction of the population in whom a fracture event was prevented was probably at a lower risk to begin with and was therefore more likely to have benefited from an overall decreasing trend.
Several mechanisms have been proposed to explain the widespread improvement in fracture rates22. A set of hypotheses relates to planned efforts targeting bone fragility, such as increasing availability of bone density testing, a growing uptake of pharmacological treatment of osteoporosis and menopausal hormone therapy, or better clinical management after a first fracture. However, trend reversals in many countries began before these strategies were widespread5. Additionally, reversals have been described in both sexes whereas osteoporosis management has much higher coverage (even though with a low population impact) in women17. Another set of hypotheses relates to macro-level changes that may have caused decreasing fracture trends as an unpredicted effect. Improvements in health and nutrition throughout the 20th century likely increased adult peak bone mass in younger cohorts, which is an early determinant of fracture48. As for shorter term risk factors, prosperity also brought about an increased frequency of overweight which, despite its deleterious effects, is protective of fragility fractures in adults. Additional important changes may include increased physical activity, and less frequent smoking and drinking habits28. There is also some empirical evidence that upstream factors that may influence trauma severity, such as urbanization, have followed similar time trends as hip fractures22. It should be noted, however, that our study did not aim to disentangle short- from long-term effects on trends, such as those that would be obtained from a formal age-period-cohort analysis. Thus, our findings regarding the effects of calendar period and age describe the hip fracture epidemic at the turn of the century but partly reflect earlier birth cohort influences, which amount to periods long before the fracture event itself and result from accumulated exposures throughout the life course.
Even though several explanations for trend reversals have been put forward, assessing their plausibility is challenging. Specifically, our findings suggest that the determinants of hip fracture trends may have evolved in different ways between high- and low-risk countries. Our proposal of a single shape to model secular trends in different countries provides a basis for examining candidate explanations in several settings simultaneously.
This study shows that it is plausible that recent hip fracture incidence rates in European countries can be described within the same overall pattern of secular trend reversal, with significant intercountry variability in the timing of reversal and peak fracture rates. This provides a quantitative basis for mechanistic explanations and may ultimately contribute to policy modelling.
References
Hiligsmann, M., Bruyere, O., Ethgen, O., Gathon, H. J. & Reginster, J. Y. Lifetime absolute risk of hip and other osteoporotic fracture in Belgian women. Bone 43, 991–994, doi:10.1016/j.bone.2008.08.119 (2008).
Boonen, S. et al. Functional outcome and quality of life following hip fracture in elderly women: a prospective controlled study. Osteoporos Int. 15, 87–94, doi:10.1007/s00198-003-1515-z (2004).
Klop, C. et al. Mortality in British hip fracture patients, 2000–2010: a population-based retrospective cohort study. Bone 66, 171–177, doi:10.1016/j.bone.2014.06.011 (2014).
Johnell, O. & Kanis, J. A. An estimate of the worldwide prevalence and disability associated with osteoporotic fractures. Osteoporos Int. 17, 1726–1733, doi:10.1007/s00198-006-0172-4 (2006).
Spector, T. D., Cooper, C. & Lewis, A. F. Trends in admissions for hip fracture in England and Wales, 1968–85. BMJ (Clinical research ed.) 300, 1173–1174 (1990).
Gullberg, B. et al. Incidence of hip fractures in Malmo, Sweden (1950–1991). Bone 14(Suppl 1), S23–29 (1993).
Korhonen, N. et al. Continuous decline in incidence of hip fracture: nationwide statistics from Finland between 1970 and 2010. Osteoporos Int. 24, 1599–1603, doi:10.1007/s00198-012-2190-8 (2013).
Boereboom, F. T., Raymakers, J. A., de Groot, R. R. & Duursma, S. A. Epidemiology of hip fractures in The Netherlands: women compared with men. Osteoporos Int. 2, 279–284 (1992).
Dimai, H. P. et al. Epidemiology of hip fractures in Austria: evidence for a change in the secular trend. Osteoporos Int. 22, 685–692, doi:10.1007/s00198-010-1271-9 (2011).
Giversen, I. M. Time trends of age-adjusted incidence rates of first hip fractures: a register-based study among older people in Viborg County, Denmark, 1987–1997. Osteoporos Int. 17, 552–564, doi:10.1007/s00198-005-0012-y (2006).
Wildner, M., Casper, W. & Bergmann, K. E. A secular trend in hip fracture incidence in East Germany. Osteoporos Int. 9, 144–150, doi:10.1007/s001980050128 (1999).
Icks, A., Haastert, B., Wildner, M., Becker, C. & Meyer, G. Trend of hip fracture incidence in Germany 1995–2004: a population-based study. Osteoporos Int. 19, 1139–1145, doi:10.1007/s00198-007-0534-6 (2008).
Siggeirsdottir, K. et al. Epidemiology of fractures in Iceland and secular trends in major osteoporotic fractures 1989–2008. Osteoporos Int. 25, 211–219, doi:10.1007/s00198-013-2422-6 (2014).
Lofthus, C. M. et al. Epidemiology of hip fractures in Oslo, Norway. Bone 29, 413–418 (2001).
Hernandez, J. L. et al. Trend in hip fracture epidemiology over a 14-year period in a Spanish population. Osteoporos Int. 17, 464–470, doi:10.1007/s00198-005-0008-7 (2006).
Rosengren, B. E. et al. Forearm bone mineral density and incidence of hip fractures in Swedish urban and rural men 1987–2002. Scand J Public Healt 40, 102–108, doi:10.1177/1403494811425604 (2012).
Abrahamsen, B. & Vestergaard, P. Declining incidence of hip fractures and the extent of use of anti-osteoporotic therapy in Denmark 1997–2006. Osteoporos Int. 21, 373–380, doi:10.1007/s00198-009-0957-3 (2010).
Lippuner, K. et al. Fracture hospitalizations between years 2000 and 2007 in Switzerland: a trend analysis. Osteoporos Int. 22, 2487–2497, doi:10.1007/s00198-010-1487-8 (2011).
Goettsch, W. G., de Jong, R. B., Kramarz, P. & Herings, R. M. C. Developments of the incidence of osteoporosis in The Netherlands: a PHARMO study. Pharmacoepidem Dr S 16, 166–172, doi:10.1002/pds.1245 (2007).
Briot, K., Maravic, M. & Roux, C. Changes in number and incidence of hip fractures over 12 years in France. Bone 81, 131–137, doi:10.1016/j.bone.2015.07.009 (2015).
Cooper, C. et al. Secular trends in the incidence of hip and other osteoporotic fractures. Osteoporos Int. 22, 1277–1288, doi:10.1007/s00198-011-1601-6 (2011).
Ballane, G., Cauley, J. A., Luckey, M. M. & Fuleihan Gel, H. Secular trends in hip fractures worldwide: opposing trends East versus West. Journal of bone and mineral research: the official journal of the American Society for Bone and Mineral Research 29, 1745–1755, doi:10.1002/jbmr.2218 (2014).
Unal, B., Critchley, J. A. & Capewell, S. Explaining the decline in coronary heart disease mortality in England and Wales between 1981 and 2000. Circulation 109, 1101–1107, doi:10.1161/01.cir.0000118498.35499.b2 (2004).
Jurisson, M., Vorobjov, S., Kallikorm, R., Lember, M. & Uuskula, A. The incidence of hip fractures in Estonia, 2005–2012. Osteoporos Int. 26, 77–84, doi:10.1007/s00198-014-2820-4 (2015).
Maravic, M., Taupin, P., Landais, P. & Roux, C. Change in hip fracture incidence over the last 6 years in France. Osteoporos Int. 22, 797–801, doi:10.1007/s00198-010-1255-9 (2011).
Piscitelli, P. et al. Updated incidence rates of fragility fractures in Italy: extension study 2002–2008. Clinical cases in mineral and bone metabolism: the official journal of the Italian Society of Osteoporosis, Mineral Metabolism, and Skeletal Diseases 8, 54–61 (2011).
Hartholt, K. A. et al. The epidemic of hip fractures: are we on the right track? PloS one 6, e22227, doi:10.1371/journal.pone.0022227 (2011).
Omsland, T. K. et al. Hip fractures in Norway 1999–2008: time trends in total incidence and second hip fracture rates: a NOREPOS study. European journal of epidemiology 27, 807–814, doi:10.1007/s10654-012-9711-9 (2012).
Alves, S. M. et al. Osteoporotic hip fractures: bisphosphonates sales and observed turning point in trend. A population-based retrospective study. Bone 53, 430–436, doi:10.1016/j.bone.2012.12.014 (2013).
Azagra, R. et al. Changing trends in the epidemiology of hip fracture in Spain. Osteoporos Int. 25, 1267–1274, doi:10.1007/s00198-013-2586-0 (2014).
Nilson, F., Moniruzzaman, S., Gustavsson, J. & Andersson, R. Trends in hip fracture incidence rates among the elderly in Sweden 1987–2009. Journal of public health (Oxford, England) 35, 125–131, doi:10.1093/pubmed/fds053 (2013).
Wu, T. Y. et al. Admission rates and in-hospital mortality for hip fractures in England 1998 to 2009: time trends study. Journal of public health (Oxford, England) 33, 284–291, doi:10.1093/pubmed/fdq074 (2011).
Pinheiro, J. C. & Bates, D. M. Mixed-effects models in S and S-PLUS (Springer, 2000).
Witten, I. & Frank, E. Data Mining: Practical machine learning tools and techniques (2005).
Fraley, C. & Raftery, A. E. Model-based clustering, discriminant analysis, and density estimation. J Am Stat Assoc 97, 611–631, doi:10.1198/016214502760047131 (2002).
Fraley, C. & Raftery, A. E. Bayesian regularization for normal mixture estimation and model-based clustering. J Classif 24, 155–181, doi:10.1007/s00357-007-0004-5 (2007).
Schwarz, G. Estimating Dimension of a Model. Ann Stat 6, 461–464, doi:10.1214/aos/1176344136 (1978).
R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL http://www.R-project.org/ (2013).
Ambler, G. & Benner, A Multivariable Fractional Polynomials Version 1.5.2 (2015).
Pinheiro, J. C. & Bates, D. M Linear and Nonlinear Mixed Effects Models. R Package Version 3.1-124 (2016).
Fraley, C., Raftery, A. E., Murphy, B. & Scrucca, L. Mclust version 4 for R: normal mixture modeling and model-based clustering, classification, and density estimation. Technical report no. 597. Department of Statistics, University of Washington (2012).
Bouxsein, M. L. Determinants of skeletal fragility. Best practice & research. Clinical rheumatology 19, 897–911, doi:10.1016/j.berh.2005.07.004 (2005).
Brauer, C. A., Coca-Perraillon, M., Cutler, D. M. & Rosen, A. B. Incidence and mortality of hip fractures in the United States. Jama 302, 1573–1579, doi:10.1001/jama.2009.1462 (2009).
Leslie, W. D. et al. Trends in hip fracture rates in Canada. Jama 302, 883–889, doi:10.1001/jama.2009.1231 (2009).
Lyritis, G. P., Rizou, S., Galanos, A. & Makras, P. Incidence of hip fractures in Greece during a 30-year period: 1977–2007. Osteoporos Int. 24, 1579–1585, doi:10.1007/s00198-012-2154-z (2013).
Kanis, J. A., Johnell, O., Oden, A., Johansson, H. & McCloskey, E. FRAX and the assessment of fracture probability in men and women from the UK. Osteoporos Int. 19, 385–397, doi:10.1007/s00198-007-0543-5 (2008).
Kanis, J. A. et al. A systematic review of hip fracture incidence and probability of fracture worldwide. Osteoporos Int. 23, 2239–2256, doi:10.1007/s00198-012-1964-3 (2012).
Alves, S. M., Castiglione, D., Oliveira, C. M., de Sousa, B. & Pina, M. F. Age-period-cohort effects in the incidence of hip fractures: political and economic events are coincident with changes in risk. Osteoporos Int. 25, 711–720, doi:10.1007/s00198-013-2483-6 (2014).
Acknowledgements
We gratefully acknowledge Dr. Thierry Chevalley (Switzerland), Dr. Niina Korhonen (Finland), Dr. Finn Nilson (Sweden), Dr. Tone Kristin Omsland (Norway) and Dr. Manfred Wildner (Germany) for kindly providing age- and sex-specific rates for the present paper. The work received funding through grants to RL and TM from the Portuguese Foundation for Science and Technology (refs SFRH/BPD/88729/2012 and SFRH/BD/92370/2013).
Author information
Authors and Affiliations
Contributions
R.L. defined the systematic review strategy, supported reference screening, extracted data, analysed part of the information and drafted the paper, A.M. and P.S. screened references and extracted data for analysis, M.S. and A.R.G. conducted and supervised, respectively, the statistical analysis of the time series, including the mixed-effects regression modelling and mixture models, T.M. validated data with external sources and assisted in drafting the paper, A.R.G., C.C. and H.B. supervised the conceptual aspects of the model and the intellectual content of the manuscript in general. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lucas, R., Martins, A., Severo, M. et al. Quantitative modelling of hip fracture trends in 14 European countries: testing variations of a shared reversal over time. Sci Rep 7, 3754 (2017). https://doi.org/10.1038/s41598-017-03847-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-03847-x
This article is cited by
-
Continuously declining incidence of fall injuries in older adults: nationwide statistics from Finland between 1970 and 2016
European Geriatric Medicine (2018)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
