
Abstract
Introduction:
Individuals with isolated cleft lip and/or palate (ICLP) are often reported to be of shorter stature relative to peers, and the objective of this study was to explore the role of the pituitary in relationship to growth.
Methods:
Fifty-five males and 32 females with ICLP were compared to 121 healthy males and 158 healthy females with respect to height and BMI. Magnetic resonance imaging (MRI) scans were obtained from all ICLP participants and 47% of healthy group participants.
Results:
Males with ICLP were shorter than healthy males and had lower BMI. However, the trajectories for height and BMI did not differ between groups. Analyses in a separate sample of adult males suggested that height normalizes in males with ICLP in their early 30s. There were no differences in mean pituitary volume and pituitary trajectories between male groups. Females with ICLP were shorter than healthy females and also had slower growth rates. They did not differ in mean BMI or BMI trajectories. Furthermore, there were no differences in mean pituitary volume, or in pituitary trajectories.
Discussion:
Our findings suggest that there are no gross morphological differences in pituitary volume in individuals with ICLP, although more subtle differences may exist.
Similar content being viewed by others

Main
Oral clefts are among the most common congenital disorders, affecting about 10 babies per 10,000 births (1,2). About 70% of all oral clefts are isolated (i.e., not part of a known syndrome) and are referred to as isolated cleft lip and/or palate (ICLP (3,4)). Clefts are the result of insufficient fusion of the palatal shelves and facial swellings between the 5th and 10th wk of embryonic development (5). This is caused, at least in part, by a failure of neural crest cells to migrate properly into the facial region (6).
Compared to the general population, children with ICLP are more likely to have short stature (7) and to have growth hormone deficiency (8). Of note, the majority of patients with ICLP do not suffer from severe growth retardation (9) but are nevertheless significantly shorter than age-matched peers (10,11,12,13,14). Although there are quite a few studies on growth in children with ICLP (7,11,15), studies in individuals beyond the age of 12 y are rare. In one study of 19-y-old males with ICLP, males with cleft palate only (CPO) were shorter compared to healthy peers, although their BMI was normal, whereas males with clefts of the lip and/or palate were of average height but had significantly lower BMI relative to peers (16). This suggests that that cleft phenotype may have an effect on long-term outcomes. Others have speculated that males with ICLP catch up in growth later in development, whereas females with ICLP remain shorter (15). To our knowledge, this hypothesis has not been directly tested in a relatively wide age range.
As oral clefts pose problems with feeding, it has been proposed that the observed growth lag may be related to insufficient nutrition (10). However, modern health care and appliances have greatly improved feeding of infants with ICLP (17,18). Moreover, one study found that feeding problems did not account for differences in height between children with ICLP and healthy peers (11).
Alternatively, it could be the case that growth problems in ICLP are related to abnormalities in the pituitary gland, a structure critical for normal growth (19). The anterior portion of the pituitary produces six hormones, including growth hormone, which plays a crucial role in muscle and long bone growth (19,20,21). Furthermore, magnetic resonance imaging (MRI) studies have demonstrated that pituitary gland volume increases with age from childhood to young adulthood (22,23,24,25,26).
Given the unique embryonic origin of the pituitary gland, it may be the case that orofacial clefts pose a risk for abnormal pituitary development. That is, the anterior pituitary is formed from an ectodermal placode located near the future mouth in between the mandibular and maxillary processes (5,8,27,28). This placode invaginates to form Rathke’s pouch, migrates dorsally, and differentiates into the anterior pituitary (5). A recent study in mice showed that the anterior pituitary is indeed significantly affected in those with orofacial clefts (29). Taken together, there seems to be compelling evidence that orofacial malformations disturb the development of the pituitary (27) and, hence, growth.
This study aimed to explore the role of the pituitary gland in abnormal growth in individuals with ICLP. To this end, participants with and without ICLP in the age range of 7–25 y were compared in terms of height and BMI. In addition, volume of the pituitary gland was compared between groups. Given previous reports on height and BMI in ICLP, it was hypothesized that individuals with ICLP would be shorter and have lower BMI than their peers. Furthermore, given the potential risk that orofacial clefts pose on early pituitary development, it was expected that the pituitary gland would be abnormal in individuals with ICLP. Finally, as an ad hoc analysis, a separate sample of adult males (ages 18–50) with ICLP was analyzed along with the younger male sample (ages 7–25) to provide a long-term trajectory of growth.
Results
Comparison of Mean Height
After adjusting for the effects of age and repeated measures, both males and females with ICLP were significantly shorter relative to the normal comparison (NC) group (P = 0.0153, and P = 0.0027, respectively; Table 1 ). Although significantly shorter than the NC group, the current sample of individuals with ICLP did not include any individuals who were at least two standard deviations below the mean of the NC group. That is, the current sample did not include individuals who had major growth malformations or clinically deemed short stature.
Comparison of Height Trajectories
Age-by-height regression lines for males and females are depicted in Figure 1a,b , respectively. A test of the difference in the two slopes for males showed that the effect of age on height did not differ in the two groups (P = 0.5485). This suggests that males with ICLP are, on average, shorter throughout the time period assessed (up through 24 y of age).

Height and BMI trajectories. Panel (a) depicts age by height for the NC males (open circles, solid regression line) and males with ICLP (shaded circles, dotted regression line). Panel (b) depicts age by height for NC females (open triangles, solid regression line) and females with ICLP (shaded triangles, dotted regression line). Panel (c) depicts age by BMI for NC males (open circles, solid regression line) and males with ICLP (shaded circles, dotted regression line). Panel (d) depicts age by BMI for NC females (open triangles, solid regression line) and females with ICLP (shaded triangles, dotted regression line). ICLP, isolated cleft lip and/or palate; NC, normal comparison.
However, a comparison of the two slopes for females revealed a significant difference in the effect of age on height for the two groups (P = 0.0044), as females with ICLP tended to grow more slowly and therefore tended to be shorter later on.
Comparison of Mean BMI
Table 1 shows the means and P values of the comparisons of BMI for males and females. After adjusting for age and repeated measures, males with ICLP had significantly lower BMI than comparison males (P = 0.0297); however, for females there was no significant difference in terms of BMI (P = 0.7332).
Comparison of BMI Trajectories
Age-by-BMI regression lines for males and females are depicted in Figure 1c,d , respectively. A test of the difference of the two slopes for males showed that the effect of age on BMI did not differ in the two groups (P = 0.3480). This suggests that males with ICLP tend to have lower BMI throughout the time period assessed. Furthermore, a test of the difference in the two slopes for females revealed that the effect of age on BMI did not differ in the two groups (P = 0.9219).
Comparison of Mean Pituitary Volumes
Table 2 shows the means and P values of the t-tests for males and females. There was no significant difference in mean pituitary volumes in cubic centimeters between groups for either sex.
These results did not change when the analyses were adjusted for age and repeated measures. That is, pituitary volume did not differ between males (P = 0.3052) or females (P = 0.2500) with and without ICLP.
Comparison of Pituitary Volume Trajectories
Figure 2a,b show the regression lines for age and pituitary volume for males and females, respectively. After adjusting for repeated measures, the correlation between age and pituitary volume for NC males was r = 0.372 (P = 0.0012) and for males with ICLP r = 0.268 (P = 0.0514). In addition, the adjusted correlation between age and pituitary volume for NC females was r = 0.628 (P < 0.0001) and for females with ICLP r = 0.437 (P = 0.0069).

Pituitary trajectories. Panel (a) depicts age by pituitary volume for NC males (open circles, solid regression line) and males with ICLP (shaded circles, dotted regression line). Panel (b) depicts age by pituitary volume for NC females (open triangles, solid regression line) and females with ICLP (shaded triangles, dotted regression line). cc, cubic centimeters; ICLP, isolated cleft lip and/or palate; NC, normal comparison.
Although the correlations were generally stronger for the NC groups relative to the ICLP groups, tests of difference in regression slopes revealed that the slopes were not significantly different between males (P = 0.2010) or females (P = 0.2318) with or without ICLP.
Ad hoc Analysis: Long-Term Trajectory of Height
Height measures were available for a separate sample of adult males with and without ICLP. The growth trends for the two groups are plotted as a Loess curve ( Figure 3 ) to descriptively capture the progressive growth during childhood and adolescence and the growth plateau during the second decade of life. The Loess regression function suggests that males with ICLP appear on average somewhat shorter compared to peers until the age of 30, after which they appear somewhat taller.

Height trajectories for NC males (open circles, solid line) and males with ICLP (shaded circles, dashed line). ICLP, isolated cleft lip and/or palate; NC, normal comparison.
Discussion
Individuals with ICLP are often found to be of shorter stature relative to peers, and because orofacial clefts may pose a risk for abnormal pituitary development (30), this study assessed growth and pituitary volume in individuals with and without ICLP. In line with previous research, we found that individuals with ICLP were significantly shorter relative to peers (10,11) and that males with ICLP had lower BMI (16). Furthermore, we replicated findings of linear increase in pituitary volume over time in the NC groups (22,24,25,26,31). Finally, the results demonstrated that there are no gross morphological differences in pituitary volume in individuals with ICLP.
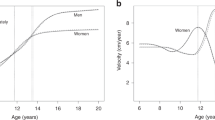
Height comparisons between individuals with and without ICLP revealed small but significant differences, showing that those with ICLP are somewhat shorter relative to healthy peers. Some have speculated that the long-term outcomes may be different for males and females with ICLP (15). Specifically, because prepubescent boys with ICLP showed higher than average growth velocity rates relative to peers, it was hypothesized that males with ICLP eventually catch up in height. In contrast, girls with ICLP were found to have lower than average growth velocity rates and were therefore thought to be less likely to catch up (15). The findings of our study complement these speculations by showing that males with ICLP catch up in their early 30s, whereas females likely remain shorter, as indicated by the significant difference in the regression slopes for height between females with and without ICLP.
The relatively subtle differences in height between individuals with and without ICLP could be conceptualized by two different distributions, where the distribution for the ICLP group is shifted to the left ( Figure 4 ). In this scenario, many individuals with ICLP fall within normal height ranges, or are only slightly different from normal-developing individuals. At the same time, however, individuals with ICLP are also more likely to fall within the extreme tail of the distribution of normal-developing individuals. In other words, although most of the time differences may be subtle, as a group, individuals with ICLP are more likely to suffer from more severe conditions relative to normal-developing individuals. An example of this phenomenon is extreme short stature, which is more common in individuals with ICLP relative to the normal population (8,27).

Hypothetical height distributions for NC individuals (solid outline) and individuals with ICLP (dashed outline). If the distribution of height for the ICLP group is shifted to the left, individuals with ICLP would be more likely to suffer from extreme growth problems (gray area) as compared with the NC group (black area). ICLP, isolated cleft lip and/or palate; NC, normal comparison.
On a final note, there is some evidence that cleft phenotype plays an important role in terms of height (16), although findings in this regard are not consistent (11,32,33). This notion is important in view of the different genetic mechanisms and embryology underlying various phenotypes of clefting (34). Unfortunately, our sample size was considered too small to do reliable comparisons between different cleft types within males and females. The literature would greatly benefit from a systematic study on long-term outcomes of growth in various phenotypes, as well as the (potentially differential) role of the pituitary.
BMI was also examined in this study and in line with results reported by others (16,32), our results showed that males with ICLP had lower BMI compared to peers, whereas females did not differ in terms of BMI (32). In males with ICLP, BMI appeared to remain low throughout development (16), although we could not directly test this, as weight was not collected for the adult sample. It is interesting that BMI was not lower in females with ICLP (32), despite the fact that they were significantly shorter than peers. Very little is known about BMI in females with ICLP; therefore, more research into this topic is necessary.
A major aim of this study was to examine pituitary volume, and although there were subtle differences in height between the ICLP groups and the NC groups, we did not see differences in terms of mean pituitary volume or pituitary trajectories. The age-by-pituitary regression lines were somewhat weaker for the ICLP groups, but not significantly so. A caveat of this study is the relatively low power because of small sample size, which increases the likelihood of false-negative findings, i.e., type II error. There is a chance that the pituitary is abnormal in ICLP but our study may have failed to reject the null hypothesis given our sample size. It is therefore important to replicate the findings in a larger sample. Our tentative conclusion is that gross pituitary volume appears normal in individuals with ICLP. This interpretation was underscored by resampling the data using a bootstrap procedure, in which we observed that only 1.08% of 50,000 iterations for males and 3.02% of these iterations for females had a significance level of <0.1. These results suggest that there is a low probability that the groups are actually different, making us more confident in the lack of group differences. It should be noted, however, that our imaging methods allowed for only relatively coarse comparisons. That is, although the groups did not differ in terms of gross pituitary volume, more subtle differences may remain. For example, abnormal shape of the pituitary, abnormal growth hormone secretion, or molecular abnormalities could be involved as well. Given the importance of the pituitary in growth and the fact that orofacial clefts may pose a risk for abnormal pituitary development (29), future research should continue to explore the role of the pituitary in relation to growth in this population.
Conclusion
Although individuals with ICLP were found to be shorter and had lower BMI (males only), their pituitaries appeared to develop normally. However, this does not necessarily mean that the pituitary is not involved in subtle differences in height and BMI in ICLP. As mentioned earlier, more subtle factors as opposed to gross morphological differences may account for the observed differences in height between individuals with and without ICLP, and this should be examined in future research.
Of note, growth problems in children with clefts are not confined to height, as delays are reported for the musculoskeletal system (4,13), dental development (35), and brain development (12,36,37,38). Birth defects often affect a combination of organs, and a triad of defects in the craniofacial region, the central nervous system, and the musculoskeletal system is particularly common (4,39). This is likely due to the shared ectodermal origins of these systems, or a result of the interplay between the ectoderm and mesoderm (5,39). Children with ICLP are more likely to suffer from a general developmental delay that affects multiple organ systems (39). Abnormalities in one system should therefore be evaluated in the context of possible multiple systems. Adopting an integrated view would contribute to a more comprehensive understanding of growth delays in individuals with ICLP.
Methods
Participants—Youth Sample
Individuals with ICLP were recruited from the Cleft Lip/Palate Clinic at the University of Iowa Hospital and Clinics, whereas the comparison groups were recruited from the community via newspaper announcements. Both individuals with ICLP and NCs were recruited in the same geographic area in Iowa. Average family income and education level for residents of Iowa are very close to the means for the US population (http://www.quickfacts.census.gov). In other words, demographically Iowa can be considered an average state. However, the ethnic makeup of Iowa is skewed toward a large proportion of individuals of European descent (91.3%), which is well above the US mean (72.4%).
Males. Height and BMI measures were obtained from 49 males with ICLP in the age range of 7.7–21.8 y (mean age 13.65, SD = 4.0). A total of six males were seen twice, adding up to 55 observations. Because there appear to be no growth problems in individuals with clefts of the lip only (10,11), only individuals with cleft lip and palate (CLP) and CPO were included. In the current sample, 13 males had CPO, and 36 males had CLP. Height was obtained in centimeters, and BMI was calculated as follows:

Males with ICLP were compared to 121 developmentally NC males in the age range of 6.7–24.1 y (mean age 12.80, SD = 3.6). A total of 11 males from this pool were seen twice, adding up to 132 observations ( Table 3 ). Please note that height measures of 39 males with ICLP and 50 NC males in this sample were previously reported (12).
Females. Height and BMI measurements were taken from 30 females with ICLP in the age range of 7.5–22.9 y (mean age 14.7, SD = 4.1). One female with ICLP was seen twice, adding up to 31 observations. Sixteen of these females had CPO and 14 females had CLP.
Females with ICLP were compared to 158 developmentally normal females in the age range of 6.0–22.2 y (mean age 12.70, SD = 3.7). A total of 14 females from this pool were seen twice, adding up to 172 observations. Please note that height measures of 18 females with ICLP and 24 NC females in this sample were previously reported (12).
MRI scans were obtained from the entire sample of individuals with ICLP; however, only a subset of the NC group had undergone MRI scanning with similar magnet strength to that of the ICLP group. Specifically, 65 NC males had undergone compatible MRI scanning, and seven males were seen twice, adding up to 72 observations. In addition, compatible MRI scans were obtained from 60 NC females. A total of six females were seen twice, adding up to 66 observations ( Table 3 ).
Participants—Adult Sample
The adult sample was collected from 1992 to 1999 and consisted of 46 males with ICLP (32 had CLP and 14 had CPO) and 46 age-matched comparisons, in the age range of 18–50 y (36). Individuals with ICLP were recruited from the University of Iowa Cleft Clinic, and healthy comparisons were recruited via local newspapers. As with the youth sample, individuals with ICLP and healthy comparisons were all recruited in the same geographic area.
This sample was used for height measures only, as pituitary and weight measures were not available. Also, the sample was limited to males, thus no data in older females with ICLP are available to assess long-term trajectory of growth for the female sample.
Before participating in this study, all participants were screened by a research assistant. In both groups, participants were excluded if they had braces, or if a serious medical or neurological disease was present. In addition, NC participants were excluded if they had a history of a learning disorder or psychiatric disorder.
The study was approved by the University of Iowa Human Subjects Institutional Review Board. If the participant was under the age of 13, written consent was obtained from one parent and assent was obtained from the participant. Participants age 13 and above provided their own consent.
Structural Imaging
All scans were performed using a 1.5 Tesla scanner. In the years 2002 and 2005, 170 scans were obtained from a SIGNA System (General Electric, Waukesha, WI). Since this scanner was replaced in 2006, the remaining 54 scans were obtained from an Avanto scanner (Siemens, Erlangen, Germany) using the same acquisition protocol. Comparison of the volumes obtained between the two machines produced comparable measures (40). Three-dimensional T1-weighted 1.5-mm coronal images were acquired. Proton-density and T2-weighted images were also acquired. MRI data were processed using BRAINS2 (Brain Research: Analysis of Images, Networks, and Systems (41)).
Pituitary Segmentation
All images were loaded in BRAINS2, and the pituitary was traced manually by A.M.A., who established intrarater reliability on a separate set of 10 subjects (intraclass R coefficient .99). The neuroanatomical boundaries of the pituitary were determined by reference to a neuroanatomical atlas (42). The carotid artery and the optic chiasm were used as landmarks to identify the boundaries of the pituitary. The rater was blind to participant’s diagnosis.
Statistical Methods
First, t-tests were used for comparisons of mean height, BMI, and pituitary volume between individuals with and without ICLP. The analyses were performed separately for males and females. In addition, mixed-model analysis of covariance was used to compare the variables between groups while adjusting for the effects of age and repeated measures. Each mixed model treated research ID number as a random effect, because the time between first and second visits varied between participants. The parameter estimates from the mixed models were also used to calculate correlations between age and the dependent measures for each group, such that trajectories could be examined.
Finally, a Loess curve was fitted to the combined adult and youth male samples. This nonparametric method, which is based on locally weighted regression, uses a smoothing function to fit a regression surface to the data (43). It was used in this setting as an exploratory graphing tool.
Because of small sample sizes, analyses of potential differences between individuals with CPO and CLP were not conducted.
Statement of Financial Support
This study was funded by the National Institute of Dental and Craniofacial Research.
References
Canfield MA, Honein MA, Yuskiv N, et al. National estimates and race/ethnic-specific variation of selected birth defects in the United States, 1999-2001. Birth Defects Res Part A Clin Mol Teratol 2006;76:747–56.
Vieira AR . Unraveling human cleft lip and palate research. J Dent Res 2008;87:119–25.
Jones MC . Etiology of Facial Clefts – Prospective Evaluation of 428 Patients. Cleft Palate Craniofac J 1988;25:16–20.
Calzolari E, Pierini A, Astolfi G, Bianchi F, Neville AJ, Rivieri F . Associated anomalies in multi-malformed infants with cleft lip and palate: An epidemiologic study of nearly 6 million births in 23 EUROCAT registries. Am J Med Genet A 2007;143:528–37.
Schoenwolf GC, Bleyl SB, Brauer PR, Francis-West PH . Larsen’s Human Embryology, 4th edn. Philadelphia, PA: Churchill Livingstone, 2009.
Mittwoch U . Different gene expressions on the left and the right: a genotype/phenotype mismatch in need of attention. Ann Hum Genet 2008;72(Pt 1):2–9.
Lipman TH, Rezvani I, Mitra A, Mastropieri CJ . Assessment of stature in children with orofacial clefting. MCN Am J Matern Child Nurs 1999;24:252–6.
Rudman D, Davis T, Priest JH, et al. Prevalence of growth hormone deficiency in children with cleft lip or palate. J Pediatr 1978;93:378–82.
Ranalli DN, Mazaheri M . Height-weight growth of cleft children, birth to 6 years. Cleft Palate Craniofac J 1975;12:400–4.
Jensen BL, Kreiborg S, Dahl E, Foghandersen P . Cleft-lip and palate in Denmark, 1976-1981: epidemiology, variability, and early somatic development. Cleft Palate Craniofac J 1988;25:258–69.
Felix-Schollaart B, Hoeksma JB, Prahl-Andersen B . Growth comparison between children with cleft lip and/or palate and controls. Cleft Palate Craniofac J 1992;29:475–80.
Nopoulos P, Langbehn DR, Canady J, Magnotta V, Richman L . Abnormal brain structure in children with isolated clefts of the lip or palate. Arch Pediatr Adolesc Med 2007;161:753–8.
Jensen BL, Dahl E, Kreiborg S . Longitudinal study of body height, radius length and skeletal maturity in Danish boys with cleft lip and palate. Scand J Dent Res 1983;91:473–81.
Hunter WS, Dijkman DJ . The timing of height and weight deficits in twins discordant for cleft of the lip and/or palate. Cleft Palate J 1977;14:158–66.
Cunningham ML, Jerome JT . Linear growth characteristics of children with cleft lip and palate. J Pediatr 1997;131:707–11.
Persson M, Becker M, Svensson H . Physical characteristics of young men with cleft lip, with or without cleft palate, and cleft palate only. Scand J Plast Reconstr Surg Hand Surg 2007;41:6–9.
Smedegaard L, Marxen D, Moes J, Glassou EN, Scientsan C . Hospitalization, breast-milk feeding, and growth in infants with cleft palate and cleft lip and palate born in Denmark. Cleft Palate Craniofac J 2008;45:628–32.
Turner L, Jacobsen C, Humenczuk M, Singhal VK, Moore D, Bell H . The effects of lactation education and a prosthetic obturator appliance on feeding efficiency in infants with cleft lip and palate. Cleft Palate Craniofac J 2001;38:519–24.
Blumenfeld H . Neuroanatomy Through Clinical Cases. Sunderland, MA: Sinauer Associates, 2002.
Isaksson OG, Jansson JO, Gause IA . Growth hormone stimulates longitudinal bone growth directly. Science 1982;216:1237–9.
Bengtsson BA, Edén S, Lönn L, et al. Treatment of adults with growth hormone (GH) deficiency with recombinant human GH. J Clin Endocrinol Metab 1993;76:309–17.
Marziali S, Gaudiello F, Bozzao A, et al. Evaluation of anterior pituitary gland volume in childhood using three-dimensional MRI. Pediatr Radiol 2004;34:547–51.
Argyropoulou M, Perignon F, Brunelle F, Brauner R, Rappaport R . Height of normal pituitary gland as a function of age evaluated by magnetic resonance imaging in children. Pediatr Radiol 1991;21:247–9.
Takano K, Utsunomiya H, Ono H, Ohfu M, Okazaki M . Normal development of the pituitary gland: assessment with three-dimensional MR volumetry. AJNR Am J Neuroradiol 1999;20:312–5.
Fink AM, Vidmar S, Kumbla S, et al. Age-related pituitary volumes in prepubertal children with normal endocrine function: volumetric magnetic resonance data. J Clin Endocrinol Metab 2005;90:3274–8.
MacMaster FP, Keshavan M, Mirza Y, et al. Development and sexual dimorphism of the pituitary gland. Life Sci 2007;80:940–4.
Laron Z, Taube E, Kaplan I . Pituitary growth hormone insufficiency associated with cleft lip and palate. An embryonal developmental defect. Helv Paediatr Acta 1969;24:576–81.
Triulzi F, Scotti G, di Natale B, et al. Evidence of a congenital midline brain anomaly in pituitary dwarfs: a magnetic resonance imaging study in 101 patients. Pediatrics 1994;93:409–16.
Lipinski RJ, Song C, Sulik KK, et al. Cleft lip and palate results from Hedgehog signaling antagonism in the mouse: Phenotypic characterization and clinical implications. Birth Defects Res Part A Clin Mol Teratol 2010;88:232–40.
Roitman A, Laron Z . Hypothalamo-pituitary hormone insufficiency associated with cleft lip and palate. Arch Dis Child 1978;53:952–5.
Arslanoglu I, Kutlu H, Isgüven P, Tokus F, Isik K . Diagnostic value of pituitary MRI in differentiation of children with normal growth hormone secretion, isolated growth hormone deficiency and multiple pituitary hormone deficiency. J Pediatr Endocrinol Metab 2001;14:517–23.
Bowers EJ, Mayro RF, Whitaker LA, Pasquariello PS, LaRossa D, Randall P . General body growth in children with clefts of the lip, palate, and craniofacial structure. Scand J Plast Reconstr Surg Hand Surg 1987;21:7–14.
Lee J, Nunn J, Wright C . Height and weight achievement in cleft lip and palate. Arch Dis Child 1997;76:70–2.
Murray JC . Gene/environment causes of cleft lip and/or palate. Clin Genet 2002;61:248–56.
Hazza’a AM, Rawashdeh MA, Al-Jamal G, Al-Nimri KS . Dental development in children with cleft lip and palate: a comparison between unilateral and bilateral clefts. Eur J Paediatr Dent 2009;10:90–4.
Nopoulos P, Berg S, Canady J, Richman L, Van Demark D, Andreasen NC . Structural brain abnormalities in adult males with clefts of the lip and/or palate. Genet Med 2002;4:1–9.
Nopoulos P, Richman L, Andreasen NC, Murray JC, Schutte B . Abnormal brain structure in adults with Van der Woude syndrome. Clin Genet 2007;71:511–7.
van der Plas E, Conrad A, Canady J, Richman L, Nopoulos P . Effects of unilateral clefts on brain structure. Arch Pediatr Adolesc Med 2010;164:763–8.
Mueller AA, Sader R, Honigmann K, Zeilhofer HF, Schwenzer-Zimmerer K . Central nervous malformations in presence of clefts reflect developmental interplay. Int J Oral Maxillofac Surg 2007;36:289–95.
Nopoulos P, Magnotta VA, Mikos A, Paulson H, Andreasen NC, Paulsen JS . Morphology of the cerebral cortex in preclinical Huntington’s disease. Am J Psychiatry 2007;164:1428–34.
Magnotta VA, Harris G, Andreasen NC, O’Leary DS, Yuh WT, Heckel D . Structural MR image processing using the BRAINS2 toolbox. Comput Med Imaging Graph 2002;26:251–64.
Mills CM, De Groot J, Posin JP . Magnetic resonance imaging: Atlas of the head, neck and spine. Philadelphia, PA: Lea and Febiger, 1987.
Cleveland WS . Robust locally weighted regression and smoothing scatterplots. J Am Stat Assoc 1979;74:829–36.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
van der Plas, E., Caspell, C., Aerts, A. et al. Height, BMI, and pituitary volume in individuals with and without isolated cleft lip and/or palate. Pediatr Res 71, 612–618 (2012). https://doi.org/10.1038/pr.2012.12
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pr.2012.12
This article is cited by
-
Three-dimensional assessment of the sella turcica: comparison between cleft lip and palate patients and skeletal malocclusion classes
Surgical and Radiologic Anatomy (2020)
