
Abstract
Blood pressure (BP) categories defined by systolic BP (SBP) and diastolic BP (DBP) are commonly used. However, the BP category-specific risk of cardiovascular disease (CVD) has not been thoroughly investigated in different age groups. The aim of this study was to assess long-term CVD risk and its impact according to BP categories and age group. Pooling individual data from 10 cohorts, we studied 67 309 Japanese individuals (40–89 years old) who were free of CVD at baseline: we categorized them as belonging to three age groups: ‘middle-aged’ (40–64 years), ‘elderly’ (65–74 years) and ‘very elderly’ (75–89 years). BP was classified according to the 2009 Japanese Society of Hypertension Guidelines. Cox models were used to estimate adjusted hazard ratios for CVD deaths. We observed 1944 CVD deaths over a mean follow-up of 10.2 years. In all age groups, the overall relationship between BP category and CVD risk was positive, with a greater strength observed for younger age groups. We observed a trend of increased risk from SBP/DBP⩾130/85 mm Hg in the very elderly, and a significant increase from SBP/DBP⩾120/80 mm Hg in the other age groups. The population attributable fractions (PAFs) of CVD death in reference to the SBP/DBP<120/80 mm Hg category ranged from 23.4% in the very elderly to 60.3% in the middle-aged. We found an overall graded increase in CVD risk with higher BP category in the very elderly. The PAFs suggest that keeping BP levels low is an important strategy for primary CVD prevention, even in an elderly population.
Similar content being viewed by others
Introduction
Epidemiological studies have shown that the effect of both systolic blood pressure (SBP) and diastolic blood pressure (DBP) on the risk of cardiovascular disease (CVD) is continuous and consistent.1, 2 Because both SBP and DBP are independent predictors of CVD risk,3, 4, 5, 6, 7 most guidelines for adult blood pressure (BP) management have proposed similar BP categorization systems with regard to the following: (1) BP categories are defined by taking both SBP and DBP into account, and (2) the most favorable BP category is SBP<120 mm Hg and DBP<80 mm Hg, irrespective of age.8, 9, 10, 11
Although such BP categorization is widely used, there is only limited evidence assessing long-term CVD risk according to BP category, particularly for elderly populations. Given the worldwide trend of aging,12 assessing the long-term risk of elevated BP and its impact on the aged population is increasingly important from both clinical and public health standpoints. The Framingham Heart Study (FHS) reported graded increases in major CVD risk across higher BP categories among 1932 participants aged ⩾80 years.13 However, the follow-up period was relatively short (mean, 2.7 years).13 Therefore, long-term CVD risk was not fully assessed in that study. Other Western studies seeking to assess the BP category-specific risk of CVD events were based on subjects aged ⩽75 years.5, 14, 15, 16 Epidemiological studies on long-term CVD risk among an elderly population have also been limited,17, 18 and hence needed,19 in Asia.
The objectives of this study were (1) to estimate long-term CVD mortality risk according to BP categories defined by both SBP and DBP, (2) to examine whether the relationship between BP categories and CVD risk differs according to age group and (3) to compare the impact of increased BP on long-term CVD risk for different age groups by estimating population attributable fractions (PAFs). We focused particularly on an elderly population.
Methods
Design
This study is part of a pooling project in which individual participants’ data from 13 observational cohorts across Japan were combined. The project was designed to examine the relationship between disease mortality and various exposure factors, including laboratory and lifestyle/behavioral factors. The project is called Evidence for Cardiovascular Prevention from Observational Cohorts in Japan. The inclusion criteria for the cohorts were as follows: collection of health examination measures, follow-up of almost 10 years and more than 1000 participants. Both nationwide and regional cohort studies were included. Other details are reported elsewhere.20
Study population
In all, 10 of 13 cohorts provided data on cause of death (n=90 528). Of those, we used the following exclusion criteria for the present study: age <40 years or >89 years at baseline (n=10 528); history of CVD at baseline (n=5031); missing values for SBP, DBP or both (n=147); and missing adjusting covariates (n=7513). Thus, 67 309 individuals from 10 cohort studies were pooled (Tanno-Sobetsu, Ohsaki, Ohasama, Oyabe, YKK workers, the Radiation Effects Research Foundation cohort, Hsayama, JACC study, NIPPON DATA80 and NIPPON DATA90; see Supplementary Table S1 for the demographics of each cohort).
Death ascertainment
In accordance with the Family Registration Law in Japan, all death certificates are forwarded to the Ministry of Health, Labour and Welfare via the public health center in the area of residence. Registration of death is required by law and believed to be complete. The underlying cause of death is coded according to the International Classification of Disease (ICD) for National Vital Statistics, based on the criteria proposed by the World Health Organization.21
Cause of death was sought in great detail using the available sources in each cohort study. In most studies, death certificates were reviewed and/or National Vital Statistics were used after obtaining permission. Other sources used in some studies included autopsy, medical records, health examination and questionnaires. The cause of death was coded based on either ICD-9 or ICD-10. The classification codes used in the study were as follows: death from CVD (390–459 by ICD-9; I00–I99 by ICD-10), total stroke (410–414 or 430–438; I20–I25 or I60–I69), ischemic stroke (433 or 434 or 437.8; I63 or I69.3), intracerebral hemorrhage (431–432; I61 or I69.1), coronary heart disease (410–414; I20–I25) and heart failure (428; I50).
BP measurement
Detailed information on the BP measurement method for each cohort is provided in Supplementary Table S2. BP measurements were obtained using a mercury sphygmomanometer when each participant was in a seated position in all but two cohort studies. In one cohort (Ohasama), an automated device was used.22 In the other study (JACC), the BP values were based on self-recorded values after BP had been measured at a health check-up.23 In most cohorts, BP was measured once with a participant in a seated position after rest.
BP categories
Participants were categorized according to the modified classification of the 2009 Japanese Society of Hypertension Guidelines (JSH2009).10 The cutoff values for the BP classification were the same as those in the 2007 Guidelines from the European Society of Hypertension and the European Society of Cardiology (ESH-ESC 2007).8 Optimal BP was defined as SBP<120 mm Hg and DBP<80 mm Hg; the corresponding SBP and DBP values were 120–129 and 80–84 mm Hg for normal/non-optimal BP, 130–139 or 85–89 mm Hg (whichever was greater) for high-normal BP, 140–159 or 90–99 mm Hg for grade I hypertension, 160–179 or 100–109 mm Hg for grade II hypertension, and ⩾180 or ⩾110 mm Hg for grade III hypertension, respectively.
Statistical analysis
We estimated multivariable adjusted hazard ratios (HRs) of death from total CVD and its subtypes for each BP category by Cox proportional hazard models, in reference to the optimal BP category. We constructed two models to adjust for potential confounders. First, we adjusted for age (years), sex and cohort (model 1). Second, we further adjusted for serum total cholesterol (mmol l−1), body mass index (kg m−2), smoking status (current, past, never)24 and alcohol intake (current, past, never) (model 2).
To examine whether the relationship between BP category and risk of CVD death differed according to age, we divided participants into three groups based on their age at baseline: ‘middle-aged’ represented those 40–64 years old, ‘elderly’ represented those 65–74 years old and ‘very elderly’ represented those 75–89 years old. The HR and the corresponding PAF for CVD deaths were estimated for each BP category in each age group. To assess heterogeneity, we assumed a monotonic association between CVD risk and BP category and created pertinent variables. In assessing heterogeneity among cohorts, we created a Forest plot.
PAF was calculated as pd × (RR−1)/RR, where pd represents the proportion of exposed deaths in a specific BP category and RR is the corresponding multivariable-adjusted HR in reference to the optimal BP category.25 Additionally, we calculated gender-specific mortality risks and PAFs for CVD, total stroke, ischemic stroke, intracerebral hemorrhage, coronary heart disease and heart failure according to the BP category. In testing statistical evidence of interaction between sex and BP category on the effect of CVD risk, we first visually confirmed the overall positive relationship between BP category and CVD risk in both sexes. Then, we created an ordinal variable for BP category and its interaction term with sex, and inserted them in the models.
We performed the following sensitivity analyses: (1) excluding those who died from any cause within the first 3 years as an attempt to eliminate potential reverse causality from low BP;26, 27 (2) restricting the subjects to non-users of antihypertensive medication at baseline; and (3) adding diabetes mellitus (DM) status (yes or no) to the models for those participants for whom diabetes-defining variables were available (n=36 393). We defined DM as either a fasting glucose level of ⩾126 mg dl−1 (7.0 mmol l−1), a casual glucose level of ⩾200 mg dl−1 (11.1 mmol l−1), a Hb A1c level of ⩾6.5%, a history of DM, or taking medication for DM.
All statistical analyses were performed using SAS version 9.13 (SAS Institute, Cary, NC, USA). All of the P values for statistical tests were two-tailed, and P<0.05 were regarded as statistically significant. The study protocol was approved by the internal review board at each study center.
Results
The participants’ characteristics at baseline according to BP category are shown in Table 1. The proportion of the participants (n=67 309) in each BP category was 21.9 (optimal BP), 20.2 (normal/non-optimal BP), 21.3 (high-normal BP), 24.9 (grade I hypertension), 9.0 (Grade II hypertension) and 2.7% (grade III hypertension) at baseline. Compared with participants in higher BP categories, those in the optimal BP category tended to be younger and to have a lower body mass index and lower total cholesterol level at baseline. The number of participants categorized as middle-aged, elderly and very elderly was 49 935 (74.2%), 13 707 (20.4%) and 3667 (5.4%), respectively.
During a mean follow-up of 10.2 years, we observed 1944 CVD deaths: 917 from total stroke, 479 from ischemic stroke, 220 from intracerebral hemorrhage, 388 from coronary heart disease and 343 from heart failure in all age groups combined. In the Cox regression models, CVD risk increased almost continuously as the BP category advanced. In disease-specific analyses, the risk of total stroke and coronary heart disease increased similarly as the BP category advanced (see Supplementary Table S3). The PAF estimates indicated that the elimination of normal/non-optimal BP to grade III hypertension could have prevented almost half of the CVD deaths. The results were similar for both sexes, with no statistical evidence of interaction (P for interaction by sex 0.95) (see Supplementary Table S4 and Supplementary Table S5 for sex-specific results).
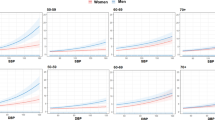
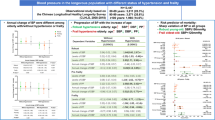
The crude death rates, adjusted HRs and PAFs according to BP category for each age group are shown in Table 2. The overall relationship between BP category and CVD risk was positive and graded for all age groups, with a greater strength of association observed in the younger group (P value for heterogeneity<0.001). For both the middle-aged and elderly groups, compared with individuals in the optimal BP category, the CVD risk increased significantly for those in the normal/non-optimal BP category and continued to increase overall for those in higher BP categories. For the very elderly group, in contrast, both optimal and normal/non-optimal BP categories appeared to have the lowest CVD risk. The PAFs for CVD death in reference to the optimal BP category tended to be greater for younger groups, accounting for 60, 49 and 23% of all CVD deaths in the middle-aged, elderly and very elderly groups, respectively. There is no statistical evidence that these trends differ according to sex in any of the age groups (P values for interaction by sex were 0.23, 0.11 and 0.50 for the middle-aged, elderly and very elderly, respectively). (For sex-specific results by age group, see Supplementary Table S6 and Supplementary Table S7).
The Forest plot by cohort indicated an apparently stronger effect of BP in the YKK workers cohort than in other cohorts (Supplementary Figure S1). However, the confidence interval was wide, and the direction of association was the same as for the other cohorts. Furthermore, exclusion of this cohort did not change the results substantially (data not shown). In the Forest plot, we did not observe a clear difference among methods of BP measurement.
In the first sensitivity analysis, which excluded deaths within the first 3 years, the observed association between the BP category and CVD death became stronger for the very elderly group than it was in the main analysis, such that the CVD risk significantly increased for participants in the high-normal BP category and higher categories (Table 3). The results for other age groups were similar to those in the main analysis. In the second sensitivity analysis, which was restricted to non-users of antihypertensive medication at baseline (29 097 participants, 823 CVD deaths), we observed similar results to the main analysis for all age groups (see Supplementary Table S8). In the third sensitivity analysis, which included DM status in the model, the relationship between BP category and CVD risk was attenuated in both the elderly and very elderly groups, whereas the relationship was slightly strengthened in the middle-aged group (see Supplementary Table S9).
Discussion
This pooled analysis of 10 well-qualified, prospective cohort studies in Japan enabled us to investigate the detailed relationship between BP categories and long-term CVD mortality risk over a broad age range. We found an overall positive relationship for all of the age groups that were studied. In the middle-aged and elderly groups, the risk was lowest for those in the optimal BP category. Importantly, even in the very elderly, the risk appeared to increase from the high-normal BP category to higher BP categories in a graded fashion. The relationship became stronger in this age group when the first 3 years of deaths were excluded. Another important finding of our study is that the impact of elevated BP, as measured by PAF, remained substantial in older groups, suggesting that maintaining optimal BP could have eliminated as many as one-quarter of CVD deaths in the very elderly group and half of those in the elderly group.
In many guidelines, BP categorization involves both SBP and DBP, and the same cutoff values are used irrespective of age.8, 9, 10, 11 However, only a few studies have examined BP category-specific CVD risk in an elderly population. To our knowledge, this is the first observational study that has demonstrated a long-term CVD risk and its impact according to BP category in a group of very elderly (aged ⩾75 years) Asian men and women. From North America/European regions, the FHS showed that major CVD risk increased in a graded fashion with advancing BP category among those aged ⩾80 years.13 Most other studies from these regions have examined populations aged ⩽75 years.5, 14, 15, 16 The FHS observed 336 CVD events among 1932 elderly over a mean of 2.7 years.13 Compared with the FHS, we observed more than five times as many CVD events among twice as many elderly participants over a mean of 10.2 years. Furthermore, we used six BP categories compared with the four used in the FHS (based on a modified version of the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure (JNC7) guidelines).9 Our categorization allows us to show finer BP category-specific CVD risks, such as those for normal/non-optimal BP or high-normal BP categories. Nevertheless, our results were broadly consistent with those in the FHS. There are at least two large-scale meta-analyses with pooled data from individual participants that have studied the association between BP and CVD risk: the Prospective Studies Collaboration (PSC)2 and the Asia Pacific Cohort Studies Collaboration (APCSC).28 Although our results are consistent with the results of these studies, our study differs significantly from both of these studies with respect to BP measurements. The PSC and the APCSC used either continuous DBP or SBP alone, whereas we used BP categories that accounted for both SBP and DBP. Several studies from Japan have reported both BP category-specific risk and/or PAF for CVD events.29, 30, 31, 32, 33 Because of the small sample sizes, however, none of these studies sought detailed estimates for the very elderly population (aged ⩾75 years), unlike the present study. A recent, large, prospective study from China showed both BP category-specific risk and PAF for CVD events.18 However, this study provided only limited information with regard to BP category-specific risk and impact on the very elderly population because the authors grouped those aged ⩾65 years together and used fewer BP categories (a modified JNC7 categorization similar to the FHS) than did our study.
When excluding the first 3 years of death in the very elderly, we observed a stronger overall relationship between BP category and CVD risk, with a significant increase in risk observed for the high-normal BP category and higher categories. This observation may suggest the presence of reverse causality, in which a poor health condition could have caused a lower BP.34, 35 Exclusion of the first few years of deaths from the analysis was proposed as one way to address reverse causality, particularly when analyzing an elderly population.26, 27, 35 Therefore, the lack of difference in CVD risk between the two lowest BP categories in the very elderly group may be attributable to reverse causality. Another possible explanation is that there is an attenuated strength of association between BP and CVD risk in this age group compared with younger age groups.3, 28
We observed a significant difference in the strength of the association between BP and CVD risk (that is, a difference in the relative risk of CVD) according to age group. Such heterogeneity by age in the effect of BP on CVD risk has been observed consistently in many large observational studies.18, 28, 32, 36 However, a recent meta-analysis of clinical trials by the Blood Pressure Lowering Treatment Trialists’ Collaboration (BPLTTC) concluded that there was no evidence of statistical heterogeneity in the effect of BP-lowering therapy on CVD risk between younger and older subjects.37 We speculate that this discrepancy could be due to differences between observational studies and clinical trials and/or due to a lack of statistical power in the BPLTTC study, as the authors of the study have noted.37
Regarding sex-specific differences, we observed that the absolute risk of CVD was generally higher in men than in women in all age groups, whereas the relative risk of CVD according to BP category (expressed as the HR) was similar between men and women (Supplementary Table S4–S7). These findings were consistent with those of previous large observational studies.18, 38
The PAF estimates calculated in our study imply that, in a Japanese population, BP has a greater impact on CVD risk than does smoking24, 39, 40 or elevated cholesterol.41 Combined with the observed lower CVD risks associated with the lower BP categories, the results endorse maintaining a low BP throughout one’s life as an important strategy for CVD prevention, both at an individual level and at the population level. It should be emphasized, however, that our results do not necessarily endorse pharmaceutical treatment for hypertension because the study was an observational study among a general population, and not an interventional study on a group of patients. In fact, recent studies indicate that the use of antihypertensive medication is unlikely to lower the risk of CVD to the same level as the risk for those who remain in low BP categories without such treatment.42 Furthermore, evidence on pharmaceutical treatment for hypertension in the very elderly is still limited, as stated in the recent consensus document by the American College of Cardiology Foundation and the American Heart Association.43
Several limitations need to be considered when interpreting our results. First, we did not take into account the use or non-use of antihypertensive medication in the main analyses because of a substantial amount of missing information. However, the sensitivity analysis that was restricted to non-users of such medication at baseline showed similar results to the main analyses for all three age groups. Thus, it is unlikely that this limitation would materially change our inferences. Second, the study was based on a BP measurement on a single occasion, and it did not account for regression dilution bias.2 Therefore, the results of the study are likely to underestimate the true association. Third, our estimates in the main analyses were not adjusted for DM. However, we found qualitatively similar results in the sensitivity analysis that adjusted for DM. Therefore, the influence of this limitation on our conclusion would likely be small. One strength of the study is that we pooled data from cohorts with a prospective design with a long follow-up period (over 10 years). Another strength is that the results are likely to be generalizable to a wide age range of adult men and women given that our samples were obtained from across the nation.
In summary, we observed a graded positive trend in CVD mortality risk starting from the high-normal BP category (SBP/DBP>130/85 mm Hg) continuing up to the higher BP categories among the very elderly group and a significant increase in risk starting from the normal/non-optimal BP category (SBP/DBP>120/80 mm Hg) up to the higher categories among the middle-aged and elderly groups. The strength of association between the BP category and CVD risk was attenuated but remained positive and graded in the very elderly. PAFs revealed that keeping BP levels low could prevent one-quarter of CVD deaths in the very elderly and one-half of those in the elderly. These findings suggest that maintaining low BP is an important strategy for primary CVD prevention in an elderly population, even among those aged 75–89 years.
References
Stamler J, Stamler R, Neaton JD . Blood pressure, systolic and diastolic, and cardiovascular risks. US population data. Arch Intern Med 1993; 153: 598–615.
MacMahon S, Peto R, Cutler J, Collins R, Sorlie P, Neaton J, Abbott R, Godwin J, Dyer A, Stamler J . Blood pressure, stroke, and coronary heart disease. Part 1, Prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. Lancet 1990; 335: 765–774.
Lewington S, Clarke R, Qizilbash N, Peto R, Collins R . Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet 2002; 360: 1903–1913.
Miura K, Dyer AR, Greenland P, Daviglus ML, Hill M, Liu K, Garside DB, Stamler J . Pulse pressure compared with other blood pressure indexes in the prediction of 25-year cardiovascular and all-cause mortality rates: The Chicago Heart Association Detection Project in Industry Study. Hypertension 2001; 38: 232–237.
Domanski M, Mitchell G, Pfeffer M, Neaton JD, Norman J, Svendsen K, Grimm R, Cohen J, Stamler J . Pulse pressure and cardiovascular disease-related mortality: follow-up study of the Multiple Risk Factor Intervention Trial (MRFIT). JAMA 2002; 287: 2677–2683.
Okayama A, Kadowaki T, Okamura T, Hayakawa T, Ueshima H . Age-specific effects of systolic and diastolic blood pressures on mortality due to cardiovascular diseases among Japanese men (NIPPON DATA80). J Hypertens 2006; 24: 459–462.
Ueshima H, Iida M, Shimamoto T, Konishi M, Tsujioka K, Tanigaki M, Nakanishi N, Ozawa H, Kojima S, Komachi Y . Multivariate analysis of risk factors for stroke. Eight-year follow-up study of farming villages in Akita, Japan. Prev Med 1980; 9: 722–740.
Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, Grassi G, Heagerty AM, Kjeldsen SE, Laurent S, Narkiewicz K, Ruilope L, Rynkiewicz A, Schmieder RE, Struijker Boudier HA, Zanchetti A, Vahanian A, Camm J, De Caterina R, Dean V, Dickstein K, Filippatos G, Funck-Brentano C, Hellemans I, Kristensen SD, McGregor K, Sechtem U, Silber S, Tendera M, Widimsky P, Zamorano JL, Erdine S, Kiowski W, Agabiti-Rosei E, Ambrosioni E, Lindholm LH, Manolis A, Nilsson PM, Redon J, Struijker-Boudier HA, Viigimaa M, Adamopoulos S, Bertomeu V, Clement D, Farsang C, Gaita D, Lip G, Mallion JM, Manolis AJ, O’Brien E, Ponikowski P, Ruschitzka F, Tamargo J, van Zwieten P, Waeber B, Williams B. The task force for the management of arterial hypertension of the European Society of H, The task force for the management of arterial hypertension of the European Society of C. 2007 Guidelines for the management of arterial hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J 2007; 28: 1462–1536.
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jones DW, Materson BJ, Oparil S, Wright JT, Roccella EJ . The Seventh Report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC 7 report. JAMA 2003; 289: 2560–2572.
Ogihara T, Kikuchi K, Matsuoka H, Fujita T, Higaki J, Horiuchi M, Imai Y, Imaizumi T, Ito S, Iwao H, Kario K, Kawano Y, Kim-Mitsuyama S, Kimura G, Matsubara H, Matsuura H, Naruse M, Saito I, Shimada K, Shimamoto K, Suzuki H, Takishita S, Tanahashi N, Tsuchihashi T, Uchiyama M, Ueda S, Ueshima H, Umemura S, Ishimitsu T, Rakugi H . The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2009). Hypertens Res 2009; 32: 3–107.
Williams B, Poulter NR, Brown MJ, Davis M, McInnes GT, Potter JF, Sever PS, Mc GTS . Guidelines for management of hypertension: report of the fourth working party of the British Hypertension Society, 2004-BHS IV. J Hum Hypertens 2004; 18: 139–185.
United_Nations. World population ageing: 1950-2050. In Division_Department_of_Economic_and_Social_Affairs_United_Nations P (ed), The 2002 World Assembly on Ageing. United Nations Publications: New York 2001.
Lloyd-Jones DM, Evans JC, Levy D . Hypertension in adults across the age spectrum: current outcomes and control in the community. JAMA 2005; 294: 466–472.
Miura K, Daviglus ML, Dyer AR, Liu K, Garside DB, Stamler J, Greenland P . Relationship of blood pressure to 25-year mortality due to coronary heart disease, cardiovascular diseases, and all causes in young adult men: the Chicago Heart Association Detection Project in Industry. Arch Intern Med 2001; 161: 1501–1508.
Kshirsagar AV, Carpenter M, Bang H, Wyatt SB, Colindres RE . Blood pressure usually considered normal is associated with an elevated risk of cardiovascular disease. Am J Med 2006; 119: 133–141.
Liszka HA, Mainous AG, King DE, Everett CJ, Egan BM . Prehypertension and cardiovascular morbidity. Ann Fam Med 2005; 3: 294–299.
Arima H, Tanizaki Y, Kiyohara Y, Tsuchihashi T, Kato I, Kubo M, Tanaka K, Ohkubo K, Nakamura H, Abe I, Fujishima M, Iida M . Validity of the JNC VI recommendations for the management of hypertension in a general population of Japanese elderly: the Hisayama study. Arch Intern Med 2003; 163: 361–366.
He J, Gu D, Chen J, Wu X, Kelly TN, Huang JF, Chen JC, Chen CS, Bazzano LA, Reynolds K, Whelton PK, Klag MJ . Premature deaths attributable to blood pressure in China: a prospective cohort study. Lancet 2009; 374: 1765–1772.
Murakami Y . The need for further epidemiologic research on hypertension in Asian regions. Am J Hypertens 2009; 22: 1030.
Murakami Y, Hozawa A, Okamura T, Ueshima H . Relation of blood pressure and all-cause mortality in 180,000 Japanese participants: pooled analysis of 13 cohort studies. Hypertension 2008; 51: 1483–1491.
Anonymous. Mannual to fill in a death certificate (in Japanese), In The Ministry of Health, Labour, and Welfare (ed), The Ministry of Health, Labour, and Welfare 2010. http://www.mhlw.go.jp/toukei/manual/dl/manual.pdf.
Ohkubo T, Kikuya M, Metoki H, Asayama K, Obara T, Hashimoto J, Totsune K, Hoshi H, Satoh H, Imai Y . Prognosis of ‘masked’ hypertension and ‘white-coat’ hypertension detected by 24-h ambulatory blood pressure monitoring 10-year follow-up from the Ohasama study. J Am Coll Cardiol 2005; 46: 508–515.
Yamada S, Koizumi A, Iso H, Wada Y, Watanabe Y, Date C, Yamamoto A, Kikuchi S, Inaba Y, Toyoshima H, Kondo T, Tamakoshi A . Risk factors for fatal subarachnoid hemorrhage: the Japan Collaborative Cohort Study. Stroke 2003; 34: 2781–2787.
Murakami Y, Miura K, Okamura T, Ueshima H . Population attributable numbers and fractions of deaths due to smoking: a pooled analysis of 180,000 Japanese. Prev Med 2011; 52: 60–65.
Rockhill B, Newman B, Weinberg C . Use and misuse of population attributable fractions. Am J Public Health 1998; 88: 15–19.
Kikuya M, Ohkubo T, Asayama K, Metoki H, Obara T, Saito S, Hashimoto J, Totsune K, Hoshi H, Satoh H, Imai Y . Ambulatory blood pressure and 10-year risk of cardiovascular and noncardiovascular mortality: the Ohasama study. Hypertension 2005; 45: 240–245.
Glynn RJ, Field TS, Rosner B, Hebert PR, Taylor JO, Hennekens CH . Evidence for a positive linear relation between blood pressure and mortality in elderly people. Lancet 1995; 345: 825–829.
Lawes CM, Rodgers A, Bennett DA, Parag V, Suh I, Ueshima H, MacMahon S . Blood pressure and cardiovascular disease in the Asia Pacific region. J Hypertens 2003; 21: 707–716.
Sairenchi T, Iso H, Irie F, Fukasawa N, Yamagishi K, Kanashiki M, Saito Y, Ota H, Nose T . Age-specific relationship between blood pressure and the risk of total and cardiovascular mortality in Japanese men and women. Hypertens Res 2005; 28: 901–909.
Ikeda A, Iso H, Yamagishi K, Inoue M, Tsugane S . Blood pressure and the risk of stroke, cardiovascular disease, and all-cause mortality among Japanese: the JPHC Study. Am J Hypertens 2009; 22: 273–280.
Kokubo Y, Kamide K, Okamura T, Watanabe M, Higashiyama A, Kawanishi K, Okayama A, Kawano Y . Impact of high-normal blood pressure on the risk of cardiovascular disease in a Japanese urban cohort: the Suita study. Hypertension 2008; 52: 652–659.
Hozawa A, Kuriyama S, Kakizaki M, Ohmori-Matsuda K, Ohkubo T, Tsuji I . Attributable risk fraction of prehypertension on cardiovascular disease mortality in the Japanese population: the Ohsaki Study. Am J Hypertens 2009; 22: 267–272.
Iida M, Ueda K, Okayama A, Kodama K, Sawai K, Shibata S, Tanaka S, Keijnkai T, Horibe H, Minowa M, Yanagawa H, Hashimoto T . Impact of elevated blood pressure on mortality from all causes, cardiovascular diseases, heart disease and stroke among Japanese: 14 year follow-up of randomly selected population from Japanese -- Nippon data 80. J Hum Hypertens 2003; 17: 851–857.
Staessen J, Bulpitt C, Clement D, De Leeuw P, Fagard R, Fletcher A, Forette F, Leonetti G, Nissinen A, O'Malley K et al. Relation between mortality and treated blood pressure in elderly patients with hypertension: report of the European Working Party on High Blood Pressure in the Elderly. BMJ 1989; 298: 1552–1556.
Greenberg JA . Removing confounders from the relationship between mortality risk and systolic blood pressure at low and moderately increased systolic blood pressure. J Hypertens 2003; 21: 49–56.
Cholesterol, diastolic blood pressure, and stroke: 13 000 strokes in 450 000 people in 45 prospective cohorts. Prospective studies collaboration. Lancet 1995; 346: 1647–1653.
Turnbull F, Neal B, Ninomiya T, Algert C, Arima H, Barzi F, Bulpitt C, Chalmers J, Fagard R, Gleason A, Heritier S, Li N, Perkovic V, Woodward M, MacMahon S . Effects of different regimens to lower blood pressure on major cardiovascular events in older and younger adults: meta-analysis of randomised trials. BMJ 2008; 336: 1121–1123.
Miura K, Nakagawa H, Ohashi Y, Harada A, Taguri M, Kushiro T, Takahashi A, Nishinaga M, Soejima H, Ueshima H . Four blood pressure indexes and the risk of stroke and myocardial infarction in Japanese men and women: a meta-analysis of 16 cohort studies. Circulation 2009; 119: 1892–1898.
Mannami T, Iso H, Baba S, Sasaki S, Okada K, Konishi M, Tsugane S . Cigarette smoking and risk of stroke and its subtypes among middle-aged Japanese men and women: the JPHC Study Cohort I. Stroke 2004; 35: 1248–1253.
Baba S, Iso H, Mannami T, Sasaki S, Okada K, Konishi M . Cigarette smoking and risk of coronary heart disease incidence among middle-aged Japanese men and women: the JPHC Study Cohort I. Eur J Cardiovasc Prev Rehabil 2006; 13: 207–213.
Woodward M, Martiniuk A, Lee CM, Lam TH, Vanderhoorn S, Ueshima H, Fang X, Kim HC, Rodgers A, Patel A, Jamrozik K, Huxley R . Elevated total cholesterol: its prevalence and population attributable fraction for mortality from coronary heart disease and ischaemic stroke in the Asia-Pacific region. Eur J Cardiovasc Prev Rehabil 2008; 15: 397–401.
Asayama K, Ohkubo T, Yoshida S, Suzuki K, Metoki H, Harada A, Murakami Y, Ohashi Y, Ueshima H, Imai Y . Stroke risk and antihypertensive drug treatment in the general population: the Japan arteriosclerosis longitudinal study. J Hypertens 2009; 27: 357–364.
Aronow WS, Fleg JL, Pepine CJ, Artinian NT, Bakris G, Brown AS, Ferdinand KC, Forciea MA, Frishman WH, Jaigobin C, Kostis JB, Mancia G, Oparil S, Ortiz E, Reisin E, Rich MW, Schocken DD, Weber MA, Wesley DJ, Harrington RA . ACCF/AHA 2011 expert consensus document on hypertension in the elderly: a report of the American College of Cardiology Foundation Task Force on Clinical Expert Consensus Documents. Circulation 2011; 123: 2434–2506.
Acknowledgements
We are grateful to all of the participants in each cohort study. This research was supported by a grant-in-aid from the Ministry of Health, Labour and Welfare, Health and Labor Sciences research grants, Japan (Research on Health Services: H17-Kenkou-007; Comprehensive Research on Cardiovascular Disease and Life-Related Disease: H18-Junkankitou[Seishuu]-Ippan-012; Comprehensive Research on Cardiovascular Disease and Life-Related Disease: H19-Junkankitou [Seishuu]-Ippan-012; Comprehensive Research on Cardiovascular and Life-Style Related Diseases: H20-Junkankitou [Seishuu]-Ippan-013; and Comprehensive Research on Cardiovascular and Life-Style Related Diseases: H23-Junkankitou [Seishuu]-Ippan-005).
Author information
Authors and Affiliations
Consortia
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on Hypertension Research website
Supplementary information
Appendix
Appendix
The EPOCH-JAPAN Research Group
Evidence for Cardiovascular Prevention from Observational Cohorts in Japan Research Group is composed of the following individuals: Chairperson: Hirotsugu Ueshima (Shiga University of Medical Science); Executive committee: Hirotsugu Ueshima (Shiga University of Medical Science), Yutaka Imai (Tohoku University Graduate School of Pharmaceutical Sciences), Fujiko Irie (Ibaraki Prefecture), Hiroyasu Iso (Osaka University Graduate School of Medicine), Yutaka Kiyohara (Kyushu University Graduate School of Medicine), Katsuyuki Miura, Yoshitaka Murakami (Shiga University of Medical Science), Hideaki Nakagawa (Kanazawa Medical University), Takeo Nakayama (Kyoto University School of Public Health), Tomonori Okamura (Keio University), Akira Okayama (Japan Anti-Tuberculosis Association), Toshimi Sairenchi (Dokkyo Medical University), Shigeyuki Saitoh (Sapporo Medical University), Kiyomi Sakata (Iwate Medical University), Akiko Tamakoshi (Aichi Medical University), Ichiro Tsuji (Tohoku University Graduate School of Medicine) and Michiko Yamada (Radiation Effects Research Foundation).
Rights and permissions
About this article
Cite this article
Fujiyoshi, A., Ohkubo, T., Miura, K. et al. Blood pressure categories and long-term risk of cardiovascular disease according to age group in Japanese men and women. Hypertens Res 35, 947–953 (2012). https://doi.org/10.1038/hr.2012.87
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2012.87
Keywords
This article is cited by
-
Blood pressure classification using the Japanese Society of Hypertension Guidelines for the Management of Hypertension and cardiovascular events among young to middle-aged working adults
Hypertension Research (2024)
-
High blood pressure and colorectal cancer mortality in a 29-year follow-up of the Japanese general population: NIPPON DATA80
Hypertension Research (2024)
-
Could high continuity of care (COC) have a negative impact on subjective health of hypertensive patients? A Japanese perspective
Cost Effectiveness and Resource Allocation (2023)
-
Suboptimal control status of young hypertensive population
Clinical Hypertension (2023)
-
Self-measured home blood pressure highlights cardiovascular risk in women: the HOMED-BP study
Hypertension Research (2023)
