
Abstract
Study design
Animal proof of principle study.
Objectives
To investigate neurodegeneration in rabbit L4-dorsal root ganglion (DRG) cells by creating experimental spinal subarachnoid hemorrhage (SAH), we aimed to show the neuronal pathway between L4-DRG and femoral artery.
Setting
Ataturk University, Medical Faculty, Animal Laboratory, Erzurum, Turkey.
Methods
This study was designed on 20 rabbits, which were randomly divided into three groups: Spinal SAH (n = 8), SHAM (n = 6), and control (n = 6) groups. Animals were followed for 20 days and then killed. Vasospasm index values of the femoral artery and neuron density of L4-DRG were analyzed.
Results
The number of degenerated neurons in DRG was higher in the spinal SAH than the control and SHAM groups (p < 0.001). But, the difference between the control group and the SHAM group was not significant. Normal neuron densities were significantly lower in the spine SAH group compared to the SHAM and the control groups. There was a statistically significant increase in vasospasm index values of the spinal SAH group compared to the other two groups (p < 0.001).
Conclusions
Decreased volume of the femoral artery lumen was showed in animals with spinal SAH compared with control and SHAM groups. Increased degeneration of the L4 dorsal root ganglion in animals with spinal SAH was also demonstrated. Our findings might shed light on the planning of future experimental studies and evaluating the clinical relevance of such studies.
Similar content being viewed by others


Introduction
Subarachnoid hemorrhage can occur either spontaneously or due to trauma [1]. This is a destructive pathology [2]. Vasospasm following SAH is still a major cause of mortality and morbidity [3]. More than one-third of SAH patients develop clinically significant vasospasm. Therefore, the mechanisms of vasospasm remain important. The vasospasm of the Adamkiewicz artery (AKA) due to spinal SAH has been reported to carry a risk of developing ischemic spinal cord dysfunction in an animal model [4]. According to, the histopathological changes in dorsal root ganglion (DRG) after spinal SAH were reported by different authors [4,5,6]. Onder et al. [6] demonstrated that bloody and high-protein cerebrospinal fluid (CSF) led to neural degeneration. Kanat et al. [7] reported that vasospasm of the anterior spinal artery after spinal SAH affects the sensory pathways and could cause degeneration in DRG neurons.
Kayacı et al. [8] showed that after spinal SAH, the relationship between cervical sixth DRG degeneration and brachial artery vasospasm. Xing et al. [9] reported that femoral artery occlusion is created by the cell patch-clamp method, it has been shown that degeneration of the afferent L4-DRG neurons and, following lower extremity vascular insufficiency. These studies show us that a change in DRGs cause femoral artery vasospasm or vice versa. It is suggested that there is contact between L4-neuron cells and femoral arteries through a nerve pathway containing afferent and efferent fibers or chemical mediators.
In this study, experimental spinal SAH was performed to induce neurodegeneration in L4-DRG cells of rabbits. All sacral spinal cord and sacral parasympathetics are affected. L4 has the most active role in the parasympathetic activity of the femoral arteries in the rough sacral inner plexus. It focuses on the upper L4 root.
Methods
This study was designed on 20 adult male New Zealand rabbits (3.6 ± 0.5 kg) (Ataturk University, Erzurum, Turkey) that were haphazardly split into three groups: control (n = 6), SHAM (n = 6), and spinal SAH (n = 8). The animal protocols were approved (Date: 26.07.2018, Decision number: 163, Meeting number: 8) by the Ethics Committee of Ataturk University, Medical Faculty.
Animals were anesthetized by subcutaneous injection of a mixture of ketamine hydrochloride (25 mg/kg), lidocaine hydrochloride (15 mg/kg), and acepromazine (1 mg/kg). Computed tomography was used to define L2–L3 levels. After the surgical site was shaved and sterilized, a skin incision was made, then the paravertebral muscles were dissected, and the L2 laminotomy was performed using a Midas Rex high-speed drill (Medtronic Midas Rex, Fort Worth, Texas, USA). Autologous blood (0.5 mL) obtained from the auricular artery was applied using a 22-Gauge needle into the subarachnoid space at the L2–L3 level in the SAH group of rabbits over the course of 1 min. In the SHAM group, 0.5 mL saline was administered to the subarachnoid space at the L2–L3 level. This procedure was not applied to the animals in the control group. All animals were followed for 20 days and then killed.
Tissue processing
Their lumbar DRGs at the left L4 level was removed. Femoral artery (left extremity), just proximal of the bifurcation of the deep and superficial, and left L4 DRG were assessed histopathologically after staining with hematoxylin–eosin (H&E) and tunel. Sections from the left femoral artery and left DRG, which were cut into small blocks and placed in fresh fixative, were stored in 10% formaldehyde at 4 °C for 7 days. The fixed tissues were then passed through graded ethyl alcohol series to be dehydrated and embedded in paraffin. Sections of 5 µm thickness were taken with a rotary microtome and collected on glass slides for histopathological and stereological analysis. The sections were analyzed morphologically using H&E and tunel staining, via light microscopy. Neuronal shrinkage, perinuclear halo formation, cytoplasmic condensation, cellular angulation, and neuronal loss were accepted as ganglionary degeneration criteria.
Stereological analyses of histological findings were investigated according to the principles of the study performed by Turkmenoglu et al. [4].
The vasospasm index calculations of Ozturk et al. were made taking into account [5] (Fig. 1).

A Normal in the control group. B Moderately constructed in the SHAM group and, (C) the severely constructed femoral artery with a convoluted inner elastic membrane, degenerated muscles (DM), and endothelin in the narrowed lumen (NL) in a SAH-created rabbit (LM, H&E, ×4).
Stereological analysis
The physical disector method was applied to interpret the number of neurons in a DRG. Data were obtained from pairs of dissectors made of parallel cuttings taken at known times. The mean numerical density of ganglia neurons (NvGN) per mm3 was determined using the formula.
where ΣQN is the total number of counting neurons appearing only in the reference sections; t is the section thickness; and A is the area of the counting frame. The Cavalieri volume assessment procedure was followed to determine the total number of neurons in each sample. The total number of neurons was determined by multiplying the volume (mm3) and the quantitative density of the neurons in each DRG calculated by stereological methods. Wall surface/lumen surface ratios were considered to calculate the vasospasm index (VSI) values of the femoral artery. The VSI calculation method was made as follows: 2R is the outer diameter of the femoral artery and 2r is the inner diameter. The VSI was calculated as the ratio of the outer surface value to the lumen surface value: (πR2 − πr2)/πr2 = (R2 − r2)/r2.
The VSI was 1 to 1.5 in femoral arteries without vasospasm, 1.5 to 2 with mild vasospasm, and >2 in arteries with severe vasospasm, as stated by Kanat et al. [7].
Statistical methods
L4-DRG numerical densities and femoral artery VSIs of all three groups were evaluated by one-way (ANOVA) analysis and the post hoc Tukey HSD test were used to determine the group making difference. P value < 0.05 was considered significant.
Results
Histological changes
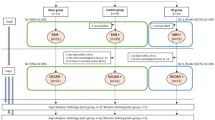
Thin and smooth endothelium, unfolded internal elastic lamina and concentric smooth muscle cells and femoral artery lumen were clearly distinguished in the control group (Fig. 1A). The endothelial cells of the SHAM group had less deterioration than the vasospasm group. Regular internal elastic lamina was also shown in the SHAM group (Fig. 1B). Desquamation and proliferation of endothelial cells into the lumen were shown in the vasospasm group. Internal elastic lamina irregularity was noticed. Concentric smooth muscle cells were also found to be irregular in the SAH group (Fig. 1C/Base).
Histological appearances of the femoral artery in the control group (Fig. 2A). Slight apoptotic changes at the endothelial and muscular cells are shown in the SHAM group (Fig. 2B). Vasospastic inner elastic lamina of the femoral artery, heavy apoptotic changes at the endothelial and muscular cells are seen in the SAH group (Fig. 2C/Base). Histological appearances of DRG in the control group (Fig. 3A), the slight degenerated appearance of the SHAM group (Fig. 3B), the histopathological appearance of degenerated DRG in the SAH group (Fig. 3C/Base).

A Normal in the control group. B Moderately constructed in the SHAM and (C) the severely constructed femoral artery with a convoluted inner elastic membrane, degenerated muscles (DM), and apoptotic endothelin in narrowed lumen (NL) in a SAH-created rabbit (LM, Tunel, ×4).

A Normal in the control group. B SHAM group with moderate neurodegeneration and, (C) severe neurodegeneration (ND) in rabbits induced SAH (LM, H&E, ×4).
Numerical results
We compared the density of the L4 DRG and VSI in all groups and summarized them as mean and standard deviation.
There was no statistically significant difference in the DRG values of the control and SHAM groups, and VSI values between the control and SHAM groups (P > 0.05). However, statistical analysis between of the DRG and VSI values in the control and SAH group were significant (P < 0.001) (Fig. 4).

A Normal neuron density. B Degenerated neuron density. C Vasospasm index of the femoral artery. Spinal SAH induced DRG degeneration and vasospasm of the femoral artery. The results were evaluated by one-way ANOVA analysis and Tukey test post hoc tests. DRG dorsal root ganglion, SAH subarachnoid hemorrhage. *P < 0.05 was considered statistically significant for all results. **p < 0.01; ***p < 0.001.
Discussion
SAH, which causes vasospasm in both cerebral arteries and extra cerebral arteries, is an important complication. The spinal cord affected by spinal SAH is very rare, and can have devastating consequences [4]. Turkmenoglu et al. [4] and Ozturk et al. [5] showed that vasospasm of the AKA following spinal SAH causes spinal ischemia. Therefore, neurodegeneration of the DRG occurs following AKA vasospasm. Acute hypoperfusion of the AKA can give into disastrous ischemic problems, resulting in paraparesis or paraplegia with urinary bladder dysfunction [10]. In addition to, Onder et al. [6] reported that SAH results in bloody CSF, blood or high-protein, can cause neural degeneration. Spinal SAH can also cause vasoconstriction in other extra-spinal arteries. DRG degeneration caused by spinal SAH can lead femoral artery vasospasm [9, 11].
Kanat et al. showed that SAH may cause anterior spinal artery spasm-related spinal cord ischemia [7]. The same mechanism may be responsible for femoral artery spasm.
Onuf’s nucleus sends afferent parasympathetic fibers to the femoral arteries. Karadeniz et al. showed that Onuf’s nucleus ischemia due to sacral parasympathetic ischemia after spinal SAH may be responsible for femoral artery spasm due to parasympathetic insufficiency triggered sympathetic overactivity [12].
In another study, the relationship between Onuf’s parasympathetic nucleus degeneration and sperm count after spinal subarachnoid hemorrhage (SAH) was investigated, and it was shown that Onuf’s nucleus changes may play a role in low sperm count [13].
The DRG is defined between the dorsal root and the spinal nerve [4, 14]. We created the SAH group by applying autologous blood into the L2–3 subarachnoid space, and SHAM group that was injected with saline and compared findings with the control group, that had nothing applied. We found significantly increasing in the degenerated neuron density of DRG in the SAH group, compared with the control and SHAM groups.
Having broad information about anatomy is obligatory for experiencing neurosurgery. Some anatomical structures require detailed study due to their functional importance [4, 15, 16]. One of these structures is the DRG. Some authors have analyzed ganglion and neuronal cell alterations after SAH [5, 6]. DRG are sensitive to ischemia [4, 5]. Kayacı et al. [8] showed that after spinal SAH, the relationship between cervical 6 DRG degeneration and brachial artery vasospasm. Xing et al. [9] reported that femoral artery occlusion is created by the cell patch-clamp method, it has been shown that degeneration of the afferent L4-DRG neurons and, following lower extremity vascular insufficiency.
In our study, we observed severe vasospasm in the femoral artery of rabbits in the SAH group, but not in the SHAM and control groups.
These results suggest that there is a pathway that provides neuronal communication between the DRG and the femoral artery. We think that femoral artery vasospasm caused by DRG degeneration, formed after spinal SAH, might become more destructive, especially in patients with peripheral arterial disease.
Limitations
Animals with small bodily proportions, such as mice and rats, technically, have disadvantages in such experimental studies, however, animals such as rabbits have been shown to be more suitable in spinal SAH studies [16]. Although the relationship between femoral artery vasospasm and DRG degeneration has been demonstrated, motor function testing, somatosensory and motor potentials, hindlimb motility, and long-term follow-up were not performed. We believe this work would inspire pioneer groups.
Conclusions
The development of neurodegeneration after L4 SAH has been demonstrated in this study. SAH induces neurodegeneration by causing vasospasm of the arteries supplying the L4 DRG. Vasospasm of DRG arteries exposed to subarachnoid blood might lead to ischemic neurodegeneration, and a decrease in normal neuron density of DRG may be an important factor in the regulation of the femoral artery accordingly. We have shown the vasospasm and histopathological changes in the femoral artery, and DRG degeneration by forming spinal SAH. With these results, we believe that L4 DRG degeneration caused by spinal SAH might increase femoral arterial insufficiency. In patients with lumbar trauma, the presence of edema and neurogenic claudication in the lower extremities, weakness in the calf muscles, chills, and discoloration of the feet may suggest femoral artery stenosis.
Data availability
Further data, is available from all author.
References
Kim KS, Brophy GM. Symptomatic venous thromboembolism: incidence and risk factors in patients with spontaneous or traumatic intracranial hemorrhage. Neurocrit Care. 2009;11:28–33.
Tuzgen S, Kucukyuruk B, Aydin S, Ozlen F, Kizilkilic O, Abuzayed B, et al. Decompressive craniectomy in patients with cerebral infarction due to malignant vasospasm after aneurysmal subarachnoid hemorrhage. J Neurosci Rural Pract. 2012;3:251–5.
Findlay JM, Nisar J, Darsaut T. Cerebral vasospasm: a review. Can J Neurol Sci. 2016;43:15–32.
Turkmenoglu ON, Kanat A, Yolas C, Aydin MD, Ezirmik N, Gundogdu C, et al. First report of important causal relationship between the Adamkiewicz artery vasospasm and dorsal root ganglion cell degeneration in spinal subarachnoid hemorrhage: An experimental study using a rabbit model. Asian J Neurosurg. 2017;12:22–7.
Ozturk C, Kanat A, Aydin MD, Yolas C, Kabalar ME, Gundogdu B, et al. The impact of L5 dorsal root ganglion degeneration and Adamkiewicz artery vasospasm on descending colon dilatation following spinal subarachnoid hemorrhage: an experimental study; first report. J Craniovertebr Junction Spine. 2015;6:69–75.
Onder A, Serarslan Y, Aydin MD, Kanat A, Gursan N, Yolas C, et al. Spinal arachnoiditis and the axonal degeneration of the spinal nerve roots due to ischemia induced by vasospasm: an experimental study. J Neurol Sci Turk. 2009;26:416–23.
Kanat A, Yilmaz A, Aydin MD, Musluman M, Altas S, Gursan N, et al. Role of degenerated neuron density of dorsal root ganglion on anterior spinal artery vasospasm in subarachnoid hemorrhage: experimental study. Acta Neurochir. 2010;152:2167–72.
Kayacı S, Cakir T, Aydin MD, Kanat A, Omeroglu M, Levent A, et al. Brachial artery vasospasm caused by cervical dorsal root ganglion degeneration after subarachnoid hemorrhage: an experimental study. World Neurosurg. 2019;126:895–900.
Xing J, Lu J, Li J. Augmented P2X response and immunolabeling in dorsal root ganglion neurons innervating skeletal muscle following femoral artery occlusion. J Neurophysiol. 2013;109:2161–8.
Kuipers R, Izhar Z, Gerrits PO, Miner W, Holstege G. Location of bladder and urethral sphincter motoneurons in the male guinea pig (Cavia porcellus). Neurosci Lett. 2004;362:57–60.
Xing J, Li J. TRPA1 function in skeletal muscle sensory neurons following femoral artery occlusion. Cell Physiol Biochem. 2017;42:2307–17.
Karadeniz E, Caglar O, Firinci B, Ahiskalioglu A, Aydin MD, Kocak MN, et al. Predeterminative role of Onuf’s nucleus ischemia on mesenteric artery vasospasm in spinal subarachnoid hemorrhage: A preliminary experimental study. Asian J Surg. 2019;42:797–804.
Caglar O, Firinci B, Aydin ME, Arslan R, Kanat A, Demirci T, et al. First emerging evidence of the relationship between Onuf’s nucleus degeneration and reduced sperm number following spinal subarachnoid haemorrhage: experimental study. Andrologia. 2021;53:e14030.
Ray P, Torck A, Quigley L, Wangzhou A, Neiman M, Rao C, et al. Comparative transcriptome profiling of the human and mouse dorsal root ganglia: an RNA-seq-based resource for pain and sensory neuroscience research. Pain. 2018;159:1325–45.
Kikuchi S, Sato K, Konno S, Hasue M. Anatomic and radiographic study of dorsal root ganglia. Spine. 1994;19:6–11.
Mazensky D, Radonak J, Danko J, Petrovova E, Frankovicova M. Anatomical study of blood supply to the spinal cord in the rabbit. Spinal Cord. 2011;49:525–8.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval
All procedures performed on animals were in accordance with the ethical standards of the Integrated Laboratory Systems animal care and use committees and followed the NIH Guidelines for the Care and Use of Laboratory Animals. We certify that all applicable institutional and governmental regulations concerning the ethical use of animals were followed during the course of this research. This article does not contain any studies with human participants.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Cetin, A., Ozevren, H., Arslan, R. et al. Assessment relationship between the femoral artery vasospasm and dorsal root ganglion cell degeneration in spinal subarachnoid hemorrhage: an experimental study. Spinal Cord 60, 404–407 (2022). https://doi.org/10.1038/s41393-022-00778-x
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-022-00778-x
