
Abstract
The annual incidence of infective endocarditis (IE) is estimated to be between 15 and 80 cases per million persons in population-based studies. The incidence of IE is markedly increased in patients with valve prostheses (>4 per 1,000) or with prior IE (>10 per 1,000). The interaction between platelets, microorganisms and diseased valvular endothelium is the cause of vegetations and valvular or perivalvular tissue destruction. Owing to its complexity, the diagnosis of IE is facilitated by the use of the standardized Duke–Li classification, which combines two major criteria (microbiology and imaging) with five minor criteria. However, the sensitivity of the Duke–Li classification is suboptimal, particularly in prosthetic IE, and can be improved by the use of PET or radiolabelled leukocyte scintigraphy. Prolonged antibiotic therapy is mandatory. Indications for surgery during acute IE depend on the presence of haemodynamic, septic and embolic complications. The most urgent indications for surgery are related to heart failure. In the past decade, the prevention of IE has been reoriented, with indications for antibiotic prophylaxis now limited to patients at high risk of IE undergoing dental procedures. Guidelines now emphasize the importance of nonspecific oral and cutaneous hygiene in individual patients and during health-care procedures.
Key points
-
Infective endocarditis (IE) is a rare disease, but its incidence is highly variable according to the underlying heart disease; incidence is highest in patients with prior endocarditis.
-
The diagnosis of IE combines different factors that are not specific for IE when considered individually; the Duke–Li classification is the reference diagnostic criteria for IE but has suboptimal sensitivity.
-
Echocardiography remains the first-line imaging modality for the diagnosis of IE; growing evidence supports the usefulness of nuclear imaging in doubtful cases occurring on foreign material.
-
The main complications of IE are heart failure, persistent sepsis (in particular owing to perivalvular extension of infection) and embolic events, most often cerebral in location.
-
Treatment of IE is based on prolonged antibiotic therapy; valvular surgery is performed in approximately half of patients with IE during the initial course of antibiotic therapy.
-
Indications for antibiotic prophylaxis have been downgraded in guidelines, which now emphasize the importance of nonspecific hygiene measures.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$29.99 / 30 days
cancel any time
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others
References
Osler, W. The Gulstonian lectures, on malignant endocarditis. Br. Med. J. 1, 577–579 (1885).
Murdoch, D. R. et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: the International Collaboration on Endocarditis-Prospective Cohort Study. Arch. Intern. Med. 169, 463–473 (2009). This paper provides an assessment of the presentation and prognosis of IE in a large international cohort.
Selton-Suty, C. et al. Preeminence of Staphylococcus aureus in infective endocarditis: a 1-year population-based survey. Clin. Infect. Dis. 54, 1230–1239 (2012). This is a nationwide French population-based study with individual validation of IE cases.
Toyoda, N. et al. Trends in infective endocarditis in California and New York state, 1998–2013. JAMA 317, 1652–1660 (2017).
Thornhill, M. H. et al. Quantifying infective endocarditis risk in patients with predisposing cardiac conditions. Eur. Heart. J. 39, 586–595 (2018). This is a recent estimate of the incidence of IE according to underlying heart disease from a nationwide English database.
Østergaard, L. et al. Long-term causes of death in patients with infective endocarditis who undergo medical therapy only or surgical treatment: a nationwide population-based study. Eur. J. Cardiothorac. Surg. 54, 860–866 (2018).
Verhagen, D. W. M., Hermanides, J. & Korevaar, J. C. Health-related quality of life and posttraumatic stress disorder among survivors of left-sided native valve endocarditis. Clin. Infect. Dis. 48, 1559–1565 (2009).
Tleyjeh, I. M. et al. A systematic review of population-based studies of infective endocarditis. Chest 132, 1025–1035 (2007).
Iung, B. & Vahanian, A. Epidemiology of acquired valvular heart disease. Can. J. Cardiol. 30, 962–970 (2014).
Delahaye, F. et al. Systematic search for present and potential portals of entry for infective endocarditis. J. Am. Coll. Cardiol. 67, 151–158 (2016).
Østergaard, L. et al. Incidence of infective endocarditis among patients considered at high risk. Eur. Heart J. 39, 623–629 (2018).
Østergaard, L. et al. Incidence of infective endocarditis in patients considered at moderate risk. Eur. Heart J. 40, 1355–1361 (2019). This is a recent estimate of the incidence of IE according to underlying heart disease from a nationwide Danish database.
Regueiro, A. et al. Association between transcatheter aortic valve replacement and subsequent infective endocarditis and in-hospital death. JAMA 316, 1083–1092 (2016). This is a comprehensive review of the incidence, presentation and prognosis of IE after TAVI.
Butt, J. H. et al. Long-term risk of infective endocarditis after transcatheter aortic valve replacement. J. Am. Coll. Cardiol. 73, 1646–1655 (2019).
Kuijpers, J. M. et al. Incidence, risk factors, and predictors of infective endocarditis in adult congenital heart disease: focus on the use of prosthetic material. Eur. Heart. J. 38, 2048–2056 (2017).
Malekzadeh-Milani, S. et al. French national survey on infective endocarditis and the Melody valve in percutaneous pulmonary valve implantation. Arch. Cardiovasc. Dis. 111, 497–506 (2018).
Abdelghani, M. et al. Infective endocarditis after Melody valve implantation in the pulmonary position: a systematic review. J. Am. Heart Assoc. 7, e008163 (2018).
Cahill, T. J. et al. Antibiotic prophylaxis for infective endocarditis: a systematic review and meta-analysis. Heart 103, 937–944 (2017).
Holland, T. L. et al. Infective endocarditis. Nat. Rev. Dis. Primers 2, 160159 (2016).
Slipczuk, L. et al. Infective endocarditis epidemiology over five decades: a systematic review. PLOS ONE 8, e82665 (2013).
Iung, B. & Vahanian, A. Epidemiology of valvular heart disease in the adult. Nat. Rev. Cardiol. 8, 162–172 (2011).
Benito, N. et al. Health care-associated native valve endocarditis: importance of non-nosocomial acquisition. Ann. Intern. Med. 150, 586–594 (2009).
Fernandez-Hidalgo, N. et al. Contemporary epidemiology and prognosis of health care-associated infective endocarditis. Clin. Infect. Dis. 47, 1287–1297 (2008).
Letaief, A. et al. Epidemiology of infective endocarditis in Tunisia: a 10-year multicenter retrospective study. Int. J. Infect. Dis. 11, 430–433 (2007).
Mirabel, M. et al. Infective endocarditis in the Lao PDR: clinical characteristics and outcomes in a developing country. Int. J. Cardiol. 180, 270–273 (2015).
GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age–sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 385, 117–171 (2015).
Veloso, T. R. et al. Induction of experimental endocarditis by continuous low-grade bacteremia mimicking spontaneous bacteremia in humans. Infect. Immun. 79, 2006–2011 (2011).
Moreillon, P. & Que, Y. A. Infective endocarditis. Lancet 363, 139–149 (2004).
Werdan, K. et al. Mechanisms of infective endocarditis: pathogen-host interaction and risk states. Nat. Rev. Cardiol. 11, 35–50 (2014).
Iung, B. et al. Determinants of cerebral lesions in endocarditis on systematic cerebral magnetic resonance imaging: a prospective study. Stroke 44, 3056–3062 (2013).
Rizzi, M. et al. Predicting the occurrence of embolic events: an analysis of 1456 episodes of infective endocarditis from the Italian Study on Endocarditis (SEI). BMC Infect. Dis. 14, 230 (2014).
Stout, K. K. & Verrier, E. D. Acute valvular regurgitation. Circulation 11, 3232–3241 (2009).
Wang, A. et al. Contemporary clinical profile and outcome of prosthetic valve endocarditis. JAMA 297, 1354–1361 (2007). This is an assessment of the presentation and prognosis of IE on prosthetic valves, as compared with IE on native valves, in a large international cohort.
Kannoth, S. & Thomas, S. V. Intracranial microbial aneurysm (infectious aneurysm): current options for diagnosis and management. Neurocrit. Care 11, 120–129 (2009).
Raoult, D. et al. Contribution of systematic serological testing in diagnosis of infective endocarditis. J. Clin. Microbiol. 43, 5238–5242 (2005).
Millar, B. C., Habib, G. & Moore, J. E. New diagnostic approaches in infective endocarditis. Heart 102, 796–807 (2016).
Habib, G. et al. 2015 ESC Guidelines for the management of infective endocarditis: the Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 36, 3075–3128 (2015). This is the latest European guidelines addressing the prevention, diagnosis and management of IE.
Fournier, P. E. et al. Blood culture-negative endocarditis: improving the diagnostic yield using new diagnostic tools. Medicine 96, e8392 (2017).
Bruun, N. E., Habib, G., Thuny, F. & Sogaard, P. Cardiac imaging in infectious endocarditis. Eur. Heart J. 35, 624–632 (2014).
Iung, B., Rouzet, F., Brochet, E. & Duval, X. Cardiac imaging of infective endocarditis, echo and beyond. Curr. Infect. Dis. Rep. 19, 8 (2017).
Baumgartner, F. J. et al. Annular abcesses in surgical endocarditis: anatomic, clinical, and operative features. Ann. Thorac. Surg. 70, 442–447 (2000).
Lancellotti, P. et al. Recommendations for the echocardiographic assessment of native valvular regurgitation: an executive summary from the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 14, 611–644 (2013).
Lindner, J. R. et al. Diagnostic value of echocardiography in suspected endocarditis. An evaluation based on the pretest probability of disease. Circulation 93, 730–736 (1996).
Di Salvo, G. et al. Echocardiography predicts embolic events in infective endocarditis. J. Am. Coll. Cardiol. 37, 1069–1076 (2001).
Fagman, E. et al. ECG-gated computed tomography: a new role for patients with suspected aortic prosthetic valve endocarditis. Eur. Radiol. 22, 2407–2414 (2012).
Feuchtner, G. M. et al. Multislice computed tomography in infective endocarditis: comparison with transesophageal echocardiography and intraoperative findings. J. Am. Coll. Cardiol. 53, 436–444 (2009).
Duval, X. et al. Effect of early cerebral magnetic resonance imaging on clinical decisions in infective endocarditis. A prospective study. Ann. Intern. Med. 152, 497–504 (2010).
Mathieu, C. et al. Characterization of 18F-Fluorodeoxyglucose uptake pattern in noninfected prosthetic heart valves. Circ. Cardiovasc. Imaging 10, e005585 (2017).
Saby, L. et al. Positron emission tomography/computed tomography for diagnosis of prosthetic valve endocarditis: increased valvular 18F-fluorodeoxyglucose uptake as a novel major criterion. J. Am. Coll. Cardiol. 61, 2374–2382 (2013).
Pizzi, M. N. et al. Improving the diagnosis of infective endocarditis in prosthetic valves and intracardiac devices with 18F-fluordeoxyglucose positron emission tomography/computed tomography angiography: initial results at an infective endocarditis referral center. Circulation 132, 1113–1126 (2015).
Ricciardi, A. et al. 18-Fluoro-2-deoxyglucose positron emission tomography-computed tomography: an additional tool in the diagnosis of prosthetic valve endocarditis. Int. J. Infect. Dis. 28, 219–224 (2014).
García-Arribas, D. et al. Usefulness of positron emission tomography/computed tomography in patients with valve-tube graft infection. Heart 104, 1447–1454 (2018).
Swart, L. E. et al. Improving the diagnostic performance of 18F-FDG PET/CT in prosthetic heart valve endocarditis. Circulation 138, 1412–1427 (2018).
Granados, U. Diagnostic accuracy of 18F-FDG PET/CT in infective endocarditis and implantable cardiac electronic device infection: a cross-sectional study. J. Nucl. Med. 57, 1726–1732 (2016).
Mikail, N. et al. Detection of mycotic aneurysms of lower limbs by whole-body (18)F-FDG-PET. JACC Cardiovasc. Imaging 8, 859–862 (2015).
Rouzet, F. et al. Respective performance of 18F-FDG PET and radiolabeled leukocyte scintigraphy for the diagnosis of prosthetic valve endocarditis. J. Nucl. Med. 55, 1980–1985 (2014). This is an evaluation of the diagnostic performance of the two nuclear medicine techniques used in IE.
Erba, P. A. et al. Radiolabeled WBC scintigraphy in the diagnostic workup of patients with suspected device-related infections. JACC Cardiovasc. Imaging 6, 1075–1086 (2013).
Li, J. S. et al. Proposed modifications to the Duke criteria for the diagnosis of infective endocarditis. Clin. Infect. Dis. 30, 633–638 (2000).
Habib, G. et al. Value and limitations of the Duke criteria for the diagnosis of infective endocarditis. J. Am. Coll. Cardiol. 33, 2023–2029 (1999).
Baddour, L. M. et al. Infective endocarditis in adults: diagnosis, antimicrobial therapy, and management of complications: a scientific statement for healthcare professionals from the American Heart Association. Circulation 132, 1435–1486 (2015). This paper presents the latest US guidelines addressing all aspects of the diagnosis and management of IE.
Abdallah, L. et al. Long-term prognosis of left-sided native-valve Staphylococcus aureus endocarditis. Arch. Cardiovasc. Dis. 109, 260–267 (2016).
Abdallah, L. et al. Comparison of prognoses of Staphylococcus aureus left-sided prosthetic endocarditis and prosthetic endocarditis caused by other pathogens. Arch. Cardiovasc. Dis. 109, 542–549 (2016).
Kiefer, T. et al. Association between valvular surgery and mortality among patients with infective endocarditis complicated by heart failure. JAMA 306, 2239–2247 (2011).
Graupner, C. et al. Periannular extension of infective endocarditis. J. Am. Coll. Cardiol. 39, 1204–1211 (2002).
Lopez, J. et al. Prognostic role of persistent positive blood cultures after initiation of antibiotic therapy in left-sided infective endocarditis. Eur. Heart J. 34, 1749–1754 (2013).
Thuny, F. et al. Risk of embolism and death in infective endocarditis: prognostic value of echocardiography: a prospective multicenter study. Circulation 112, 69–75 (2005). This is the largest series on the risk of embolism in IE.
Thuny, F. et al. Impact of cerebrovascular complications on mortality and neurologic outcome during infective endocarditis: a prospective multicentre study. Eur. Heart J. 28, 1155–1161 (2007).
Snygg-Martin, U. et al. Cerebrovascular complications in patients with left-sided infective endocarditis are common: a prospective study using magnetic resonance imaging and neurochemical brain damage markers. Clin. Infect. Dis. 47, 23–30 (2008).
Cooper, H. A. et al. Subclinical brain embolization in left-sided infective endocarditis: results from the evaluation by MRI of the brains of patients with left-sided intracardiac solid masses (EMBOLISM) pilot study. Circulation 120, 585–591 (2009).
Iung, B. et al. Respective effects of early cerebral and abdominal magnetic resonance imaging on clinical decisions in infective endocarditis. Eur. Heart J. Cardiovasc. Imaging 13, 703–710 (2012).
Selton-Suty, C. et al. Symptomatic and asymptomatic neurological complications of infective endocarditis: impact on surgical management and prognosis. PLOS ONE 11, e0158522 (2016).
Dickerman, S. A. et al. The relationship between the initiation of antimicrobial therapy and the incidence of stroke in infective endocarditis: an analysis from the ICE Prospective Cohort Study (ICE-PCS). Am. Heart J. 154, 1086–1094 (2007).
Hubert, S. et al. Prediction of symptomatic embolism in infective endocarditis: construction and validation of a risk calculator in a multicenter cohort. J. Am. Coll. Cardiol. 62, 1384–1392 (2013).
Garcia-Cabrera, E. et al. Neurological complications of infective endocarditis: risk factors, outcome, and impact of cardiac surgery: a multicenter observational study. Circulation 127, 2272–2284 (2013). This is the largest series on the characteristics and prognostic implications of neurological complications of IE.
Goulenok, T. et al. Infective endocarditis with symptomatic cerebral complications: contribution of cerebral magnetic resonance imaging. Cerebrovasc. Dis. 35, 327–336 (2013).
Yoshioka, D. et al. Valve surgery in active endocarditis patients complicated by intracranial haemorrhage: the influence of the timing of surgery on neurological outcomes. Eur. J. Cardiothorac. Surg. 45, 1082–1088 (2014).
Salaun, E. et al. Intracranial haemorrhage in infective endocarditis. Arch. Cardiovasc. Dis. 111, 712–721 (2018).
Hui, F. K. et al. Mycotic aneurysm detection rates with cerebral angiography in patients with infective endocarditis. J. Neurointerv. Surg. 7, 449–452 (2015).
Colen, T. W., Gunn, M., Cook, E. & Dubinsky, T. Radiologic manifestations of extracardiac complications of infective endocarditis. Eur. Radiol. 18, 2433–2244 (2008).
Ostergaard, L. et al. Incidence and factors associated with infective endocarditis in patients undergoing left-sided heart valve replacement. Eur. Heart J. 39, 2668–2675 (2018).
Amat-Santos, I. J. et al. Infective endocarditis after transcatheter aortic valve implantation: results from a large multicenter registry. Circulation 131, 1566–1574 (2015).
Salaun, E. et al. Diagnosis of infective endocarditis after TAVR: value of a multimodality imaging approach. JACC Cardiovasc. Imaging 11, 143–146 (2018).
Oliver, L. et al. Infective endocarditis in octogenarians. Heart 103, 1602–1609 (2017).
Lopez, J. et al. Definition, clinical profile, microbiological spectrum, and prognostic factors of early-onset prosthetic valve endocarditis. Eur. Heart J. 28, 760–765 (2007).
Lalani, T. et al. In-hospital and 1-year mortality in patients undergoing early surgery for prosthetic valve endocarditis. JAMA Intern. Med. 173, 1495–1504 (2013).
Athan, E. et al. Clinical characteristics and outcome of infective endocarditis involving implantable cardiac devices. JAMA 307, 1727–1735 (2012). This is an assessment of the presentation and prognosis of IE on CIEDs in a large international cohort.
Da Costa, A. et al. Role of the preaxillary flora in pacemaker infections: a prospective study. Circulation 97, 1791–1795 (1998).
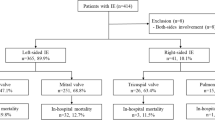
Polewczyk, A., Jachec, W., Janion, M., Podlaski, R. & Kutarski, A. Lead-dependent infective endocarditis: the role of factors predisposing to its development in an analysis of 414 clinical cases. Pacing Clin. Electrophysiol. 38, 846–856 (2015).
Klug, D. et al. Risk factors related to infections of implanted pacemakers and cardioverter-defibrillators: results of a large prospective study. Circulation 116, 1349–1355 (2007).
Dundar, C. et al. The prevalence of echocardiographic accretions on the leads of patients with permanent pacemakers. J. Am. Soc. Echocardiogr. 24, 803–807 (2011).
Jiménez-Ballvé, A. et al. Assessment of the diagnostic accuracy of 18F-FDG PET/CT in prosthetic infective endocarditis and cardiac implantable electronic device infection: comparison of different interpretation criteria. Eur. J. Nucl. Med. Mol. Imaging 43, 2401–2412 (2016).
Del Rio, A. et al. Surgical treatment of pacemaker and defibrillator lead endocarditis: the impact of electrode lead extraction on outcome. Chest 124, 1451–1459 (2003).
Kusumoto, F. M. et al. 2017 HRS expert consensus statement on cardiovascular implantable electronic device lead management and extraction. Heart Rhythm. 14, e503–e551 (2017).
Clementy, N. et al. Infections and associated costs following cardiovascular implantable electronic device implantations. Europace 20, 1974–1980 (2018).
Miro, J. M. et al. Infective endocarditis in intravenous drug abusers and HIV-1 infected patients. Infect. Dis. Clin. North. Am. 16, 273–295 (2002).
San Roman, J. A. et al. Role of transthoracic and transesophageal echocardiography in right-sided endocarditis: one echocardiographic modality does not fit all. J. Am. Soc. Echocardiogr. 25, 807–814 (2012).
Showler, A. et al. Use of transthoracic echocardiography in the management of low-risk Staphylococcus aureus bacteremia: results from a retrospective multicenter cohort study. JACC Cardiovasc. Imaging 8, 924–931 (2015).
Tubiana, S. et al. The VIRSTA score, a prediction score to estimate risk of infective endocarditis and determine priority for echocardiography in patients with Staphylococcus aureus bacteremia. J. Infect. 72, 544–553 (2016).
Dahl, A. et al. Risk factors of endocarditis in patients with Enterococcus faecalis bacteremia: external validation of the NOVA score. Clin. Infect. Dis. 63, 771–775 (2016).
Sunnerhagen, T. et al. HANDOC: a handy score to determine the need for echocardiography in non-β-hemolytic streptococcal bacteremia. Clin. Infect. Dis. 10, 693–698 (2018).
Mirabel, M. et al. Long-term outcomes and cardiac surgery in critically ill patients with infective endocarditis. Eur. Heart J. 35, 1195–1204 (2014).
Gelsomino, S. et al. Emergency surgery for native mitral valve endocarditis: the impact of septic and cardiogenic shock. Ann. Thorac. Surg. 93, 1469–1476 (2012).
Pajaron, M. et al. Self-administered outpatient parenteral antimicrobial therapy (S-OPAT) for infective endocarditis: a safe and effective model. Eur. J. Intern. Med. 26, 131–136 (2015).
Mzabi, A. et al. Switch to oral antibiotics in the treatment of infective endocarditis is not associated with increased risk of mortality in non-severely ill patients. Clin. Microbiol. Infect. 22, 607–612 (2016).
Pericas, J. M. et al. Outpatient parenteral antibiotic treatment (OPAT) for infective endocarditis: a prospective cohort study from the GAMES cohort. Clin. Infect. Dis. https://doi.org/10.1093/cid/ciz030 (2019).
Iversen, K. et al. Partial oral versus intravenous antibiotic treatment of endocarditis. N. Engl. J. Med. 380, 415–424 (2019). This is the first randomized trial validating the use of oral antibiotic therapy in selected patients with IE.
Chan, K. L. et al. A randomized trial of aspirin on the risk of embolic events in patients with infective endocarditis. J. Am. Coll. Cardiol. 42, 775–780 (2003).
de Kerchove, L. et al. Reconstructive surgery in active mitral valve endocarditis: feasibility, safety and durability. Eur. J. Cardiothorac. Surg. 31, 592–599 (2007).
de Kerchove, L. et al. Extending the scope of mitral valve repair in active endocarditis. J. Thorac. Cardiovasc. Surg. 143, S91–S95 (2012).
David, T. E. Aortic valve repair for active infective endocarditis. Eur. J. Cardiothorac. Surg. 42, 127–128 (2012).
Perrotta, S., Jeppsson, A., Freojd, V. & Svensson, G. Surgical treatment of aortic prosthetic valve endocarditis: a 20-year single-center experience. Ann. Thorac. Surg. 101, 1426–1432 (2016).
Kim, J. B. et al. Are homografts superior to conventional prosthetic valves in the setting of infective endocarditis involving the aortic valve? J. Thorac. Cardiovasc. Surg. 151, 1239–1246 (2016).
Kirklin, J. K. Challenging homografts as the holy grail for aortic valve endocarditis. J. Thorac. Cardiovasc. Surg. 15, 1230–1231 (2016).
Nappi, F., Spadaccio, C. & Acar, C. Use of allogeneic tissue to treat infective valvular disease: Has everything been said? J. Thorac. Cardiovasc. Surg. 153, 824–828 (2017).
Chirouze, C. et al. ICE Prospective Investigators. Impact of early valve surgery on outcome of Staphylococcus aureus prosthetic valve infective endocarditis: analysis in the International Collaboration of Endocarditis-Prospective Cohort Study. Clin. Infect. Dis. 60, 741–749 (2015).
Kang, D. H. et al. Early surgery versus conventional treatment for infective endocarditis. N. Engl. J. Med. 366, 2466–2473 (2012). This is a randomized trial supporting early surgery in patients with large vegetations and severe regurgitation without other indications for surgery.
Delahaye, F. Is early surgery beneficial in infective endocarditis? A systematic review. Arch. Cardiovasc. Dis. 104, 35–44 (2011).
Narayanan, M. A. et al. Early versus late surgical intervention or medical management for infective endocarditis: a systematic review and meta-analysis. Heart 102, 950–957 (2016).
Bannay, A. et al. The impact of valve surgery on short- and long-term mortality in left-sided infective endocarditis: do differences in methodological approaches explain previous conflicting results? Eur. Heart J. 32, 2003–2015 (2011). This is an in-depth analysis of the association between surgery and mortality in IE considering sources of methodological bias.
Thuny, F. et al. The timing of surgery influences mortality and morbidity in adults with severe complicated infective endocarditis: a propensity analysis. Eur. Heart J. 32, 2027–2033 (2011).
Chu, V. H. et al. Association between surgical indications, operative risk, and clinical outcome in infective endocarditis: a prospective study from the International Collaboration on Endocarditis. Circulation 131, 131–140 (2015).
Iung, B. et al. Cardiac surgery during the acute phase of infective endocarditis: discrepancies between European Society of Cardiology guidelines and practices. Eur. Heart J. 37, 840–848 (2016).
Madeira, S. et al. Assessment of perioperative mortality risk in patients with infective endocarditis undergoing cardiac surgery: performance of the EuroSCORE I and II logistic models. Interact. Cardiovasc. Thorac. Surg. 22, 141–148 (2016).
Patrat-Delon, S. et al. EuroSCORE II underestimates mortality after cardiac surgery for infective endocarditis. Eur. J. Cardiothorac. Surg. 49, 944–951 (2016).
De Feo, M. et al. The need for a specific risk prediction system in native valve infective endocarditis surgery. Sci. World J. 2012, 307571 (2012).
Martınez-Selles, M. et al. Valve surgery in active infective endocarditis: a simple score to predict inhospital prognosis. Int. J. Cardiol. 175, 133–137 (2014).
Gaca, J. G. et al. Outcomes for endocarditis surgery in North America: a simplified risk scoring system. J. Thorac. Cardiovasc. Surg. 141, 98–106 (2011).
Di Mauro, M. et al. A predictive model for early mortality after surgical treatment of heart valve or prosthesis infective endocarditis. The EndoSCORE. Int. J. Cardiol. 241, 97–102 (2017).
Gatti, G. et al. Simple scoring system to predict in-hospital mortality after surgery for infective endocarditis. J. Am. Heart Assoc. 6, e004806 (2017).
Olmos, C. et al. Risk score for cardiac surgery in active left-sided infective endocarditis. Heart 103, 1435–1442 (2017).
Durack, D. T. Prevention of infective endocarditis. N. Engl. J. Med. 332, 38–44 (1995).
Agha, Z., Lofgren, R. P. & Van Ruiswyk, J. V. Is antibiotic prophylaxis for bacterial endocarditis cost-effective? Med. Decis. Making 25, 308–320 (2005).
Franklin, M. et al. The cost-effectiveness of antibiotic prophylaxis for patients at risk of infective endocarditis. Circulation 134, 1568–1578 (2016).
Devereux, R. B., Frary, C. J., Kramer-Fox, R., Roberts, R. B. & Ruchlin, H. S. Cost-effectiveness of infective endocarditis prophylaxis for mitral valve prolapse with or without a mitral regurgitant murmur. Am. J. Cardiol. 74, 1024–1029 (1994).
Gould, I. M. & Buckingham, J. K. Cost effectiveness of prophylaxis in dental practice to prevent infective endocarditis. Br. Heart. J. 70, 79–83 (1993).
Tubiana, S. et al. Dental procedures, antibiotic prophylaxis, and endocarditis among people with prosthetic heart valves: nationwide population based cohort and a case crossover study. BMJ 358, j3776 (2017). This is the largest analysis of the relationship between dental procedures and IE using data from a nationwide database.
Duval, X. et al. Estimated risk of endocarditis in adults with predisposing cardiac conditions undergoing dental procedures with or without antibiotic prophylaxis. Clin. Infect. Dis. 42, e102–e107 (2006).
Wilson, W. et al. Prevention of infective endocarditis: guidelines from the American Heart Association: a guideline from the American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee, Council on Cardiovascular Disease in the Young, and the Council on Clinical Cardiology, Council on Cardiovascular Surgery and Anesthesia, and the Quality of Care and Outcomes Research Interdisciplinary Working Group. Circulation 116, 1736–1754 (2007).
Habib, G. et al. Guidelines on the prevention, diagnosis, and treatment of infective endocarditis: the Task Force on the Prevention, Diagnosis, and Treatment of Infective Endocarditis of the European Society of Cardiology (ESC). Eur. Heart J. 30, 2369–2413 (2009).
Stokes, T., Richey, R., Wray, D. & Wrayon, D. Prophylaxis against infective endocarditis: summary of NICE guidance. Heart 94, 930–931 (2008).
Duval, X. et al. Temporal trends in infective endocarditis in the context of prophylaxis guideline modifications: three successive population-based surveys. J. Am. Coll. Cardiol. 59, 1968–1976 (2012).
DeSimone, D. C. et al. Incidence of infective endocarditis caused by viridans group streptococci before and after publication of the 2007 American Heart Association’s endocarditis prevention guidelines. Circulation 126, 60–64 (2012).
DeSimone, D. C. et al. Incidence of infective endocarditis due to viridans group Streptococci before and after the 2007 American Heart Association’s Prevention Guidelines: an extended evaluation of the Olmsted County, Minnesota, population and nationwide inpatient sample. Mayo Clin. Proc. 90, 874–881 (2015).
DeSimone, D. C. et al. Temporal trends in infective endocarditis epidemiology from 2007 to 2013 in Olmsted County, MN. Am. Heart. J. 170, 830–836 (2015).
Pant, S. et al. Trends in infective endocarditis incidence, microbiology, and valve replacement in the United States from 2000 to 2011. J. Am. Coll. Cardiol. 65, 2070–2076 (2015).
Pericas, J. M. et al. Neglecting enterococci may lead to a misinterpretation of the consequences of last changes in endocarditis prophylaxis American Heart Association guidelines. J. Am. Coll. Cardiol. 66, 2156 (2015).
Dayer, M. J. et al. Incidence of infective endocarditis in England, 2000-13: a secular trend, interrupted time-series analysis. Lancet 385, 1219–1228 (2015).
Iung, B., Tubiana, S., Alla, F. & Lavielle, M. Infective endocarditis and antibiotic prophylaxis. Lancet 386, 529–530 (2015).
Mackie, A. S., Liu, W., Savu, A., Marelli, A. J. & Kaul, P. Infective endocarditis hospitalizations before and after the 2007 American Heart Association Prophylaxis Guidelines. Can. J. Cardiol. 32, 942–948 (2016).
van den Brink, F. S. et al. Increased incidence of infective endocarditis after the 2009 European Society of Cardiology guideline update: a nationwide study in the Netherlands. Eur. Heart J. Qual. Care Clin. Outcomes 3, 141–147 (2017).
Petersen, P. E., Bourgeois, D., Ogawa, H., Estupinan-Day, S. & Ndiaye, C. The global burden of oral diseases and risks to oral health. Bull. World Health Organ. 83, 661–669 (2005).
Lockhart, P. B. et al. Poor oral hygiene as a risk factor for infective endocarditis-related bacteremia. J. Am. Dent. Assoc. 140, 1238–1244 (2009).
Duval, X. et al. Oral streptococcal endocarditis, oral hygiene habits and recent dental procedures: a case-control study. Clin. Infect. Dis. 64, 1678–1685 (2017).
Millot, S. et al. Position paper for the evaluation and management of oral status in patients with valvular disease: Groupe de Travail Valvulopathies de la Société Française de Cardiologie, Société Française de Chirurgie Orale, Société Française de Parodontologie et d’Implantologie Orale, Société Française d’Endodontie et Société de Pathologie Infectieuse de Langue Française. Arch. Cardiovasc. Dis. 110, 482–494 (2017).
Hoen, B. et al. Tumors of the colon increase the risk of developing Streptococcus bovis endocarditis: case-control study [letter]. Clin. Infect. Dis. 19, 361–362 (1994).
Pericas, J. M. et al. Relationship between Enterococcus faecalis infective endocarditis and colorectal neoplasm: preliminary results from a cohort of 154 patients. Rev. Esp. Cardiol. 70, 451–458 (2017).
Sandoe, J. A. et al. Guidelines for the diagnosis, prevention and management of implantable cardiac electronic device infection. Report of a joint Working Party project on behalf of the British Society for Antimicrobial Chemotherapy (BSAC, host organization), British Heart Rhythm Society (BHRS), British Cardiovascular Society (BCS), British Heart Valve Society (BHVS) and British Society for Echocardiography (BSE). J. Antimicrob. Chemother. 70, 325–359 (2015).
Baddour, L. M., Cha, Y. M. & Wilson, W. R. Infections of cardiovascular implantable electronic devices. N. Engl. J. Med. 367, 842–849 (2012).
Fowler, V. G. et al. Effect of an investigational vaccine for preventing Staphylococcus aureus infections after cardiothoracic surgery: a randomized trial. JAMA 309, 1368–1378 (2013).
Veloso, T. R. et al. Prophylaxis of experimental endocarditis with antiplatelet and antithrombin agents: a role for long-term prevention of infective endocarditis in humans? J. Infect. Dis. 211, 72–79 (2015).
Veloso, T. R. et al. Aspirin plus ticlopidine prevented experimental endocarditis due to Enterococcus faecalis and Streptococcus gallolyticus. Pathog. Dis. 73, ftv060 (2015).
Mestres, C. A. et al. Organization and functioning of a multidisciplinary team for the diagnosis and treatment of infective endocarditis: a 30-year perspective (1985–2014). Rev. Esp. Cardiol. 68, 363–368 (2015).
Hoen, B. & Duval, X. Infective endocarditis. N. Engl. J. Med. 368, 1425–1433 (2013).
Acknowledgements
Review criteria
The PubMed database was searched to select articles for inclusion in this Review using the search terms “infective endocarditis” alone and combined with “epidemiology”, “pathophysiology”, “imaging”, “valvular surgery”, “transcatheter valves”, “prophylaxis” and “guidelines”. Only full-text papers in the English language were considered, and original papers were favoured over reviews. The authors selected papers published between 1990 and 2018. Reference lists of identified papers were searched for further leads, favouring papers published after 2010.
Author information
Authors and Affiliations
Contributions
Both authors contributed to researching data for the article, discussion of content, writing and reviewing and/or editing the manuscript before submission.
Corresponding author
Ethics declarations
Competing interests
B.I. has received consultant fees from Edwards Lifesciences and speaker’s fees from Boehringer Ingelheim and Novartis. X.D. has received a grant from Pfizer.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
41569_2019_215_MOESM1_ESM.avi
Supplementary Video 1 Infective endocarditis on a rheumatic mitral valve with moderate stenosis. Large (18 mm) and very mobile vegetation inserted on the atrial side of the mitral valve with intermittent prolapse in the left ventricle during the diastole. Transthoracic echocardiography, parasternal long-axis view.
41569_2019_215_MOESM2_ESM.avi
Supplementary Video 2 Infective endocarditis on a bicuspid aortic valve. Vegetations on both leaflets, partial prolapse of the anterior leaflet and lack of coaptation due to valve mutilation (left panel). The consequence is a severe aortic regurgitation with a large jet according to colour Doppler (right panel). Transoesophageal echocardiography.
41569_2019_215_MOESM3_ESM.avi
Supplementary Video 3 Infective endocarditis on an aortic bioprosthesis. Periprosthetic posterior abscess fistulised in the aorta and the left ventricle causing severe aortic regurgitation according to colour Doppler. Transthoracic echocardiography, parasternal long-axis (left panel) and short-axis (right panel) views.
41569_2019_215_MOESM4_ESM.avi
Supplementary Video 4 Infective endocarditis on an aortic bioprosthesis. Periprosthetic posterior abscess fistulised in the aorta and the left ventricle causing severe aortic regurgitation according to colour Doppler. Transthoracic echocardiography, apical 2 chamber view.
41569_2019_215_MOESM5_ESM.avi
Supplementary Video 5 Infective endocarditis on an aortic bioprosthesis. Periprosthetic posterior abscess at the upper part of the prosthesis, fistulised in the aorta and the left ventricle. Transoesophageal echocardiography, long-axis view.
41569_2019_215_MOESM6_ESM.avi
Supplementary Video 6 Infective endocarditis on an aortic bioprosthesis. Periprosthetic posterior abscess at the upper part of the prosthesis, fistulised in the aorta and the left ventricle causing severe aortic regurgitation according to colour Doppler. Transoesophageal echocardiography, long-axis (left panel) and short-axis (right panel) views.
41569_2019_215_MOESM7_ESM.avi
Supplementary Video 7 Infective endocarditis on an aortic bioprosthesis. Perivalvular abscess at the upper part of the aortic prosthesis with systolic expansion. 3D transoesophageal echocardiography, short-axis views.
Rights and permissions
About this article

Cite this article
Iung, B., Duval, X. Infective endocarditis: innovations in the management of an old disease. Nat Rev Cardiol 16, 623–635 (2019). https://doi.org/10.1038/s41569-019-0215-0
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41569-019-0215-0
This article is cited by
-
Real world experience of therapeutic monitoring of medically treated prosthetic valve infective endocarditis by 18F-FDG-PET/CT
Journal of Nuclear Cardiology (2023)
-
ASSESS-IE: a Novel Risk Score for Patients with Infective Endocarditis
Journal of Cardiovascular Translational Research (2023)
-
The clinical pattern differentiates ANCA-positive infective endocarditis patients from ANCA-associated vasculitis patients: a 23 years’ retrospective cohort study in China and follow-ups
Clinical Rheumatology (2022)
-
Clinical and Microbiological Characteristics of Infective Endocarditis at a Cardiac Center in Saudi Arabia
Journal of Epidemiology and Global Health (2021)
