
Abstract
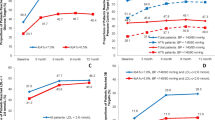
We did not find any paper that assessed clinical inertia in obese patients. Therefore, no paper has compared the clinical inertia rates between morbidly and nonmorbidly obese patients. A cross-sectional observational study was carried out. We analysed 8687 obese patients ⩾40 years of age who attended their health-care center for a checkup as part of a preventive program. The outcome was morbid obesity. Secondary variables were as follows: failure in the management of high blood pressure (HBP), high blood cholesterol (HBC) and high fasting blood glucose (HFBG); gender; personal history of hypertension, dyslipidemia, diabetes, smoking and cardiovascular disease; and age (years). We analysed the association between failures and morbid obesity by calculating the adjusted odds ratio (OR). Of 8687 obese patients, 421 had morbid obesity (4.8%, 95% confidence interval (CI): 4.4–5.3%). The prevalence rates for failures were as follows: HBP, 34.7%; HBC, 35.2%; and HFBG, 12.4%. Associated factors with morbid obesity related with failures were as follows: failure in the management of HBP (OR=1.42, 95% CI: 1.15–1.74, P=0.001); failure in the management of HBC (OR=0.73, 95% CI: 0.58–0.91, P=0.004); and failure in the management of HFBG (OR=2.24, 95% CI: 1.66–3.03, P<0.001). Morbidly obese patients faced worse management for HBP and HFBG, and better management for HBC. It would be interesting to integrate alarm systems to avoid this problem.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 digital issues and online access to articles
$119.00 per year
only $9.92 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

References
World Health Organization. Prevention of cardiovascular disease: guideline for assessment and management of cardiovascular risk [updated 2007; accessed October 2014]. Available from http://whqlibdoc.who.int/publications/2007/9789241547178_eng.pdf?ua=1.
Salas-Salvadó J, Rubio MA, Barbany M, Moreno B . Grupo Colaborativo de la SEEDO. Consenso SEEDO 2007 para la evaluación del sobrepeso y la obesidad y el establecimiento de criterios de intervención terapéutica. Med Clin (Barc) 2007; 128: 184–196.
Center for Disease Control and Prevention (CDC). Obesity: halting the epidemic by making health easier. [updated 2011; accessed October 2014]. Available from http://www.cdc.gov/chronicdisease/resources/publications/aag/pdf/2011/obesity_aag_web_508.pdf.
World Health Organization. BMI classification. [updated August 2014; accessed October 2014]. Available from http://apps.who.int/bmi/index.jsp?introPage=intro_3.html.
Phillips LS, Branch WT, Cook CB, Doyle JP, El-Kebbi IM, Gallina DL et al. Clinical inertia. Ann Intern Med 2001; 135: 825–834 Review.
Andrade SE, Gurwitz JH, Field TS, Kelleher M, Majumdar SR, Reed G et al. Hypertension management: the care gap between clinical guidelines and clinical practice. Am J Manag Care 2004; 10 (7 Pt 2): 481–486.
Sepehri A, Gil-Guillén VF, Palazón-Bru A, Orozco-Beltrán D, Carratalá-Munuera C, Castell EC et al. Are obese patients assisted in losing weight? Am J Manag Care 2014; 20: e122–e128.
Pedrera Carbonell V, Gil Guillén V, Prieto Erades I, Schwarz Chavarri G, Moya García I . Características de la demanda sanitaria en las consultas de medicina de familia de un área de salud de la Comunidad Valenciana. Aten Primaria 2005; 35: 82–88.
Gil-Guillén V, Orozco-Beltrán D, Pérez RP, Alfonso JL, Redón J, Pertusa-Martínez S et al. Clinical inertia in diagnosis and treatment of hypertension in primary care: quantification and associated factors. Blood Press 2010; 19: 3–10.
Aujoulat I, Jacquemin P, Rietzschel E, Scheen A, Tréfois P, Wens J et al. Factors associated with clinical inertia: an integrative review. Adv Med Educ Pract 2014; 5: 141–147.
Palazón-Bru A, Gil-Guillén VF, Orozco-Beltrán D, Pallarés-Carratalá V, Valls-Roca F, Sanchís-Domenech C et al. Is the physician's behavior in dyslipidemia diagnosis in accordance with guidelines? Cross-sectional ESCARVAL study. PLoS ONE 2014; 9: e91567.
Generalitat Valenciana: Conselleria de Sanitat. Estudio Valencia (II): prevalencia de obesidad, hipertensión arterial, dislipemia, tabaquismo y resistencia a la insulina. [updated 2010; accessed July 2013]. Available from http://publicaciones.san.gva.es/publicaciones/documentos/V.4565-2010.pdf.
Acknowledgements
This work was supported by a grant from the Conselleria de Sanitat (Valencian Community). This public organization subsidized and authorized this study exclusively to determine the situation in patients attending their health-care center. It played no part in the study design, data collection, analysis or interpretation, in writing the manuscript or in the decision to send it for publication. The grant was used to contract a person (Antonio Fernández) to collect and computerize the data.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Martínez-St John, D., Palazón-Bru, A., Gil-Guillén, V. et al. Differences in the management of hypertension, diabetes mellitus and dyslipidemia between obesity classes. J Hum Hypertens 30, 7–10 (2016). https://doi.org/10.1038/jhh.2015.29
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/jhh.2015.29
