
Abstract
Background:
Being born small for gestational age (SGA) (birth weight <10th percentile) is connected to decreased white matter (WM) integrity in newborns and increased prevalence of psychiatric symptoms in adulthood. The aims of this study were to investigate whether being born SGA at term affects WM integrity in young adulthood and to explore possible relationships between fractional anisotropy (FA) and pre- and perinatal factors and cognitive and psychiatric outcomes in adulthood in SGA and controls.
Methods:
Diffusion tensor imaging and tract-based spatial statistics were conducted to test for voxelwise differences in FA in SGAs (n = 46) and controls (n = 57) at 18–22 y.
Results:
As compared with controls SGAs had reduced FA in ventral association tracts and internal/external capsules. In the SGAs, no relationship was found between FA and intrauterine head growth in the third trimester, although total intelligence quotient was negatively correlated to FA. In controls, a positive correlation was found between FA and brain growth in the third trimester and maternal smoking. No relationship was found between FA and psychiatric measures in SGAs or controls.
Conclusion:
These results demonstrate that being born SGA leads to reduced WM integrity in adulthood, and suggest that different factors modulate the development of WM in SGA and control groups.
Similar content being viewed by others

Main
Low birth weight (BW) is a marker of less fortunate fetal development, and being born small for gestational age (SGA) (BW <10th percentile) at term is connected to increased risk for cognitive (1), motor (2), behavioral, and psychiatric problems (3,4,5) in childhood, adolescence, and young adulthood. These findings suggest that brain development is influenced by factors leading to SGA status. Although 10% of all newborns fall into the SGA group, this group has received limited attention, and the biological mechanisms connected to the neurodevelopmental deficits remain unclear. The lack of studies in this group is probably connected to problems with reliably distinguishing between different causes leading to SGA status. SGA individuals include infants who are constitutionally small but healthy, and those who have not achieved their optimal growth potential, defined as intrauterine growth restriction (IUGR). The latter are considered to be at risk of adverse postnatal outcomes (6).
Human and animal studies demonstrate that white matter (WM) is vulnerable to suboptimal intrauterine conditions. Postmortem studies of newborn infants with IUGR show reduced myelin concentration (7), and disrupted WM integrity has been demonstrated in vivo in IUGR newborns with magnetic resonance imaging (MRI) and spectroscopy (8). Animal studies of IUGR present evidence of structural WM alterations, including delayed and reduced myelination (9) and retarded axonal outgrowth (10). However, in humans, no significant differences in WM integrity assessed with diffusion tensor imaging (DTI) were found between SGA and controls in the same cohort as this study on adolescence (11). The lack of a significant difference between SGAs and controls could be because of less sensitive DTI acquisition and/or analyses, or differences in WM integrity between the two cohorts could emerge with age as WM continues to develop through adolescence and into adulthood (12). For instance, the proportion of SGAs with psychiatric problems in this cohort increased significantly between adolescence and young adulthood (13), and converging data support an association between WM integrity and a variety of mental disorders (14,15,16) and intelligence quotient (IQ) (17,18,19,20).
On the basis of the increased risk for cognitive and psychiatric problems in SGAs and altered WM found in human and animal studies of IUGR, we hypothesize that WM integrity differs between SGAs and controls in adult age. The primary aim of this study was to investigate WM integrity in early adulthood in subjects born SGA at term as compared with controls using tract-based spatial statistics for voxelwise comparisons of the DTI data (21). Gender effects on fractional anisotropy (FA) in SGAs and controls were also explored because very low birth weight leads to loss of gender differences in FA (18). The second aim was to examine the impact of pre- and perinatal factors on WM integrity in early adulthood in the SGA and control groups. The third aim was to identify any connection between WM integrity and cognitive and psychiatric outcome in adulthood in the SGA and controls groups.
Results
Comparison of DTI Parameters Between SGAs and Controls
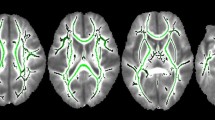
There was a significant reduction in FA in the SGA group as compared with the control group in the uncinate fasciculus, inferior longitudinal fasciculus and inferior fronto-occipital fasciculus bilaterally, and the external capsule and anterior limb of the internal capsule in the right hemisphere ( Figure 1 ). Neither the eigenvalues nor mean diffusivity was found to be significantly different between the SGA and control group on the WM skeleton at the selected significance level. There were no significant increases in FA on the WM skeleton in the SGA group as compared with the controls.

TBSS analysis demonstrated decreased FA in the SGA group as compared with the control group in the right (green) and left (light blue) uncinate fasciculus/inferior fronto-occipital fasciculus/inferior longitudinal fasciculus, right external capsule (blue), and right anterior limb of the internal capsule (red) (P < 0.05, nonparametric permutation test with a correction for multiple comparison, corrected for gender). FA, fractional anisotropy; SGA, small for gestational age; TBSS, tract-based spatial statistics.
Both SGA and control males had higher FA as compared with the respective females in the corticospinal tract, anterior thalamic radiation, and anterior limb of internal capsule (data not shown).
Relationships Between FA and Pre- and Perinatal Factors in SGA and Control Groups
Intrauterine biparietal diameter growth. For the SGA group, there was no correlation between FA values and intrauterine biparietal diameter (BPD) growth, whereas a positive correlation between FA and intrauterine BPD growth was found in all the main central tracts in the control group ( Figure 2 ). There was no difference in BW, head circumference (HC) and length at birth, Apgar scores, and IQ between the SGAs with BPD measurements and those without (results not shown).

In the control group, TBSS analysis identified positive correlations (red voxels) between FA at age 20 and intrauterine BPD growth (P < 0.05, nonparametric permutation test with a correction for multiple comparison, corrected for gender). BPD, biparietal diameter; FA, fractional anisotropy; TBSS, tract-based spatial statistics.
Maternal smoking during pregnancy. For the SGA group, no correlations were found between FA and maternal smoking at time of conception, whereas in the control group, a positive correlation was found in the genu of corpus callosum ( Figure 3 ). Maternal smoking in the SGA group (7.7 ± 7.0 cigarettes/d) was significantly higher as compared with the control group (4.8 ± 6.7 cigarettes/d). There was no difference in the smoking habits between the SGA (2.1 ± 4.8 cigarettes/d) and the control group (2.4 ± 4.2 cigarettes/d) at the time of MRI examination.

In the control group, TBSS analysis identified positive correlations (red voxels) between FA at age 20 and maternal smoking at the time of conception (P < 0.05, nonparametric permutation test with a correction for multiple comparison, corrected for gender). FA, fractional anisotropy; TBSS, tract-based spatial statistics.
Apgar scores, BW, length, and HC at birth. There were no correlations between FA values in young adulthood and Apgar scores (1 and 5 min), BW, length, or HC at birth in the SGAs or controls.
Relationships Between FA and Adult IQ Levels and Psychiatric Outcome in SGA and Control Groups
In the SGA group, FA was negatively correlated with total IQ in corpus callosum (genu and body), inferior fronto-occipital fasciculus, inferior longitudinal fasciculus, and posterior thalamic radiation ( Figure 4 ). There was no correlation between FA and IQ in the control group. The mental health variables were not found to correlate with FA in the SGA or control group.

In the SGA group, TBSS analysis identified negative correlations (red voxels) between FA and total intelligence quotient (P < 0.05, nonparametric permutation test with a correction for multiple comparison, corrected for gender). FA, fractional anisotropy; SGA, small for gestational age; TBSS, tract-based spatial statistics.
Discussion
Reduced FA in the ventral association tracts and internal and external capsules are signs of definite changes in the WM microstructure in the brains of young adults born SGA at term. Brain growth in the third trimester and maternal smoking appeared to affect WM integrity differently in the SGAs and controls, pointing to differential effects of environmental influences on brain development in the normally developing and the SGA fetus. Furthermore, higher IQ was associated with decreased FA in the SGAs, but not in the controls, indicating that alterations in WM structure have functional consequences for the SGAs. Psychiatric variables were higher in the SGAs, but no relationship could be found between these and WM structure.
Comparison of DTI Parameters Between SGAs and Controls
Reduced FA generally represents damaged or reduced organization of WM bundles (22) and is related to axon injury and reductions in myelination (23). This is in line with the described alterations in WM in animal IUGR studies and postmortem term SGA studies (7,9,10,24,25). It is well established that insulin growth factors have an important role in fetal and postnatal WM growth (26), promoting proliferation of oligodendrocytes as well as myelin synthesis (27). Levels of insulin growth factors are low in human SGA newborns (26), possibly influencing early development of WM and thus affecting FA also in early adulthood.
An alternative explanation for the differences in FA between the SGAs and the controls is differences in WM maturation trajectories during the late teens between the two groups. Development of WM occurs mainly during the first few years of life (28,29), but continues through adolescence and into adulthood (12). Because there were no group differences in FA at 15 y of age between SGAs and controls (11), the reduced WM integrity found in the SGA group at 20 y may stem from slower WM development as compared with controls. However, at 15 y the DTI was acquired in only six directions with a slice thickness of 5 mm, and the voxelwise DTI analyses has improved from the last study. The MRI data and analyses methods used in this population at 15 y may therefore not have had sufficient sensitivity to detect small WM structural differences.
On the basis of the consistent finding of reduced number of axons and myelination present from birth in animal models of IUGR and postmortem studies in human IUGR/SGA newborns, combined with the DTI results from the previous and this SGA study, a combination of the two alternative explanations above represents a third possibility. The reduced number of axons and decreased myelination are present from birth in the SGA group, but the major differences between the groups might evolve slowly and become more evident as WM matures.
Relationships Between FA and Pre- and Perinatal Factors in SGA and Control Groups
Intrauterine BPD growth. The rate of intrauterine BPD growth did not influence WM integrity in the SGA group, only in the controls. The lack of an association between FA and intrauterine BPD growth in the SGAs points to factors other than brain growth in the last trimester as determining factors for postnatal development of WM to early adulthood in SGAs. Because the intrauterine growth data were from gestational week 33 and 37, any influence of restricted intrauterine growth before 33 wk gestation could not be explored. Factors such as number of days in the intensive care unit and respiratory problems can also affect brain development (18). However, all SGA and control subjects, even the few staying in the neonatal intensive care unit, were discharged as healthy babies. It is unlikely that such factors played a role in the difference seen in FA between SGA and controls.
Maternal smoking during pregnancy. In the controls, a positive correlation was found between amount of smoking during pregnancy and FA in the genu of corpus callosum. Previous studies have found the same positive association between FA in corpus callosum and prenatal exposure to maternal smoking, and self-smoking in adolescents and adults (30,31). One possible explanation for the positive association between FA and maternal and self-smoking is related to the neurogenic properties of nicotinic receptors (31), including promotion of gene expression involving neurogenesis and nerve growth, and regulation of oligodendrocyte development (32,33). However, why this difference is repeatedly demonstrated in the genu of corpus callosum and the functional consequence of this increase in microstructural integrity remain undetermined.
To our surprise, there was no effect of maternal smoking on WM structure in the SGA group, even though the SGA mothers smoked significantly more than the control mothers. These results suggest that the effect of smoking is concealed by factors with a stronger impact on the development of WM in the SGA subjects. Indeed, it has been shown that certain adverse outcomes, such as psychiatric diagnosis in the offspring of mothers who smoked during pregnancy, are not causally related to smoking, but rather result from inherited factors (34,35). In light of these results, it is possible that genetic differences between the SGA and the control mothers influence WM microstructure to a greater extent, or give rise to differences in susceptibility to the effects of smoking on WM in the two groups.
Relationships Between FA and Adult IQ Levels and Psychiatric Outcome in SGA and Control Groups
IQ. We found a negative correlation between FA and total IQ in young SGA adults, whereas no correlation between FA and IQ in the control group was found. Increased FA has been associated with both increased (17,18,20) and decreased IQ (19), demonstrating that there is no one-to-one relationship between FA and IQ. In SGA individuals with lower IQ, increased FA in certain tracts could represent a compensatory, although less efficient, rewiring of brain WM circuitry supporting complex neuropsychological tasks. This has been shown in Turner syndrome girls with language deficits (36). IQ is, however, a complex measure that includes a large number of brain operations dependent on different fiber pathways and cortical and subcortical structures. The relationship between FA as an approximation for WM microstructure and IQ is largely unknown, and may differ between the genders (19) and between normal and pathological brains (18). Indeed, the negative correlation between FA in the genu and body of corpus callosum and IQ suggests that this change may be beneficial for the SGA group.
Psychiatric outcome. An increasing odds ratio for all categories of psychiatric diseases and decreased BW has been established (37), which is in line with the increase in psychiatric diagnosis and symptom scores in the SGA as compared with the control group. However, no relationship was found between FA and mental health in any of the groups. Converging evidence does, however, support an association between disturbances in WM integrity and a variety of mental disorders (14,15,16) in DTI studies, but these studies have included larger and more homogenous clinical groups as compared with the SGA group in this study.
Limitations
There are limitations to our study that should be taken into account when interpreting the results. First, when using tract-based spatial statistics, only the center core of the WM tracts are studied, and therefore possible differences in the more peripheral tracts are lost. Second, intrauterine BPD growth measures were only performed in a subgroup of this population. This subgroup was, however, not different from the SGAs without BDP measurements with regard to BW, HC and length at birth, Apgar scores, and IQ, and thus appear to be representative for the entire SGA group. Third, correlation analyses do not show causality, and when correlating FA values with the various pre- and perinatal data, there will always be a possibility that other underlying factors are responsible for statically significant correlations. Finally, the relationship between axon and myelin damage and the DTI metrics has yet to be firmly established.
Conclusion
The results show that being born SGA leads to definite WM microstructural changes in adulthood, probably caused by reduced number of axons and myelination present from birth and differences in the development of WM. Intrauterine BPD growth during the last trimester and intrauterine exposure to smoking had no measurable effect on WM integrity in adulthood in SGAs in contrast to the controls. Furthermore, alterations in WM structure have functional consequences for the SGAs as FA values correlated negatively with IQ. A similar pattern was not found in the controls. Taken together, these results imply that different factors modulate the development of WM in SGA and control groups, leading to differences in WM microstructure and intrinsic wiring properties between the groups. Given the nature of the SGA definition, marked differences in WM in the 10% lowest BW cohort represents a substantial number of affected individuals.
Methods
Subjects
This study was part of a population-based follow-up study of a SGA group born at term (37–42 completed weeks) with a BW <10th percentile adjusted for gestational age, gender, and parity, and a control group born at term with BW ≥10th percentile for gestational age (38).
SGA and control children were enrolled before gestational week 20 during the period 1986–1988 and followed prospectively (38,39). These children were the second or third births of mothers living in the Trondheim area of Norway. Of 1,200 eligible women, 104 gave birth at full term to a singleton SGA child. One newborn with a congenital syndrome was excluded, 17 had moved or could not be traced, and 31 did not consent. Therefore, 55 subjects (24 men) participated at the follow-up in young adulthood, of these 49 underwent MRI. Because of image artifacts, three subjects were excluded, leaving 46 MRIs suitable for analysis in the SGA group. Of the 46 SGAs included in the study, four had a stay in the neonatal intensive care unit for 1, 1, 1, and 6 d, respectively. One was admitted due to initial respiratory problems, and the others for observation of transitional problems such as grunting. All were discharged as healthy babies without a specific diagnosis. In addition, one SGA had hypoglycemia. The IQs of these individuals were between 80 and 102 at the time of MRI.
The control group included 120 subjects from a 10% random sample of mothers (38). Two with congenital syndrome were excluded, 16 had moved or could not be traced, and 27 did not consent. Therefore, 75 subjects (32 men) participated at follow-up, and 65 of these were examined with MRI. Eight DTI scans were excluded because of image artifacts, leaving 57 MRI investigations suitable for DTI analysis in the controls. Two of the controls stayed in the neonatal intensive care unit for 5 and 9 d, respectively, the latter due to respiratory problems and hypoglycemia. Both were discharged as healthy babies. See Table 1 for summary characteristics of the subjects included in the DTI analysis.
The study was approved by the Regional Committee for Medical Research Ethics (project number 4.2005.2605), and written informed consent was obtained from the participants.
Pre- and Perinatal Factors
Clinical data from pre- and perinatal periods obtained from SGA and control individuals included Apgar scores (1 min and 5 min), gender, BW, HC and length at birth, and maternal smoking at the time of conception (number of cigarettes per day) ( Table 1 ). For each participant, smoking habits at the time of MRI examination were registered. Two sample Student’s t-tests (P < 0.05) were used for comparing the pre- and perinatal data between the groups.
Intrauterine brain growth. The impact of third trimester brain growth on adult WM integrity was assessed in a subsample of individuals (24 SGAs and 49 controls) who had ultrasound BPD measurements at 33 and 37 wk. For the SGA and controls, the deviation from the mean BPD at 33 and 37 wk for 40,000 births in Norway (http://www.nsfm.no/esnurra) was calculated (40). The BPD deviation change between 33 and 37 wk was denoted as intrauterine BPD growth ( Table 1 ). A negative intrauterine BPD growth (<0%) was considered to be BPD growth restriction. To investigate any bias in the SGA group with BPD measurements as compared with those without, BW, HC and length at birth, Apgar scores, and IQ between these two groups were assessed with a Student’s t-test, and a statistical threshold of P < 0.05.
Outcome Measures
IQ. The Wechsler Adult Intelligence Scale-III (WAIS-III) was performed during one session by a neuropsychologist who was blinded to group adherence (41). Age-appropriate norms were used to calculate IQ scores in the SGA (n = 46) and control (n = 57) groups (42). Total IQ was 95.9 ± 9.7 for the SGA group and 99.6 ± 11.2 for the control group (t-test, P = 0.09).
Psychiatric assessment. A total of 41 SGAs and 56 controls were diagnosed with the Schedule for Affective Disorder and Schizophrenia for School-Age Children (K-SADS-PL) (43), Children’s Global Assessment Scale (CGAS) (44), and attention-deficit hyperactivity disorder (ADHD) Rating Scale IV Adult Self Report (45). The SGA group had more psychiatric diagnoses (ADHD and anxiety), lower CGAS scores, and higher self-report scores on the ADHD Rating Scale than controls (5) ( Table 2 ).
Statistics for Demographical and Clinical Variables
Two-sample Student’s t-tests were used for comparing the pre- and perinatal data and IQ measurements between the groups. χ2 Tests were used for comparing ADHD and anxiety disorders, Student’s t-tests were used for comparing CGAS scores, and Mann–Whitney U-tests were used to compare the ADHD Rating Scale between the SGA and control groups, respectively. P < 0.05 was chosen as the significance level for all the statistical tests.
Image Acquisition
The DTI data was acquired on a 1.5 Tesla Siemens Magnetom Symphony (Siemens, Erlangen, Germany) using a single-shot balanced-echo EPI sequence in 12 noncollinear directions with b = 1,000 s/mm2 and the following parameters: TR = 10,400 ms, TE = 100 ms, field of view 280 × 280 mm, slice thickness 2.2 mm, acquisition matrix 128 × 128, and 55 transversal slices with no gap. The DTI sequence was repeated six times for increased signal-to-noise ratio. The MRI data acquisition was carried out when the participants were 18–22 y of age.
Image and Statistical Analysis
DTI analysis was performed with the FMRIB software library (FSL, Oxford Centre for Functional MRI of the Brain, Oxford, UK; www.fmrib.ox.ac.uk/fsl). Image artifacts caused by motion and eddy current distortions were minimized by registration of all the DTI acquisitions to the b = 0 image using affine registration. The brain was extracted using Brain Extraction Tool (BET, part of FSL) (21). FMRIB’s Diffusion Toolbox (FDT) was used to fit a diffusion tensor model to the raw diffusion data in each voxel (46), creating voxelwise maps of the eigenvalues (λ1, λ2, and λ3), FA, and mean diffusivity for the SGA and control groups.
Voxelwise statistical analysis of the diffusion data was performed using tract-based spatial statistics (part of FSL) (21). A detailed description is given elsewhere (18). Voxelwise statistics of the skeletonised FA, mean diffusivity, and eigenvalues (λ1, λ2, and λ3) were carried out on the WM skeleton using Randomize (part of FSL) to test for group differences between SGAs and controls. Randomize performs a nonparametric permutation test with a correction for multiple comparisons and statistical significance level set to P < 0.05 with gender regressed out (47).
Randomize was also used to examine the gender differences in FA in the SGA and control groups. Furthermore, Randomize and multiple linear regression analysis were used to examine the relationship between FA and the pre- and perinatal factors ( Table 1 ) and between FA and total IQ and psychiatric data at the age of 20 in the SGA and control groups separately. The impact of maternal smoking habits on FA at time of conception was corrected for participant smoking habits at the time of MRI.
In all images, the background image is the mean FA map of all subjects in this study. The images are shown in radiological convention, i.e., the right side of the subjects is on the left side of the images.
Statement of Financial Support
The study was funded by the Research Council of Norway (NevroNor project), the Norwegian University of Science and Technology (NTNU), and Medical Imaging Laboratory (MI Lab) in Trondheim.
References
Strauss RS . Adult functional outcome of those born small for gestational age: twenty-six-year follow-up of the 1970 British Birth Cohort. JAMA 2000;283:625–32.
Evensen KA, Sigmundsson H, Romundstad P, Indredavik MS, Brubakk AM, Vik T . Inter- and intra-modal matching in very low birth weight and small for gestational age adolescents. Early Hum Dev 2007;83:19–27.
Elgen I, Sommerfelt K, Markestad T . Population based, controlled study of behavioural problems and psychiatric disorders in low birthweight children at 11 years of age. Arch Dis Child Fetal Neonatal Ed 2002;87:F128–32.
Indredavik MS, Vik T, Heyerdahl S, Kulseng S, Brubakk AM . Psychiatric symptoms in low birth weight adolescents, assessed by screening questionnaires. Eur Child Adolesc Psychiatry 2005;14:226–36.
Lund LK, Vik T, Skranes J, Brubakk AM, Indredavik MS . Psychiatric morbidity in two low birth weight groups assessed by diagnostic interview in young adulthood. Acta Paediatr 2011;100:598–604.
Patterson RM, Pouliot MR . Neonatal morphometrics and perinatal outcome: who is growth retarded? Am J Obstet Gynecol 1987;157:691–3.
Chase HP, Welch NN, Dabiere CS, Vasan NS, Butterfield LJ . Alterations in human brain biochemistry following intrauterine growth retardation. Pediatrics 1972;50:403–11.
Sanz-Cortés M, Figueras F, Bargalló N, Padilla N, Amat-Roldan I, Gratacós E . Abnormal brain microstructure and metabolism in small-for-gestational-age term fetuses with normal umbilical artery Doppler. Ultrasound Obstet Gynecol 2010;36:159–65.
Nitsos I, Rees S . The effects of intrauterine growth retardation on the development of neuroglia in fetal guinea pigs. An immunohistochemical and an ultrastructural study. Int J Dev Neurosci 1990;8:233–44.
Bassan H, Kidron D, Bassan M, et al. The effects of vascular intrauterine growth retardation on cortical astrocytes. J Matern Fetal Neonatal Med 2010;23:595–600.
Vangberg TR, Skranes J, Dale AM, Martinussen M, Brubakk AM, Haraldseth O . Changes in white matter diffusion anisotropy in adolescents born prematurely. Neuroimage 2006;32:1538–48.
Lebel C, Walker L, Leemans A, Phillips L, Beaulieu C . Microstructural maturation of the human brain from childhood to adulthood. Neuroimage 2008;40:1044–55.
Lund LK, Vik T, Skranes J, Lydersen S, Brubakk AM, Indredavik MS . Low birth weight and psychiatric morbidity; stability and change between adolescence and young adulthood. Early Hum Dev 2012;88:623–9.
Davenport ND, Karatekin C, White T, Lim KO . Differential fractional anisotropy abnormalities in adolescents with ADHD or schizophrenia. Psychiatry Res 2010;181:193–8.
Phan KL, Orlichenko A, Boyd E, et al. Preliminary evidence of white matter abnormality in the uncinate fasciculus in generalized social anxiety disorder. Biol Psychiatry 2009;66:691–4.
White T, Nelson M, Lim KO . Diffusion tensor imaging in psychiatric disorders. Top Magn Reson Imaging 2008;19:97–109.
Chiang MC, Barysheva M, Shattuck DW, et al. Genetics of brain fiber architecture and intellectual performance. J Neurosci 2009;29:2212–24.
Eikenes L, Løhaugen GC, Brubakk AM, Skranes J, Håberg AK . Young adults born preterm with very low birth weight demonstrate widespread white matter alterations on brain DTI. Neuroimage 2011;54:1774–85.
Schmithorst VJ . Developmental sex differences in the relation of neuroanatomical connectivity to intelligence. Intelligence 2009;37:164–73.
Skranes J, Vangberg TR, Kulseng S, et al. Clinical findings and white matter abnormalities seen on diffusion tensor imaging in adolescents with very low birth weight. Brain 2007;130(Pt 3):654–66.
Smith SM, Jenkinson M, Johansen-Berg H, et al. Tract-based spatial statistics: voxelwise analysis of multi-subject diffusion data. Neuroimage 2006;31:1487–505.
Cascio CJ, Gerig G, Piven J . Diffusion tensor imaging: Application to the study of the developing brain. J Am Acad Child Adolesc Psychiatry 2007;46:213–23.
Counsell SJ, Shen Y, Boardman JP, et al. Axial and radial diffusivity in preterm infants who have diffuse white matter changes on magnetic resonance imaging at term-equivalent age. Pediatrics 2006;117:376–86.
Mallard C, Loeliger M, Copolov D, Rees S . Reduced number of neurons in the hippocampus and the cerebellum in the postnatal guinea-pig following intrauterine growth-restriction. Neuroscience 2000;100:327–33.
Sasaki J, Fukami E, Mimura S, Hayakawa M, Kitoh J, Watanabe K . Abnormal cerebral neuronal migration in a rat model of intrauterine growth retardation induced by synthetic thromboxane A(2). Early Hum Dev 2000;58:91–9.
Randhawa RS . The insulin-like growth factor system and fetal growth restrictionn. Pediatr Endocrinol Rev 2008;6:235–40.
Zumkeller W . The effect of insulin-like growth factors on brain myelination and their potential therapeutic application in myelination disorders. Eur J Paediatr Neurol 1997;1:91–101.
Hermoye L, Saint-Martin C, Cosnard G, et al. Pediatric diffusion tensor imaging: normal database and observation of the white matter maturation in early childhood. Neuroimage 2006;29:493–504.
Provenzale JM, Liang L, DeLong D, White LE . Diffusion tensor imaging assessment of brain white matter maturation during the first postnatal year. AJR Am J Roentgenol 2007;189:476–86.
Jacobsen LK, Picciotto MR, Heath CJ, et al. Prenatal and adolescent exposure to tobacco smoke modulates the development of white matter microstructure. J Neurosci 2007;27:13491–8.
Paul RH, Grieve SM, Niaura R, et al. Chronic cigarette smoking and the microstructural integrity of white matter in healthy adults: a diffusion tensor imaging study. Nicotine Tob Res 2008;10:137–47.
Perry EK, Smith CJ, Atack JR, Candy JM, Johnson M, Perry RH . Neocortical cholinergic enzyme and receptor activities in the human fetal brain. J Neurochem 1986;47:1262–9.
Rogers SW, Gregori NZ, Carlson N, Gahring LC, Noble M . Neuronal nicotinic acetylcholine receptor expression by O2A/oligodendrocyte progenitor cells. Glia 2001;33:306–13.
D’Onofrio BM, Van Hulle CA, Waldman ID, et al. Smoking during pregnancy and offspring externalizing problems: an exploration of genetic and environmental confounds. Dev Psychopathol 2008;20:139–64.
Rice F, Harold GT, Boivin J, Hay DF, van den Bree M, Thapar A . Disentangling prenatal and inherited influences in humans with an experimental design. Proc Natl Acad Sci USA 2009;106:2464–7.
Holzapfel M, Barnea-Goraly N, Eckert MA, Kesler SR, Reiss AL . Selective alterations of white matter associated with visuospatial and sensorimotor dysfunction in turner syndrome. J Neurosci 2006;26:7007–13.
Abel KM, Wicks S, Susser ES, et al. Birth weight, schizophrenia, and adult mental disorder: is risk confined to the smallest babies? Arch Gen Psychiatry 2010;67:923–30.
Vik T, Vatten L, Jacobsen G, Bakketeig LS . Prenatal growth in symmetric and asymmetric small-for-gestational-age infants. Early Hum Dev 1997;48:167–76.
Bakketeig LS, Jacobsen G, Hoffman HJ, et al. Pre-pregnancy risk factors of small-for-gestational age births among parous women in Scandinavia. Acta Obstet Gynecol Scand 1993;72:273–9.
Gjessing HK, Grøttum P, Eik-Nes SH . A direct method for ultrasound prediction of day of delivery: a new, population-based approach. Ultrasound Obstet Gynecol 2007;30:19–27.
Løhaugen GC, Gramstad A, Evensen KA, et al. Cognitive profile in young adults born preterm at very low birthweight. Dev Med Child Neurol 2010;52:1133–8.
Kaufman AS, Lichtenberger EO . Assessing Adolescent and Adult Intelligence, 3rd edn. Hoboken, NJ: John Wiley, 2006.
Kaufman J, Birmaher B, Brent D, et al. Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version (K-SADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry 1997;36:980–8.
Shaffer D, Gould MS, Brasic J, et al. A children’s global assessment scale (CGAS). Arch Gen Psychiatry 1983;40:1228–31.
Barkley RA . Attention-deficit hyperactivity disorder. Sci Am 1998;279:66–71.
Basser PJ, Pierpaoli C . Microstructural and physiological features of tissues elucidated by quantitative-diffusion-tensor MRI. J Magn Reson B 1996;111:209–19.
Nichols TE, Holmes AP . Nonparametric permutation tests for functional neuroimaging: a primer with examples. Hum Brain Mapp 2002;15:1–25.
Acknowledgements
We thank the subjects in the study for participation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Eikenes, L., Martinussen, M., Lund, L. et al. Being born small for gestational age reduces white matter integrity in adulthood: a prospective cohort study. Pediatr Res 72, 649–654 (2012). https://doi.org/10.1038/pr.2012.129
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pr.2012.129
This article is cited by
-
Early life factors and structural brain network in children with overweight/obesity: The ActiveBrains project
Pediatric Research (2023)
-
Brain volumes and white matter microstructure in 8- to 10-year-old children born with fetal growth restriction
Pediatric Radiology (2022)
-
Combination of human endothelial colony-forming cells and mesenchymal stromal cells exert neuroprotective effects in the growth-restricted newborn
npj Regenerative Medicine (2021)
-
Neuropathology in intrauterine growth restricted newborn piglets is associated with glial activation and proinflammatory status in the brain
Journal of Neuroinflammation (2019)
