
Abstract
Study design
Cross-sectional.
Objectives
(1) Identify changes in employment status and earnings after spinal cord injury (SCI). (2) Estimate annual indirect costs and lifetime indirect costs due to lost earnings for various age and neurologic categories of those with SCI. (3) Compare our estimates with previous research.
Setting
Medical university in southeastern United States.
Methods
A population-based cohort of 307 participants met eligibility criteria of: (1) residual impairment resulting from traumatic SCI, (2) at least 1 year post injury, (3) between 23 and 64 years old at time of injury, (4) <65 years old at time of measurement, and (5) complete information on injury level, injury completeness, employment status, and earnings before and after injury. Main outcomes were employment status and earnings at the time of injury and post injury. Earnings were adjusted for inflation and the value of fringe benefits.
Results
Employment rate decreased from 87% at the time of injury to 35% after injury. Average annual indirect costs were $29,354 in 2019 dollars. Lifetime indirect costs for persons injured at age 25 varied by severity of injury, ranging from 0.5 to 2.3 million dollars. Lifetime indirect costs for persons injured at age 50 ranged from 0.3 to 0.6 million dollars.
Conclusions
Our estimate of indirect costs is lower than the previously estimated number. However, the higher unemployment rate and decreased earnings after SCI still make a heavy economic burden. With improvements in employment outcomes after SCI, the indirect costs affecting individuals, their families, and society can be further reduced.
Similar content being viewed by others

Introduction
Because spinal cord injury (SCI) is mostly associated with high-level permanent losses in sensory and motor functioning, it can lead to a heavy economic burden affecting individuals, their families, and society. Although a primary concern is the direct cost related to medical care, there are also indirect costs related to productivity resulting in losses in wages and fringe benefits. Indirect cost has been defined as “the value of potential output that is lost as a result of any reduction or elimination of work or other activity due to SCI [1]”. The most recent indirect cost estimate is from Canada, which indicates the lifetime indirect costs of SCI are substantial, ranging from 0.7 million to 1.3 million (in 2011 Canadian dollars) assuming injured at age 35 [2]. The estimated annual indirect cost accounts for 41% of the 2.67 billion total economic burdens associated with SCI in Canada [2].
Indirect costs have typically been estimated by the human-capital approach, the willingness-to-pay method, or the friction cost method [3,4,5,6,7]. The human-capital approach is a method that calculates the value of expected post-injury lifetime earnings and fringe benefit losses as a representation of what the individual was expected to make in the future had the injury never taken place, while the willingness-to-pay method aims to estimate the value of lost quality and quantity of life by asking what one would be willing to pay to remove the risk of SCI and its consequences. The friction cost method assumes the production lost due to disease can be restored after a certain time period (friction period). It estimates the indirect costs by using data from the frequency of friction periods, the length of the friction period, absence and productivity, value of production, and the macroeconomic consequences of absence and disability. Besides the three methods, DeVivo, Whiteneck, and Charles utilized a different approach to estimate the indirect cost in a study involving thirteen SCI model systems centers (SCIMS) [8]. They interviewed employed and unemployed participants (age range 15–57 at injury onset) about their current wages and wages at the time of injury. Indirect costs were estimated by the changes in earnings and fringe benefits before and after injury.
To our knowledge, three major studies have estimated indirect costs after SCI in the United States (US). Based on a sample of 332 participants from the SCIMS, DeVivo et al. [8] estimated the average annual indirect costs related to SCI ranged from $34,375 (Frankel D, functional neurologically incomplete, the least impaired group) to $50,470 in 1992 dollars for those with Cervical 1 to Cervical 4 (C1–C4) level injuries (the most severely impaired group). Berkowitz et al. [1] analyzed indirect costs based on interviews with 758 participants with SCI and found the average annual indirect cost of SCI was $12,726 in 1988 dollars. In a follow-up study by Berkowitz [3], the average annual indirect cost increased to $13,566 in 1996 dollars.
All previous studies were based on participants identified through clinical settings, which may have more severe injury than that of a population-based cohort. Furthermore, they were conducted in the 1980s and 1990s and have not been updated since then. Our current study attempted to provide the most recent estimates of indirect costs of SCI by using the same approach as DeVivo et al. [8], and to expand the previous work on the updated direct costs of care after SCI [9, 10]. We examined the changes in employment and earnings after SCI and then estimated annual and lifetime indirect costs for various age and neurologic categories by using a population-based sample. The new estimates were compared with previous findings reported in 1995 [8].
Methods
Participants
The study sample was retrieved from all eligible participants in the South Carolina SCI Outcomes Database, which routinely collects data on a population-based cohort with traumatic SCI who were injured and treated in South Carolina. All participants in the South Carolina SCI Outcomes Database were initially identified through the SCI surveillance system registry in South Carolina (SCISSR), which collects all discharge records of SCI from all nonfederal hospitals in the state. The SCISSR also validates the accuracy of the information from randomly selected medical charts and verifies the data quality. More details of SCISSR can be found elsewhere [11]. Approval was obtained from the Institutional Review Board of the Medical University of South Carolina (approval #: Pro00072655). During the study period of 2016, 307 participants met the inclusion criteria of: (1) residual effects resulting from traumatic SCI, (2) at least 1 year post injury, (3) age between 23 and 64 years at the time of injury onset, (4) younger than 65 years at the time of measurement, and (5) complete information on injury level, injury completeness, employment status, and earnings before and after injury.
Measures
We used four neurologic categories to measure injury severity and impairment: (1) C1–C4 level and nonambulatory, (2) C5–C8 level and nonambulatory, (3) T1-S3 level and nonambulatory, and (4) ambulatory group regardless of injury level. Because we did not measure the American Spinal Injury Association Impairment Scale (AIS) directly, we used ambulatory status as a proxy for AIS D injury. Otherwise, participants were grouped into nonambulatory categories (a proxy for AIS ABC injury). This classification is for comparison purposes with the previous study.
Earnings were grouped as follows: (1) <$10,000, (2) $10,000–$14,999, (3) $15,000–$19,999, (4) $20,000–$24,999, (5) $25,000–$29,999, (6) $30,000–$34,999, (7) $35,000–$39,999, (8) $40,000–$44,999, (9) $45,000–$49,999, (10) $50,000–$59,999, (11) $60,000–$74,999, (12) $75,000–$99,999, (13) $100,000–$124,999, (14) $125,000–$149,999, (15) $150,000–$174,999, and (16) $175,000 or greater. To calculate the average earning losses for all participants, we used a midpoint value for each earning category. For example, $5000 was used as the midpoint for the lowest category of <$9,999; $12,500 as the midpoint for $10,000–$14,999, etc. The highest earning category was $175,000 or more, and we defined $187,500 as the midpoint value for this category. If a participant was not employed, earnings were set to $0. See the Supplementary Appendix for the full study instrument.
Analyses
All analyses were conducted using SAS v9.3. The chi-square statistic was used via the McNemar test to examine the within-individual difference in employment status before and after injury. Paired t-test was performed to compare the pre- and post-injury earnings.
To estimate the indirect costs, each participant’s pre- and post-injury earnings were adjusted for inflation in 2019 (March) dollars using the Employment Cost Index [12]. Because fringe benefits varied historically, we adjusted them for pre- and post-injury earnings separately. By using data from the Department of Labor in 2008 (median year at injury), pre-injury earnings were increased by 30.3% to reflect the net present value of fringe benefits [13]. By using data in 2016 (median year at follow-up), post-injury earnings were increased by 31.5% to reflect the net present value of fringe benefits [14]. The annual indirect costs, defined as the annual forgone earnings and fringe benefits, were calculated as the difference in the sum of pre-injury earnings and benefits before and after injury, using the same approach as DeVivo et al. [8]. We took the summation of individual differences and then calculated the average for each neurologic category.
The lifetime indirect costs were calculated as present value of future costs, which can be interpreted as funds set aside at present in escrow for use throughout the lifetime. We used the following formula [8] to estimate the lifetime indirect costs accounting for increased productivity, the normal probability of surviving, and the discount rate. We are assuming no differences in survival probability as a function of injury severity, although we know that is not the case. We are doing this because our lifetime indirect costs estimate what people with SCI lost assuming they had the same survival probability as the general population. Adjusting figures for injury severity would result in misleading findings (i.e., those with more severe injuries would have lower lifetime indirect costs). The normal probability of surviving was obtained from US Life Tables 2008 [15], and the annual productivity increase was assumed to be 2% based on average productivity increases for the general population between 1990 and 2018. We assumed discount rates to be 2, 4, and 6% separately as the previous study did [8].
\(\sum \left( {{\mathrm{IWAGE}} - {\mathrm{PWAGE}}} \right)\left( {{\mathrm{NPS}}_{\boldsymbol{t}}} \right)({\mathrm{1}} + {\mathrm{p}})^{{\mathrm{t}} - {\mathrm{1}}}/({\mathrm{1}} + {\mathrm{d}})^{{\mathrm{t}} - {\mathrm{1}}},\)
where t = the number of years post injury, IWAGE = the annual earnings plus the value of fringe benefits at the time of injury, PWAGE = the annual earnings plus the value of fringe benefits after SCI, NPSt = the normal probability of surviving to post-injury year t in the absence of SCI given survival to the year of injury, p = the assumed annual increase in productivity, d = the discount rate, reflects the real rate of return on investments over and beyond inflation.
Results
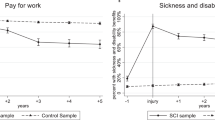
Demographic and injury characteristics are presented in Table 1. The average age at injury was 40, and the average years post injury were 9. Fifty-three percent were non-Hispanic white. Most were male (75%) and AIS D injury (61%). The majority (87%) of the 307 participants were working at the time of injury, while only 35% of them had ever worked after injury. The McNemar test indicated the change was statistically significant (p < 0.01).
We compared the pre- and post-injury earnings among employed participants (Table 2). The percentage in the “$9999 or less” category increased from 10% pre-injury to 21% post-injury, while the earnings range from $25,000 to $44,999 decreased from 35 to 17%. After using the midpoint value for each earnings category and adjusting for inflation and fringe benefits, the average earnings at the time of injury among employed participants was $65,529, and the average earnings at follow-up was $59,710. Then we recalculated the average earnings by including those not actively employed with their earnings set as zero. The average unconditional earnings was $52,680 at the time of injury and $23,326 post injury. The average earnings was significantly decreased (p < 0.01).
After adjusting for inflation and fringe benefits, the average annual indirect cost was $29,354 in 2019 dollars (Table 3). It ranged from $24,125 for AIS D injury to $40,221 for AIS (ABC) and C1–C4 level injury. We adjusted the previous estimates by DeVivo et al. [8] to 2019 dollars for comparison purposes. Their average indirect cost was $79,161, ranging from $71,844 to $105,482, which was substantially higher than the present estimates. We provided their original figures in 1992 dollars in Table 3. They were also higher than our current estimates.
The new estimates of the present value of average lifetime indirect costs (2019 dollars) are presented in Table 4. The results were classified by four neurologic groups for persons who were injured either at 25 or at 50 years old. For someone injured at 25 years old, assuming zero discount rate, the present value of average lifetime indirect costs ranged from 1.4 million to 2.3 million. Assuming a 6% discount rate, the present value ranged from 0.5 million to 0.8 million. The estimated lifetime indirect costs of people injured at 50 years old were reduced substantially because of fewer years of eligible remaining employment. With zero discount rate, the comparable present value of average lifetime indirect costs reduced to 0.4 million and 0.6 million. The value would be 0.3 million and 0.4 million assuming a 6% discount rate. Previous estimates were adjusted in 2019 dollars (Table 5), ranging from 1.4 million to 5.6 million for 25 years old and 0.8 million to 1.7 million for 50 years old. These figures were substantially higher than our estimates in all neurologic categories.
Discussion
Indirect costs are an enormous economic burden after SCI. Our study showed the employment rate decreased from 87 to 35% between pre- and post-injury among 307 study participants who were younger than 65 years at the time of measurement. The indirect costs related both to the diminished employment rate and to the lower earnings. Therefore, both need to be addressed to reduce indirect costs over time.
Not surprising, the indirect costs were related to injury severity, as indicated by both neurologic level and completeness of injury. The indirect costs are particularly high for those with more severe injuries who were injured early in life, so the most likely success in reducing indirect costs is to focus on those who were injured earlier in life, particularly in terms of promoting transition to employment. Fortunately, those who are younger at SCI onset have significant advantages in terms of transitioning to employment. Krause et al. [16] found participants with SCI onset at an age younger than 25 had a 15% higher employment rate than those injured after the age of 45. A similar trend was observed by Hirsh et al.: the younger the age at SCI onset, the higher the employment rate [17]. On the other hand, the earnings differential is much less significant for those who return to the pre-injury employer [18]. Therefore, efforts to maximize return to work among those employed at the time of injury have great potential to limit indirect costs.
Reducing indirect costs after SCI requires improvement in many areas, such as encouraging higher educational achievement, providing job retraining programs, eliminating financial disincentives, and removing environmental and attitudinal barriers. Employers also play an important role in facilitating the employment outcome of people after SCI. When employers are willing to accommodate modifications such as job adaptation, decreased work hours, and structural changes to work environment, people are more likely to return to work after SCI [19, 20]. However, simply improving the employment rate alone is not sufficient to reduce indirect costs fully, as earnings differential, particularly among those transitioning to new employment after SCI, is substantial. State vocational rehabilitation programs often prioritize post-injury employment, defined by 90 days of substantial gainful employment, typically reaching a level of earnings that reduces or eliminates economic benefits. Losing these benefits provides a significant disincentive to employment. If vocational rehabilitation practices are to be maximally successful in reducing indirect costs, they must look beyond 90 days of gainful employment and promote quality employment throughout the lifecycle, including higher earnings, better jobs, and greater work life expectancy. To improve the employment outcome for people with SCI, we should also narrow the gap between males and females. The literature indicates women have less work hours and lower earnings after SCI when compared with men [16, 21, 22].
While the direct costs of care for SCI have increased over the last 25 years [9, 10], it is interesting to note that the new estimates of indirect costs of SCI, based on the employment and earnings changes after SCI, are less than those previously reported in 1995 [8]. One possible explanation is the earnings gap between pre- and post-injury for those who were employed at both time points was narrowed over time. The earnings gap may have been larger 20 years ago, especially before the Americans with Disability Act, which prohibits discrimination based on disability and provides qualified disabled individuals with equal opportunities. The previous study [8] found the average post-injury annual wages plus the fringe benefits were 71% of the pre-injury values after adjusting for inflation and productivity among those employed both before and after injury. Our study’s comparable figure was 91%, which suggests a smaller gap. Another possibility is SCIMS participants in the previous study included the clinical sample from rehabilitation specialty hospitals, including several large cities. It is possible that their higher earnings and earnings lost lead to higher indirect cost estimates than our estimates based on a South Carolina population-based sample.
Study limitations
Our study has several limitations: we used a cross-sectional measure and only represented the time point at which the data were collected. All the data are self-reported with no attempt of verification. Memory of pre-injury earnings may not be completely accurate, and people may underreport post-injury earnings based on fear of losing benefits if someone finds out their true earnings. Our estimates were only based on the perspective of employment and earnings. We did not take societal and household perspectives into consideration, such as losses of tax revenue, vocational rehabilitation program, insurance subsidies, and family member productivity losses due to the caregiver role.
We attempted to make our analyses as comparable as possible with those previously reported by DeVivo et al. [8], but we need to be cautious due to the following methodological differences. Our earnings data were reported as 16 categories by participants, and the highest earnings were capped at $187,500 when we used the midpoint figures to calculate average earnings. There is a possibility that true earnings may deviate among those with extremely high incomes. This may underestimate the indirect costs compared with the previous study, which asked the actual income from participants. Using categories does limit the potential effects of high incomes from disproportionately affecting the average earnings. We did not have data on current student status, so we excluded those who might be students at the time of injury (22 and younger), while the previous study included participants older than 18. Our study was based on earnings information from South Carolina using a population-based cohort, while the previous study used the clinical samples from hospitals [8]. For the same reason, we need to be cautious when applying absolute dollar figures to other states where there may be differences in overall earnings.
Conclusion
This study is the first attempt to estimate the indirect costs after SCI since the 1990s. Although indirect costs are lower when compared with the estimates 20 years ago, they are still a heavy economic burden affecting individuals, their families, and society. To reduce the impact of indirect costs, we need to address the problem of the high unemployment rate after SCI and the gap between pre-injury and post-injury earnings, focusing on promoting successful employment throughout the work lifecycle after SCI.
Data availability
The data sets generated and/or analyzed during the current study are not publicly available due to the privacy concerns of study participants and are not standardized to be in a publicly interpretable format.
References
Berkowitz M, Harvey C, Greene C, Wilson S. The economic consequences of traumatic spinal cord injury. New York: Demos Medical Publications; 1992.
Krueger H, Noonan VK, Trenaman LM, Joshi P, Rivers CS. The economic burden of traumatic spinal cord injury in Canada. Chronic Dis Inj Can. 2013;33:113–22.
Berkowitz M. Economic consequences of spinal cord injury. New Brunswick, NJ: Bureau of Economic Research; 1985.
Hartunian NS, Smart CN, Thompson MS. The incidence and economic costs of major health impairments: a comparative analysis of cancer, motor vehicle injuries, coronary heart disease, and stroke. Lexington, MA: Lexington Books; 1981.
Hodgson TA, Meiners MR. Cost-of-illness methodology: a guide to current practices and procedures. Milbank Mem Fund Q Health Soc. 1982;60:429–62.
Papadakaki M, Stamouli M, Ferraro OE, Orsi C, Otte D, Tzamalouka G, et al. Hospitalization costs and estimates of direct and indirect economic losses due to injury sustained in road traffic crashes: Results from a one-year cohort study in three European countries (The REHABILAID project). Trauma 2017;19:264–76.
Koopmanschap MA, Rutten FF, van Ineveld BM, van Roijen L. The friction cost method for measuring indirect costs of disease. J Health Econ. 1995;14:171–89.
DeVivo M, Whiteneck G, Charles E. The economic impact of spinal cord injury. In: Stover S, DeLisa J, Whiteneck G, editors. Spinal cord injury: clinical outcomes from the model systems. Gaithersburg: Aspen Publishers; 1995.
DeVivo MJ, Chen Y, Mennemeyer S, Deutsch A. Costs of care following spinal cord injury. Top Spinal Cord Inj Rehabil. 2011;16:1–9.
Cao Y, Chen Y, DeVivo M. Lifetime direct costs after spinal cord injury. Top Spinal Cord Inj Rehabil. 2011;16:10–6.
Cao Y, Selassie AW, Krause JS. Risk of death after hospital discharge with traumatic spinal cord injury: a population-based analysis, 1998–2009. Arch Phys Med Rehabil. 2013;94:1054–61.
US Bureau of Labor Statistics. Continuous occupational and industry series September 1975–December 2019. 2019. https://www.bls.gov/web/eci/ecicois.txt.
US Bureau of Labor Statistics. Employer costs for employee compensation news release. 2008. https://www.bls.gov/news.release/archives/ecec_06112008.htm.
US Bureau of Labor Statistics. Employer costs for employee compensation news release. 2016. https://www.bls.gov/news.release/archives/ecec_06092016.htm.
Arias E. United States life tables, 2008. Hyattsville, MD: National Center for Health Statistics; 2012.
Krause JS, Kewman D, DeVivo MJ, Maynard F, Coker J, Roach MJ, et al. Employment after spinal cord injury: an analysis of cases from the model spinal cord injury systems. Arch Phys Med Rehabil. 1999;80:1492–500.
Hirsch AT, Molton IR, Johnson KL, Bombardier C, Jensen MP. The relationship of chronological age, age at injury, and duration of injury to employment status in individuals with spinal cord injury. Psychol Inj Law. 2009;2:263–75.
Krause JS, Edles P, Charlifue S. Changes in employment status and earnings after spinal cord injury: a pilot comparison from pre to post injury. Top Spinal Cord Inj Rehabil. 2011;16:74–9.
Chapin M, Kewman D. Factors affecting employment following spinal cord injury: a qualitative study. Rehabil Psychol. 2001;46:400–16.
Schonherr MC, Croothoff JW, Mulder GA, Schoppen T, Eisma WH. Vocational reintegration following spinal cord injury: expectations, participation and interventions. Spinal Cord. 2004;42:177–84.
Krause JS, Terza JV. Injury and demographic factors predictive of disparities in earnings after spinal cord injury. Arch Phys Med Rehabil. 2006;87:1318–26.
Krause JS, Terza JV, Erten M, Focht KL, Dismuke CE. Prediction of postinjury employment and percentage of time worked after spinal cord injury. Arch Phys Med Rehabil. 2012;93:373–5.
Funding
The contents of this publication were developed under grants from the South Carolina Spinal Cord Injury Research Fund (SCSCIRF) grants SCIRF 11-006, SCIRF 09-001, and SCIRF 2017 SI-02. However, those contents do not necessarily represent the policy of the SCSCIRF, and you should not assume endorsement by the state of South Carolina.
Author information
Authors and Affiliations
Contributions
YC was responsible for the analyses and research methods sections and contributed to the results, discussion, and conclusion sections. JSK was the principal investigator and was responsible for the research design and contributed to the discussion and overall development and editing of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethics
We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Cao, Y., Krause, J.S. Estimation of indirect costs based on employment and earnings changes after spinal cord injury: an observational study. Spinal Cord 58, 908–913 (2020). https://doi.org/10.1038/s41393-020-0447-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41393-020-0447-1
This article is cited by
-
Socioeconomic consequences of traumatic and non-traumatic spinal cord injuries: a Danish nationwide register-based study
Spinal Cord (2022)
-
Epidemiology of traumatic spinal cord injuries in Colombia
Spinal Cord Series and Cases (2021)
-
The association between secondary health conditions and indirect costs after spinal cord injury
Spinal Cord (2021)
