
Abstract
Objective
Evaluate renal outcomes and early predictive factors in infants with congenital posterior urethral valves who required catheter or surgical urinary tract decompression within the first 7 days of life.
Study design
A 10-year retrospective study at a single hospital. Primary outcomes were estimated glomerular filtration rate (eGFR) and development of end stage renal disease (ESRD).
Results
Of 35 infants, 50% developed eGFR <90 mL/min/1.73 m2 and 15% progressed to ESRD. Nadir creatinine, need for invasive ventilation in the newborn period, and need for surgical diversion after catheter diversion were associated with worse outcomes. 50% of infants requiring invasive ventilation as neonates developed eGFR <60 mL/min/1.73 m2 in childhood.
Conclusions
Half of infants with early presentation and intervention developed significant renal insufficiency in childhood, similar to children with later presentation or who had fetal intervention. Invasive ventilation in the newborn period and need for surgical urinary diversion are associated with worse outcomes.
Similar content being viewed by others


Introduction
Congenital posterior urethral valves (PUV) is the most common cause of lower urinary tract obstruction (LUTO) in males, accounting for more than half of pregnancies complicated by LUTO, and results in a spectrum of urologic and renal sequelae [1, 2]. Overall, infants with PUV have poor renal outcomes. The current literature indicates that 20–65% of patients with PUV will develop chronic kidney disease (CKD) and 8–21% will progress to end stage renal disease (ESRD) during childhood. Furthermore, there have been minimal improvements in outcomes over time [3,4,5,6,7,8,9,10,11].
Due to the poor prognosis, significant effort has been put forth to develop interventions for this population, particularly focusing on fetal interventions to relieve the obstruction and allow normal renal and pulmonary development. Fetal intervention, primarily by vesico–amniotic shunting or fetal cystoscopic ablation, has been attempted for nearly 40 years. The cumulative literature suggests that while in utero intervention may reduce perinatal mortality, fetal mortality remains high at 40–60%. Furthermore, these interventions have not improved postnatal outcomes and are associated with surgical complications [12,13,14,15,16].
Although the anatomic anomaly in PUV is relatively uniform, the evaluation of potential interventions has been limited by significant heterogeneity in available cohorts. Reported outcomes combine patients with perinatal and childhood diagnoses, varying severity of obstruction, and both fetal and postnatal interventions. In addition, patients with poor outcomes, such as early death or need for subsequent interventions, are often excluded from data analysis. Such heterogeneity likely also contributes to difficulties in identifying factors predictive of renal outcomes. Small studies have inconsistently shown association of antenatal diagnosis, prematurity, oligohydramnios, renal parenchymal changes, nadir creatinine, vesicoureteral reflux, bladder dysfunction, and younger age at diagnosis with worse renal outcomes; however in multivariate analyses only nadir creatinine has been predictive [4,5,6,7,8,9,10,11, 17,18,19,20,21,22,23].
Given the challenges associated with the heterogeneity of this patient population, the aim of this study was to isolate a specific cohort of infants with severe LUTO caused by PUV who presented and had intervention in the first week of life, to evaluate renal outcomes and early predictive factors.
Materials and methods
Subjects and data management
This study was approved by the Institutional Review Board at Boston Children’s Hospital. Requirement for consent was waived by the Board. Study data were collected and managed using REDCap electronic data capture tools hosted at the study institution [24]. Eligible subjects for this study were male infants born during a retrospective 10-year study period from January 1, 2005 to December 31,2014 who received treatment at a single tertiary children’s hospital for severe LUTO from PUV in the first week of life. Patients treated at the institution for PUV were identified through a data warehouse query using ICD-10 code Q64.2 (Congenital PUV) or CPT procedure code 52400 (Cystourethroscopy with incision, fulguration, or resection of congenital PUV, or congenital obstructive hypertrophic mucosal folds). Patients identified using this query were then reviewed for study inclusion by review of electronic medical records. Patients were included in data collection and analysis if they were: (1) confirmed to have PUV in medical records and (2) had catheter or surgical intervention for urinary tract decompression during the first week of life (n = 35). The aim was to isolate a homogeneous population of infants with severe LUTO, therefore presentation by 7 days of life was selected as it is likely that infants with severe LUTO would develop clinical signs within this time period, and infants with less severe LUTO would likely remain undetected. Patients that were excluded included those who presented after the first week of life or who underwent antenatal urinary tract intervention. Although some excluded patients presented during infancy, many presented during childhood. Children who transferred care after infancy or came to the study institution for second opinion were also excluded.
Outcome measures and methods of analysis
The primary outcome measure was the estimated glomerular filtration rate (eGFR) at last follow-up, and was only used after age 2 years. eGFR was calculated using the bedside Schwartz equation [25]. ESRD was defined as eGFR <15 mL/min/1.73 m2 or requirement for renal replacement therapy.
Covariates included birth gestational age, race, prenatal, and postnatal ultrasound (US) findings, presence of vesicoureteral reflux, nadir creatinine in first year of life, duration of follow-up, other renal or urologic surgical interventions, and any respiratory support required during the newborn or follow-up period. Prenatal US findings included hydroureter, oligohydramnios, renal parenchymal changes, and bladder changes. Postnatal US findings included hydroureter and renal parenchymal changes. Postnatal US findings were assessed at two time points, at first postnatal US and at 1 year of age. Nadir creatinine was categorized as <1 mg/dL or ≥1 mg/dL based on findings in the existing literature, and excluded values after dialysis initiation.
Analysis
Descriptive statistics were calculated. Differences in eGFR at last follow-up between groups by race, birth gestational age, respiratory supports in the newborn period, ultrasound findings, nadir creatinine, vesicoureteral reflux, and other surgical interventions were assessed with either the Kruskal–Wallis test or Mann–Whitney U test. Post hoc pairwise comparisons following the Kruskal–Wallis test were performed with Dunn’s test with the Bonferroni correction. A Kaplan–Meier curve was used to analyze time to development of eGFR <60 mL/min/1.73 m2 (Fig. 1). Stata version 13.1 (StataCorp LLC, College Station, TX) and SPSS version 24 (IBM Corp, Armonk, NY) were used in the analysis. Statistical significance was set at 5%.

Overall renal survival defined as last eGFR of 60 mL/min/1.73 m2 or greater without a renal transplant
Results
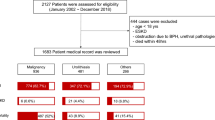
Of 112 children treated for PUV at the study institution between 2005 and 2014 who did not have antenatal intervention, 35 infants presented and had catheter or surgical urinary tract decompression within the first week of life. The remaining 77 presented after 1 week of age. The demographics and characteristics of participants are shown in Table 1. There were 32 (91%) singleton births and 3 (9%) twin births. One infant died at 20 days of life. This infant was included in patient characteristics, however due to the absence of follow-up, analyses that required follow-up data were completed using data from the surviving 34 infants.
Mean laboratory follow-up was 54 months, although clinical follow-up was frequently longer. During this time period, 17 (50%) infants developed eGFR <90 mL/min/1.73 m2, including nine (26%) with eGFR <60 mL/min/1.73 m2 and five (15%) progressed to ESRD (Table 1). All five infants who progressed to ESRD received renal transplants during the study period. Two children included also had other significant medical conditions. One child developed acute lymphoblastic leukemia in infancy, and one child was diagnosed with neurofibromatosis type 1.
15 (43%) children required invasive mechanical ventilation in the neonatal period. Ten (29%) of these children needed high-frequency ventilation. Eleven (32%) required surgical urinary diversion by nephrostomy tube, ureterostomy, or vesicostomy after attempt of catheter drainage rather than, or in addition to ablation of valves.
Among those who survived the newborn period, there were no significant differences in eGFR at last follow-up by race, gestational age, prenatal, or postnatal US findings, or presence of VUR (Table 2). All children with nadir creatinine ≥1 mg/dL developed ESRD. In addition, all children with nadir creatinine ≥1 mg/dL were diagnosed with ESRD within the first month of life. There was a significant number of preterm patients included in this study, with 50% of included patients born before 37 weeks gestation, however there was no difference in overall renal survival between very preterm (<32 weeks gestation), moderate or late preterm (32–36 weeks gestation), or term infants (37 or greater weeks gestation) (p = 0.62). Figure 1 summarizes overall renal survival of all included patients, defined as last eGFR of 60 mL/min/1.73 m2 or greater without a renal transplant.
Infants who required invasive ventilation in the newborn period had lower eGFR at the end of the follow-up period (56 mL/min/1.73 m2) compared with infants who did not require invasive ventilation (95 mL/min/1.73 m2) (p = 0.05). In addition, 80% of infants who developed ESRD required invasive ventilation in the newborn period. Infants who required surgical urinary diversion other than valve ablation had lower eGFR (57 mL/min/1.73 m2) at last follow-up than those with sufficient diversion by catheter drainage (87 mL/min/1.73 m2).
Discussion
In this cohort, 50% of infants with PUV who presented and required catheter or surgical urinary tract decompression in the first week of life developed significant renal insufficiency or ESRD during the study period. These results are concordant with other published cohorts of all children with PUV. We found that elevated nadir creatinine, invasive mechanical ventilation, and requirement for surgical urinary diversion other than routine ablation of valves were predictive factors of eGFR < 60 and ESRD. Given the progressive nature of renal disease associated with PUV, we would anticipate that eGFR would continue to decline over time in this cohort of patients, and further study to trend renal function through childhood and into adulthood is needed, including comparison with children who present at a later age. Children who present at a later age may be at a lower risk for CKD and ESRD, as their pathology is likely associated with only partial obstruction, and may progress at a different rate. The follow-up duration in this study was similar to published cohorts and further emphasizes the need for extended follow-up in all subpopulations of children with PUV.
The renal outcomes of our cohort were similar to those reported for patients who have received fetal intervention for PUV. Efforts to date to improve outcomes by fetal intervention have been relatively unsuccessful and are associated with high fetal and perinatal morbidity and mortality [12,13,14,15,16]. Furthermore, the ability to antenatally recognize and prognosticate the LUTO patients who are at the greatest risk for CKD and ESRD is limited. If technological and scientific developments allow for optimization of fetal interventions, the ability to identify those at greatest risk for CKD will be important to select the correct patients who can benefit from these interventions.
Our cohort contributes to understanding how elements of early care during fetal monitoring and neonatal intensive care could inform outcomes. Our cohort contained a significant number of premature infants and infants who required mechanical ventilation in the neonatal period. The need for invasive ventilation was associated with lower eGFR. This observation is similar to prior studies that also suggest that need for respiratory support may portend worse renal outcomes. Prior studies of patients with PUV have found an association of oligohydramnios with need for respiratory support after birth [26] and an association of early ventilator support with the development of CKD [11]. Although pulmonary hypoplasia of varying severity is associated with other congenital anomalies of the kidney and urinary tract, this has not been typical of PUV. In fact, no children in this cohort had signs of respiratory insufficiency during the follow-up period. These findings suggest that while respiratory failure in the neonatal period may be associated with the development of significant CKD in childhood, it does not appear to lead to long-term pulmonary morbidity in children with PUV. As in other studies, we hypothesize that the need for pulmonary support in the neonatal period is likely related to a combination of factors including oligohydramnios and prematurity. Although there was no association of oligohydramnios with eGFR in our cohort, oligohydramnios was significantly associated with need for invasive ventilation (data not shown). There is also existing literature suggesting an association of prematurity with CKD [27]. Further studies are needed to clarify the causes of neonatal respiratory compromise in children with PUV.
Nadir creatinine ≥1 mg/dL in the first year was found to be significantly associated with low eGFR in this study, supporting previously reported findings. Notably, all infants with elevated nadir creatinine in this study were diagnosed with ESRD and initiated on dialysis within the first month of life; therefore this variable may have limited use as an early predictive factor for the later development of CKD and ESRD. If more sensitive markers of renal function are identified and validated, they may allow an opportunity to more accurately identify changes in renal function sooner than serum creatinine, especially in the neonate.
Important limitations of this study include the retrospective design, single institution experience, small sample size and short duration of follow-up, although similar to existing literature. Prenatal US reports were not universally available and reported prenatal findings relied on documentation in admission and consult notes and likely are underreported. The postnatal US findings were fairly uniformly documented in this institution but results still may be subjective in certain cases.
Conclusions
Half of infants with PUV who presented and had catheter or surgical urinary tract decompression in the first week of life have poor renal outcomes during childhood, however they appear to have similar outcomes compared to published cohorts that include children with later presentation and children after fetal intervention. Infants who required invasive ventilation in the newborn period or required surgical urinary diversion beyond valve ablation after catheter drainage had worse renal outcomes.
References
Malin G, Tonks AM, Morris RK, Gardosi J, Kilby MD. Congenital lower urinary tract obstruction: a population-based epidemiological study. BJOG. 2012;119:1455–64.
Haeri S. Fetal lower urinary tract obstruction (LUTO): a practical review for providers. Matern Health Neonatol Perinatol. 2015;1:26.
Sanna-Cherchi S, Ravani P, Corbani V, Parodi S, Haupt R, Piaggio G, et al. Renal outcome in patients with congenital anomalies of the kidney and urinary tract. Kidney Int. 2009;76:528–33.
Matsell DG, Yu S, Morrison SJ. Antenatal determinants of long-term kidney outcome in boys with posterior urethral valves. Fetal Diagn Ther. 2016;39:214–21.
Bilgutay AN, Roth DR, Gonzales ET Jr., Janzen N, Zhang W, Koh CJ, et al. Posterior urethral valves: risk factors for progression to renal failure. J Pediatr Urol. 2016;12:179.e1–7.
Sarhan OM, El-Ghoneimi AA, Helmy TE, Dawaba MS, Ghali AM, Ibrahiem el HI. Posterior urethral valves: multivariate analysis of factors affecting the final renal outcome. J Urol. 2011;185:2491–5.
Ansari MS, Gulia A, Srivastava A, Kapoor R. Risk factors for progression to end-stage renal disease in children with posterior urethral valves. J Pediatr Urol. 2010;6:261–4.
DeFoor W, Clark C, Jackson E, Reddy P, Minevich E, Sheldon C. Risk factors for end stage renal disease in children with posterior urethral valves. J Urol. 2008;180:1705–8. discussion 8
Sarhan O, Zaccaria I, Macher MA, Muller F, Vuillard E, Delezoide AL, et al. Long-term outcome of prenatally detected posterior urethral valves: single center study of 65 cases managed by primary valve ablation. J Urol. 2008;179:307–12. discussion 12-3
Ylinen E, Ala-Houhala M, Wikstrom S. Prognostic factors of posterior urethral valves and the role of antenatal detection. Pediatr Nephrol. 2004;19:874–9.
Oliveira EA, Rabelo EA, Pereira AK, Diniz JS, Cabral AC, Leite HV, et al. Prognostic factors in prenatally-detected posterior urethral valves: a multivariate analysis. Pediatr Surg Int. 2002;18:662–7.
Farrugia MK. Fetal bladder outlet obstruction: embryopathology, in utero intervention and outcome. J Pediatr Urol. 2016;12:296–303.
Clark TJ, Martin WL, Divakaran TG, Whittle MJ, Kilby MD, Khan KS. Prenatal bladder drainage in the management of fetal lower urinary tract obstruction: a systematic review and meta-analysis. Obstet Gynecol. 2003;102:367–82.
Martinez JM, Masoller N, Devlieger R, Passchyn E, Gomez O, Rodo J, et al. Laser ablation of posterior urethral valves by fetal cystoscopy. Fetal Diagn Ther. 2015;37:267–73.
Holmes N, Harrison MR, Baskin LS. Fetal surgery for posterior urethral valves: long-term postnatal outcomes. Pediatrics. 2001;108:E7.
Salam MA. Posterior urethral valve: outcome of antenatal intervention. Int J Urol. 2006;13:1317–22.
Hochart V, Lahoche A, Priso RH, Houfflin-Debarge V, Bassil A, Sharma D, et al. Posterior urethral valves: are neonatal imaging findings predictive of renal function during early childhood? Pediatr Radiol. 2016;46:1418–23.
Kari JA, El-Desoky S, Farag YM, Mosli H, Altyieb AM, Al Sayad A, et al. Renal impairment in children with posterior urethral valves. Pediatr Nephrol. 2013;28:927–31.
Kibar Y, Ashley RA, Roth CC, Frimberger D, Kropp BP. Timing of posterior urethral valve diagnosis and its impact on clinical outcome. J Pediatr Urol. 2011;7:538–42.
Harvie S, McLeod L, Acott P, Walsh E, Abdolell M, Macken MB. Abnormal antenatal sonogram: an indicator of disease severity in children with posterior urethral valves. Can Assoc Radiol J. 2009;60:185–9.
Lopez Pereira P, Espinosa L, Martinez Urrutina MJ, Lobato R, Navarro M, Jaureguizar E. Posterior urethral valves: prognostic factors. BJU Int. 2003;91:687–90.
Sarhan OM, Helmy TE, Alotay AA, Alghanbar MS, Nakshabandi ZM, Hafez AT. Did antenatal diagnosis protect against chronic kidney disease in patients with posterior urethral valves? A multicenter study. Urology. 2013;82:1405–9.
Coleman R, King T, Nicoara CD, Bader M, McCarthy L, Chandran H, et al. Nadir creatinine in posterior urethral valves: how high is low enough? J Pediatr Urol. 2015;11:356.e1–5.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)–a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42:377–81.
Schwartz GJ, Work DF. Measurement and estimation of GFR in children and adolescents. Clin J Am Soc Nephrol. 2009;4:1832–43.
Eckoldt F, Heling KS, Woderich R, Wolke S. Posterior urethral valves: prenatal diagnostic signs and outcome. Urol Int. 2004;73:296–301.
Carmody JB, Charlton JR. Short-term gestation, long-term risk: prematurity and chronic kidney disease. Pediatrics. 2013;131:1168–79.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Coquillette, M., Lee, R.S., Pagni, S.E. et al. Renal outcomes of neonates with early presentation of posterior urethral valves: a 10-year single center experience. J Perinatol 40, 112–117 (2020). https://doi.org/10.1038/s41372-019-0489-4
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41372-019-0489-4
This article is cited by
-
Kidney disease progression in pediatric and adult posterior urethral valves (PUV) patients
Pediatric Nephrology (2024)
-
Predictive factors for survival in patients with oligohydramnios secondary to antenatal kidney disease
Pediatric Nephrology (2023)
-
Predicting childhood chronic kidney disease severity in infants with posterior urethral valve: a critical analysis of creatinine values in the first year of life
Pediatric Nephrology (2022)
