
Abstract
The healthcare system in Korea provides coverage to all the people who are residing in Korea, so the data of the Korea healthcare system are national-wide and relatively accurate. We obtained the recent 5-year data (2004–2008) on the treatment of BPH from the national health insurance system. We tried to determine the trends or changes of BPH treatments in Korea. Over 3.8 million men visited clinics and were prescribed one or more BPH medications, and more than 44 000 men underwent surgical treatment during 2004–2008. Compared with the year 2004, two times the patients were prescribed BPH medications in 2008. With respect to the surgical treatment, the number of cases was increased 1.6 times in 2006 compared with the previous years. The most commonly used surgical option was TURP before 2006, but laser therapy was carried out as much as TURP in 2006 and in the following years. The relative risk of laser therapy in the 50 s is 1.53 (95% CI is 1.47–1.59). In conclusion, our national-wide data for the Korean BPH patients show that these patients’ medical treatment increased during the 5 years from 2004 to 2008. Laser treatment had increased and it might replace TURP in several years.
Similar content being viewed by others

Introduction
BPH is defined clinically as a condition that is characterized by the combination of an enlarged prostate and lower urinary tract symptoms (LUTS). These symptoms are variable and can have a significant negative impact on the quality of life, leading many men to seek a physician.1
In the United States, ∼4.5 million visits were made to physicians’ offices for a primary diagnosis of BPH and almost 8 million visits were made with a primary or secondary diagnosis of BPH.2 In Korea, the prevalence of clinical BPH in a community-base study of Chungbuk province was 27.7%, using the definition of BPH that combined a prostate volume ⩾20 cm3 and IPSS ⩾8.3
Medical treatment is thought to be first-line therapy in men with symptomatic BPH.4 Several alpha blockers and 5 alpha reductase inhibitors are widely used for treatment of BPH. As for surgical treatment, TURP was gold standard, but laser prostatectomy showed comparable results to conventional TURP.5 But there is no recently published data of whole national-wide investigation about treatment of BPH.
The healthcare system in Korea provides coverage to all its citizens and it is comprehensively managed in the form of social insurance. It has two components, health insurance and medical aid, which is free medical care for the lower-income groups. The former is funded by beneficiaries’ contributions according to their incomes and the latter is funded by general revenue. Therefore the data of the Korea healthcare system are national wide and relatively accurate as compared with other resources. We obtained the recent 5-year data of BPH treatment courtesy of the Health Insurance Review and Assessment Service (HIRA) in Korea.
We analyzed the medical and surgical treatments for the Korean BPH patients from HIRA data. We tried to determine that what age group was most rapidly increased in visiting physicians for treatment of BPH and whether there are any trends or changes of BPH treatments during 5 years. And we also assessed whether laser therapy was conducted as many as TURP after being introduced in Korean insurance system.
Materials and methods
This study was exempted from evaluation by the institutional review board of the Boramae medical center.
We obtained the data from 2004 to 2008 from the HIRA. The data of the code N40, which indicate BPH, from the National Center for Health Statistics International Classification of Diseases, 9th revision (ICD-9) was included. It contained various parameters: the year, age and regions where the men had visited to the clinic, the medication categories they had been prescribed and the surgical treatment they had received. Age was divided by decades, and the regions were divided into seven metropolises, including Seoul, and nine provinces by administrative divisions of Korea. Each province included several small cities and rural areas. Four kinds of drugs such as alpha-blockers, 5 alpha-reductase inhibitors, anti-cholinergics and antidiuretics are currently being used in Korea. Alpha-blockers included alfuzosin ER (extended release), doxazocin gastrointestinal therapeutic system, tamsulosin and terazosin, the 5 alpha reductase inhibitors were dutasteride and finasteride, and the anti-cholinergics were flavoxate, oxybutynin XL, propiverine and tolterodine ER. The available antidiuretic was only one formulation called desmopressin.
Nocturia is one of most bothersome symptoms in patients with BPH and can have a marked impact on quality of life. In some study, alpha-blocker monotherapy resulted in both a subjective and objective improvement of nocturia in men with LUTS.6 Oral desmopressin had effects in patients with BPH especially for nocturnal polyuria.7 So desmopressin was included for medical treatment modality in our study.
Four kinds of surgeries were included in our data: TURP, open prostatectomy, hyperthermia and laser therapy. Hyperthermia therapy of the prostate included transurethral needle ablation (TUNA), Prostron, Thermex, Microfocus, Prosta and so on. Laser therapy of the prostate was mainly KTP photoselective vaporization of the prostate.
The number of each surgical case and the number of patients received BPH medication were analyzed using Poisson's regression model, respectively. Relative risks of the surgical cases were estimated by year and age from each surgical treatment. The relative risk (RR) of the number of patient received BPH medication by year was estimated, which was adjusted by age, drug, clinic and region. The RRs were obtained by taking the exponential of the parameter estimates in the Poisson's models. The significance of the RRs was determined using the Wald test statistic by using the estimated variance-covariance matrix. A significance of interaction between two significant factors in any Poisson's model was tested. All hypotheses were evaluated in a two-sided manner, and P-values of <0.05 were considered significant.
Results
More than 760 000 men annually visited medical facilities and they were prescribed medications for BPH, and more than 44 000 men underwent surgical treatment such as TURP, open prostatectomy, hyperthermia and laser therapy in 2004–2008. For the 5 years, over 3.8 million men visited health care centers and were prescribed one or more BPH medication. The number of patients who were prescribed BPH medications in 2008 was increased almost two times compared with that in 2004 (Table 1). In their 30 s, there is no annual increase in the number of patients who were prescribed BPH medications. The BPH medications were categorized as alpha-blockers, 5 alpha reductase inhibitors, anti-cholinergics and antidiuretics. The numbers of patients who were prescribed BPH medications of the first three categories were increased two times in 2008 as compared with that in 2004. And antidiuretics such as desmopressin were used 14 times more in 2008 as compared with that in 2004 (Table 2).
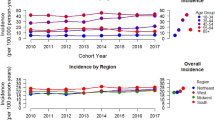
After a Poisson’s regression analysis, we found that BPH medications were depending on age groups, years (P<0.0001). Poisson’s regression analysis showed that the interaction between age and study year was significant (P<0.0001). It means that the variation of BPH medications by years was significantly different depending on the age groups. The estimated RR is shown in Figure 1. In the age of 70 s, the number of patients was most rapidly increased compared with previous year. The RRs of alpha-blockers were 1.0297 (95% CI: 1.0291–1.0302), 1.1448 (95% CI: 1.1447–1.1.1449), 1.1666 (95% CI: 1.1666–1.1666), 1.1596 (95% CI: 1.1596–1.597), 1.222 (95% CI: 1.2220–1.2221) and 1.1831 (95% CI: 1.1830–1.1832) in their 30 s, 40 s, 50 s, 60 s, 70 s and 80 s, respectively.

Estimated relative risks (RRs) of patients number according to age group, compared with the previous year. ARI, alpha reductase inhibitors.
With respect to the surgical treatments, the number of cases was increased 1.6 times in 2006 compared with the previous years, and a similar number of cases was maintained in the following years. The most commonly used surgical option was TURP before 2006, but laser therapy such as photoselective vaporization was carried out as much as TURP in 2006 and in the following years (Table 3). In Korea, laser therapy of BPH was not under coverage of medical insurance system before 2006, so our data showed that laser therapy was not conducted until 2005. Among the age groups, the patients in their 60 s most often underwent surgical treatment (Table 3), but patients in their 70 s showed most rapid increase in receiving surgical treatment (Table 4). The RRs of TURP were 1.0472 (95% CI: 0.9392–1.1675), 1.0319 (95% CI: 0.9998–1.0650), 0.9962 (95% CI: 0.9812–1.0114), 1.0867 (95% CI: 1.0690–1.1046) and 1.0753 (95% CI: 1.0412–1.1105) in their 40, 50, 60, 70 and 80 s, respectively, compared with the previous year. And those who underwent laser therapy increased 1.53 times in their 50 s compared with the previous year (Table 4).
Discussions
The National Health Insurance (NHI) program of Korea covers all the people who are residing in the territory of the Republic of Korea since 1989. As a compulsory social insurance system, its main sources of finance are contributions from the insured and government subsidy. It took just 12 years for the Korean government to achieve universal coverage after the implementation of a mandatory medical insurance program for workplaces with 500 employees or more in 1977. The Minister of Health and Welfare oversees the national health insurance system. The National Health Insurance Corporation (NHIC) serves as the insurer and the HIRA conducts reviews and assessment of medical fees. ‘Fee for Service’ has been the traditional reimbursement system. As a single payer, the NHIC is responsible for the NHI program’s operation and management.
The NHI system has greatly contributed to improving the quality of life of the public by ensuring low-cost access to healthcare. As a result, Korean society has enjoyed much better health outcomes in terms of life expectancy and infant mortality. According to the National Statistical Office of Korea, life expectancy in 2010 is expected to average 79 years, ranking 22nd in the world. NHI covers all the people, even foreign workers, who are residing in Korea. So the data from the NHI are national wide and more accurate than any other data.
BPH is the non-malignant enlargement of the prostate gland. Clinically, BPH leads to voiding dysfunction, which is most often referred to LUTS.8 BPH and LUTS are common in men 40 years or older and they increase with age. In 2000, the number of outpatient visits for BPH was 14 473/100 000 from the data of the Urologic Diseases in America BPH project.2 Approximately 4.5 million visits were made to physician offices for a primary diagnosis of BPH and almost 7.7 million visits were made with a primary or secondary diagnosis of BPH in 2000.2 According to that report, there was more than a 1.5-fold increase in the number of outpatients’ visits in 2000 compared with 1994. According to our data, over 1 million patients were prescribed BPH medications in 2008, and there was almost a two times increase compared with that in the year 2004. This was thought to be because of Korea’s specific situation such as the rapid change to an aged society, the westernization of eating habits and so on. According to the National Statistical Office of Korea, the population of those aged 65 or older increased by 33 percent to about 4.36 million, only 5 years after it first exceeded 3 million. At this pace, Korean society is expected to become a so-called ‘aged society’ by 2013, only 13 years after its designation as an ‘aging society’ in 2000. It is more rapid than that of other countries such as France, the US and even Japan.
According to our data, in their 30 s there was no increase in the prevalence of medical therapy. Contrary to other age group, prescription of alpha blockers might be mostly directed to chronic pelvic pain syndrome not to BPH. So in our national-wide BPH data, annual prevalence of prescription was about 1% and no increase in the 30 s.
Nocturia is one of the most bothersome symptoms among LUTS, and has been reported to respond less satisfactory to treatment than do other LUTS.9 Nocturnal polyuria is an important cause of nocturia that may result from age-related fluctuations in the serum levels of the antidiuretic hormone arginine vasopressin.10 Advancing age is also associated with increased nighttime excretion of water, solutes and electrolytes.11, 12 So, the synthetic antidiuretic hormone desmopressin is an effective and well-tolerated treatment for nocturia in men.10, 13 In Korea, a small clinical trial was reported on the effects of desmopressin for nocturia in 1999.14 But it was not widely used before 2004, because the Korea NHI system did not permit physicians to prescribe desmopressin for adult nocturia. After permission in 2004, the number of desmopressin prescriptions has gradually increased. Desmopressin was used more than 14 times more often in 2008 as compared with that in 2004, but its usage was a small portion compared with alpha-blocker usage.
As for surgical treatment of BPH, laser prostatectomy, especially photoselective vaporization has steadily gained clinical utility and become good alternative to TURP.15, 16
In Korea, laser prostatectomies were increasingly used for the treatment of BPH since NHI system approved of photoselective vaporization for the treatment of BPH in 2006. Before 2006, laser prostatectomies were conducted by some urologists in a few patients. But that data might be a small portion and were not captured because HIRA did not reimburse these services, so our data showed that laser therapy was zero before 2006. In 2007, laser prostatectomies were conducted more than TURP. Among the laser prostatectomies, KTP vaporization of the prostate accounted for the most portion of surgical treatments. Holmium enucleation of prostate was approved in 2009 by NHI program of Korea, so laser prostatectomies would be more frequently carried out recently. Although conventional KTP was not so good for large BPH,17, 18 the new modalities such as 120W high power system and holmiun laser enucleation of the prostate may overcome, and be preferred option in huge BPH patients instead of TURP or open prostatectomy.19, 20 We think laser prostatectomies might gradually replace TURP or open prostatectomy in several years later.
The men in their 60 s were most commonly prescribed BPH medications and they underwent surgery during the 5 years. That would be explained sociodemographically that in Korea, the population in their 60 s is larger than the population in both their 70 s and the 80 s. The men in their 60 s may more actively seek health care than the other age groups. Some other reports showed similar results that the men in their 60 s more frequently visited to surgery centers and they complained of more severe LUTS.2, 21
But increase rate was most rapid in the age of 70 s both in medical and surgical treatment. So we think that more patients in their 70 s will be prescribed BPH drug and undergo BPH surgery in several years later.
Our study has several limitations. Although we obtained the nation-wide comprehensive data, it lack the detailed patient information of the BPH status such as the symptom severity, the co-morbidities and so on. Complementary alternative medicine such as saw palmetto is widely used, but it is not under the coverage of the Korea NHI system. So its data were not included in our medical treatment data.
In conclusion, our national-wide data for the Korean BPH patients showed that the patients who received medical treatment increased during the 5 years. Compared with medical treatments, surgical treatment did not so much increase. But laser treatment increased and it might replace TURP in several years in Korea.
References
Jacobsen SJ, Guess HA, Panser L, Girman CJ, Chute CG, Oesterling JE et al. A population-based study of health care-seeking behavior for treatment of urinary symptoms. the olmsted county study of urinary symptoms and health status among men. Arch Fam Med 1993; 2: 729–735.
Wei JT, Calhoun E, Jacobsen SJ . Urologic diseases in america project: benign prostatic hyperplasia. J Urol 2005; 173: 1256–1261.
Lee HL, Seo JW, Kim WJ . The prevalence of benign prostatic hyperplasia: community-base study in Chungbuk province. Korean J Urol 1999; 40: 1500–1505.
Gonzalez RR, Kaplan SA . First-line treatment for symptomatic benign prostatic hyperplasia: is there a particular patient profile for a particular treatment? World J Urol 2006; 24: 360–366.
Bouchier-Hayes DM . Photoselective vaporization of the prostate—towards a new standard. Prostate Cancer Prostatic Dis 2007; 10: S10–S14.
Paick JS, Ku JH, Shin JW, Yang JH, Kim SW . Alpha-blocker monotherapy in the treatment of nocturia in men with lower urinary tract symptoms: a prospective study of response prediction. BJU Int 2006; 97: 1017–1023.
Wang CJ, Lin YN, Huang SW, Chang CH . Low dose oral desmopressin for nocturnal polyuria in patients with benign prostatic hyperplasia: a double-blind, placebo controlled, randomized study. J Urol 2011; 185: 219–223.
Bullock TL, Andriole Jr GL . Emerging drug therapies for benign prostatic hyperplasia. Expert Opin Emerg Drugs 2006; 11: 111–123.
Homma Y, Yamaguchi T, Kondo Y, Horie S, Takahashi S, Kitamura T . Significance of nocturia in the International Prostate Symptom Score for benign prostatic hyperplasia. J Urol 2002; 167: 172–176.
Mattiasson A, Abrams P, Van Kerrebroeck P, Walter S, Weiss J . Efficacy of desmopressin in the treatment of nocturia: a double-blind placebo-controlled study in men. BJU Int 2002; 89: 855–862.
Kirkland JL, Lye M, Levy DW, Banerjee AK . Patterns of urinary flow and electrolyte excretion in healthy elderly people. Br Med J 1983; 287: 1665–1667.
Matthiesen TB, Rittig S, Nørgaard JP, Pedersen EB, Djurhuus JC . Nocturnal polyuria and natriuresis in male patients with nocturia and lower urinary tract symptoms. J Urol 1996; 156: 1292–1299.
van Kerrebroeck P, Rezapour M, Cortesse A, Thüroff J, Riis A, Nørgaard JP . Desmopressin in the treatment of nocturia: a double-blind, placebo-controlled study. Eur Urol 2007; 52: 221–229.
Lee GH, Kim JC, Suh HJ, Kim HW, Hwang TG . The effect of desmopressin in nocturia. Korean J Urol 1999; 40: 613–616.
Te AE . Current state of the art photoselective vaporization prostatectomy: laser therapy for benign prostatic hyperplasia. Prostate Cancer and Prostatic Dis 2007; 10: S2–S5.
Ruszat R, Wyler SF, Seitz M, Lehmann K, Abe C, Bonkat G et al. Comparison of potassium-titanyl-phosphate laser vaporization of the prostate and transurethral resection of the prostate: update of a prospective non-randomized two-centre study. BJU Int 2008; 102: 1432–1438.
Horasanli K, Silay MS, Altay B, Tanriverdi O, Sarica K, Miroglu C . Photoselective potassium titanyl phosphate (KTP) laser vaporization versus transurethral resection of the prostate for prostates larger than 70 ml: a short-term prospective randomized trial. Urology 2008; 71: 247–251.
Pfitzenmaier J, Gilfrich C, Pritsch M, Herrmann D, Buse S, Haferkamp A et al. Vaporization of prostates of ⩾80 ml using a potassium-titanyl-phosphate laser: midterm-results and comparison with prostates of <80 ml. BJU Int 2008; 102: 322–327.
Dusing MW, Krambeck AE, Terry C, Matlaga BR, Miller NL, Humphreys MR et al. Holmium laser enucleation of the prostate: efficiency gained by experience and operative technique. J Urol 2010; 184: 635–640.
Geavlete P, Niţã G, Geavlete B . Initial Romanian experience with green light HPS 120 w laser in BPH. J Med Life 2008; 1: 454–460.
Hoke GP, McWilliams GW . Epidemiology of benign prostatic hyperplasia and comorbidities in racial and ethnic minority populations. Am J Med 2008; 121 (Suppl 2): S3–10.
Acknowledgements
We appreciate the statistical analyses provided by Medical Research Collaborating Center, Seoul National University College of Medicine, Seoul National University Hospital.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
This work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Kang, J., Min, G., Son, H. et al. National-wide data on the treatment of BPH in Korea. Prostate Cancer Prostatic Dis 14, 243–247 (2011). https://doi.org/10.1038/pcan.2011.12
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/pcan.2011.12
Keywords
This article is cited by
-
Free combination of dutasteride plus tamsulosin for the treatment of benign prostatic hyperplasia in South Korea: analysis of drug utilization and adverse events using the National Health Insurance Review and Assessment Service database
BMC Urology (2021)
-
Impact of different color fiber sleeves on beam hazards of 532-nm laser and vaporization efficiency
Lasers in Medical Science (2019)
