
Abstract
Background:
Long-term daily use of aspirin has been associated with reduced cancer mortality. To explore this association, we compared tumour TNM characteristics among aspirin users with those among non-users.
Methods:
From the Swedish Cancer Register, we identified patients diagnosed with colorectal, lung, prostate and breast cancers between 2006 and 2009 and matched them to the Swedish Prescribed Drug Register to obtain information on low-dose aspirin use prior to diagnosis. Contingency table and logistic regression analyses were used to test for association and obtain odds ratios (ORs).
Results:
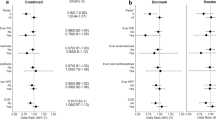
We identified 17 041 colorectal, 9766 lung, 29 770 prostate and 20 299 breast cancer patients. The proportion of low-dose aspirin users was ∼26% among colorectal, lung and prostate cancer patients and ∼14% among breast cancer patients. Adjusted for age, gender, education level and place of residence, low-dose aspirin use was associated with lower tumour extent (T) for colorectal and lung cancers (P<0.0001) but not for prostate and breast cancers. The adjusted OR of aspirin use for the T4 vs T1 categories was ∼0.7 (95% confidence interval (CI) 0.6–0.8). For all cancers, we found no evidence of association of aspirin use with nodal involvement (N). Except for a borderline result in prostate cancer (OR ∼0.9; 95% CI 0.8–1.0), aspirin use was associated with a lower rate of metastatic disease (ORs ∼0.6–0.8). Among the histological subgroups of lung cancer, significant differences in tumour extent were observed most clearly within the adenocarcinoma subgroup (OR ∼0.6, 95% CI 0.5–0.8), although numbers of other subtypes were more limited; and there was a significant reduction of ∼20–30% in the odds of metastasis among the aspirin users across the subgroups.
Conclusion:
Use of low-dose aspirin in the year prior to diagnosis was found to be associated with lower tumour extent and fewer metastatic disease for colorectal and lung cancers. For these cancers, the benefit of aspirin use appears to be during both early and late cancer progression.
Similar content being viewed by others


Main
Numerous studies, observational as well as randomised, have been performed to assess the association between aspirin intake and cancer risk and mortality. Evidence is growing that daily aspirin intake for 5 years or longer reduces the risk of death of cancer for several common cancers, notably colorectal and lung (Rothwell et al, 2011). This mortality benefit may partially be explained by reduced risk. Notably, however, Women’s Health Study (Cook et al, 2005), a randomised study of ∼40 000 participants, did not show benefit of aspirin vs placebo for cancer risk reduction. An earlier study from the Nurses’ Health Study cohort also reported null effects of aspirin on breast cancer risk (Egan et al, 1996). Reduced risk of colorectal cancer (Rothwell et al, 2010; Rothwell et al, 2012) was established in a meta-analysis of randomised studies, where both low-dose (75–300 mg daily) and high-dose aspirin (⩾500 mg daily) were attributed positive effects, primarily for long-term intake. Thus, so far convincing findings of an association between aspirin and reduced cancer incidence and mortality have mainly come from randomised trials, originally designed to examine the effect of aspirin on vascular disease (Thun et al, 2012). Evidence from observational studies has been pointing to the same direction, but the results across studies have been heterogeneous, notably for non-colorectal cancers, such as breast, prostate and lung (Bosetti et al, 2012; Seshasai et al, 2012).
Reduced mortality among aspirin users may also be explained by improved prognosis among those that develop cancer. For colon cancer patients, several studies have found an association between improved survival and postdiagnosis use of aspirin (Chan et al, 2009; Bastiaannet et al, 2012). Similarly, for breast cancer, Holmes et al (2010) found an association with a decreased risk of distant recurrence and breast cancer death. We aimed to further explore this question using a population-based approach by comparing the tumour characteristics of incident cancers among low-dose aspirin users and non-users in Sweden during 2006–2009. Better tumour characteristics in terms of extent/size (T), nodal involvement (N) or distant metastasis (M) are directly related to better prognosis and may suggest some early protective effects of aspirin use. As it uses no follow-up information after cancer diagnosis, the analysis of tumour characteristics is simpler and more transparent than the analysis of survival after diagnosis. Thus, in this study, we hypothesised that the use of low-dose aspirin is associated with better tumour characteristics in four common cancers, including colorectal, lung, prostate and breast cancers.
Methods
Cancer incidence and TNM values
Cancer registration in Sweden is mandated by law since 1958, estimated to have ∼96% coverage of all malignancies (Barlow et al, 2009). Stage information, in terms of tumour extent/size (T), nodal involvement (N) and metastatic status (M), is available since 2004. Our study was approved by the Ethical Committee of the Karolinska Institutet. Among all available cancer reports between 1 July 2006 and 31 December 2009 in the Swedish National Cancer Register, we identified 17 041 colorectal cancers (10 917 colon and 6124 rectum), 9766 lung cancers (944 small cell, 4080 non-small-cell adenocarcinoma, 1846 non-small-cell squamous, 2144 non-small-cell unspecified and 752 other), 29 770 prostate cancers and 20 299 breast cancers. All of these reports referred to primary cancers, and we excluded individuals with previous cancers. For each cancer case, we collected information on age, gender, the date of diagnosis and the individual TNM variables. Tables 1 and 2 show the number of cancer reports with available information on tumour characteristics, with respect to cancer type and TNM characteristics.
Aspirin prescription
Information on low-dose aspirin use was obtained from the Swedish Prescribed Drug Register (Wettermark et al, 2007), which had national coverage from mid-2005. This register covers all drugs sold and dispensed by prescription at Swedish pharmacies to patients with personal identification numbers. Drugs given to patients in hospitals are not included, and the coverage for drugs given in nursing homes is not complete. However, these places account for only a small portion of drug use. For example, for drugs acting on blood and blood-forming organs (ATC codes starting with ‘B’), 95% of all defined daily doses (DDDs) sold in Sweden were covered in the prescription register during its first 6 months, whereas 4% were sold to hospitals/nursing homes and 1% sold over the counter without needing prescription.
We found a total of 17 219 552 records of the low-dose aspirin prescription (ATC code B01AC06) between 1 July 2005 and 31 December 2009. During this period, 79% of B01AC06 tablets sold in Sweden contained 75 mg aspirin and the rest contained 160 mg. When we analysed the prescription patterns, 96% of all users in this time period were, in fact, prescribed one tablet per day, so there was little variation in the amount used by the patients. So, for our main analyses, we simply dichotomised the study subjects to users and non-users of aspirin. Reasons of prescription were not available in the register; however, in Sweden, low-dose aspirin was at the time prescribed for secondary prevention of myocardial infarction and stroke, not for cancer-related symptoms, so we do not expect any confounding by indication.
We also performed sensitivity analyses to assess the effects of (i) 1-year limit on aspirin use prior to diagnosis and (ii) binary classification of users vs non-users of aspirin. For the effects of aspirin use prior to diagnosis, in Supplementary Table 1, we present similar statistical analysis for which aspirin prescriptions preceding diagnosis with 2 years were available. For binary classification of users vs non-users of aspirin, we also categorised all cases as non-users and less-frequent and frequent users considering the amount prescribed in units of DDD, accumulated over the 1-year period prior to the diagnosis. According to WHO, DDD is the ‘assumed average maintenance dose per day for a drug used for its main indication in adults’. For low-dose aspirin, one DDD means one tablet, whereas the amount of aspirin per tablet can vary (in most cases 75 mg in Sweden; see above). In the resulting statistical analysis (Supplementary Table 2), individuals were categorised as less-frequent and frequent users according to whether the accumulated 1-year mean dose reached one per day, assuming the last prescribed dose before the 1-year interval distributed uniformly until the next prescription date and including the last prescribed dose before diagnosis in the total accumulated dose.
Age, gender, education and place of residence
Potential confounders in the analyses included age (obtained from the Cancer Register and categorised into <45 and >85 years and 5-year intervals in between), gender (from the Cancer Register), education status (from the Education Register; categorised into 0–9 years of education, middle school, university or higher) and place of residence (from the Cancer Register; categorised into rural and non-rural). Both aspirin prescription and cancer risk are age dependent, so age was expected to be a confounder. Educational level and place of residence are correlated with unmeasured confounders such as smoking and other lifestyle factors for which we did not have information in the national registers.
Statistical analysis
Adjusted analysis of the association between aspirin use and tumour characteristics was performed using polytomous logistic regression, with tumour characteristic as outcome and aspirin use, age, gender, education status and place of residence as predictors. All estimated odds ratios (ORs) refer to aspirin users vs non-users as reference group. For outcomes with multiple categories (such as T or N), the odds refers to the probability of higher code divided by the probability of the lowest code (e.g., T4 vs T1). Individual ORs are presented with 95% confidence intervals (CIs).
Results
Use of low-dose aspirin was ∼26% among colorectal, lung and prostate cancer patients but ∼14% among breast cancer patients (Table 1). We note that the association between aspirin use and cancer is typically confounded by age, so comparisons of crude rates are misleading. Overall, after adjustment for age, gender (where applicable), education status and place of residence, we saw significant associations between aspirin use and tumour extent (P<0.0001) in colorectal and lung cancers but not in prostate and breast cancers (P>0.05). In both colorectal and lung cancers, the use of low-dose aspirin is associated with ∼30% reduction in the odds of getting a T4 tumour (OR ∼0.7, 95% CI 0.6–0.8, for T4 vs T1). Association with nodal involvement (N) for all cancers was nonsignificant. Adjusted association of aspirin use with fewer metastases (M) was significant for colorectal and lung cancers (OR ∼0.8, 95% CI 0.7–0.9) and for breast cancer (OR ∼0.6, 95% CI 0.5–0.9) but not for prostate cancer (OR ∼0.9, 95% CI 0.8–1.0).
Dividing colorectal cancer into colon and rectum cancers (Table 2), the previously reported associations for tumour extent and distant metastases were equally present in both subgroups (P<0.0001 for T in both cancers, and P<0.0001 and 0.009 for M, respectively), but with diminished significance for rectum metastasis (M) due to lower sample size. Thus, we observed a statistically significant reduction of ∼30% in the odds of T4 vs T1 colon cancers, a corresponding ∼50% reduction for rectum cancers and a statistically significant reduction of ∼20% and ∼30%, respectively, in the odds of metastases for aspirin users.
We divided the lung cancers into three major subgroups: small cell, non-small-cell adenocarcinoma and non-small-cell squamous-cell carcinoma (Table 2). Consistently significant association for tumour extent (T) was obtained only for the non-small-cell adenocarcinoma (OR ∼0.6, 95% CI 0.5–0.8). For the squamous-cell carcinoma, only the highest T3 category is significant (OR ∼0.6, 95% CI 0.4–0.9). The lack of significant results was partly due to the fact that the numbers of small cell and non-small-cell squamous cancer reports were smaller than the number of non-small-cell adenocarcinomas. For the adenocarcinoma, we observed the only significant association with reduced nodal involvement among aspirin users, with OR ∼0.7 (95% CI 0.5–0.9). Finally, there was a near-consistent significant reduction of ∼20–30% in the odds of metastasis among the aspirin users across the three lung cancer subgroups.
Discussion
We found coherent and significant association between low-dose aspirin use in the year prior to cancer diagnosis and tumour extent (T) in colorectal and lung cancer patients but not in prostate or breast cancer patients. Except for a borderline significance in prostate cancer, there was a consistent association between aspirin use and distant metastasis (M) across colorectal, lung and breast cancers, including the subgroups of colorectal and lung cancers. Generally, we did not observe any association between low-dose aspirin use and nodal involvement (N). When analysed separately, the patterns for colon and rectum cancers were similar. Among lung cancer histological groups, the pattern was clearest within the non-small-cell adenocarcinoma subgroup, but the numbers of the other subgroups were more limited; moreover, we saw a consistent reduction of the rate of metastasis among aspirin users across the subgroups.
Assuming that the adjustment by age, gender, education status and place of residence was adequate to deal with potential confounders, the results imply that low-dose aspirin users among colorectal or lung cancer patients have a survival advantage vs non-users. This protective effect would then partially account for the cancer mortality benefit of aspirin use. Observing the differences of tumour extent at diagnoses suggests protective effect early in cancer progression in colorectal and lung cancers. Early protective effects of aspirin on cancer progression suggest that aspirin may be useful in chemoprevention. The near-consistent findings of lower metastatic disease may also suggest that aspirin is also beneficial at later stages of cancer progression. Finally, what is to make of the intriguing lack of association with nodal status for all cancers? One possible explanation could be that one benefit of aspirin is due to its antiplatelet property; involvement of platelet in cancer is well known (e.g., see Jurasz et al, 2004), but platelet is not found in the lymphatic system, so here aspirin lacks a key substrate to exert its effects.
The beneficial effects of aspirin were previously shown to come after long-term use (e.g., see Rothwell et al, 2011). It is a weakness of this study that we did not have long enough follow-up to assess long-term exposure, but we may consider the exposure in the year prior to diagnosis as a proxy variable, as a portion of the users is likely to be long-term users. It is expected that this weakness attenuates the true drug effects, leading to a conservative analysis, with significant results suggesting a larger effect than the observed estimate. We performed a sensitivity analysis by using a 2-year limit prior to diagnosis as the exposure period (Supplementary Table 1); the results were broadly similar, although we lost some power due to lower number of events.
Another weakness, given our dependence on the Prescribed Drug Register, is the lack of information on compliance. Thus, although we know that the drug was dispensed to the patients, we cannot tell for sure whether it was taken daily, less regularly or not taken at all. Again, it is expected that the impact might attenuate the true drug effects.
As a third weakness of the study, the information on TNM status was incomplete for a portion of the cancers, mostly due to Tx, Nx or Mx codes, meaning they were ‘not assessed’. For colorectal cancer, the rate of incompletion was highly similar between users and non-users of aspirin. For the other cancers and across the TNM variables, the incompletion among users of aspirin was 1–7% higher than among non-users. However, we suspect that when a cancer TNM status was not assessed, then it was likely to be of the lower category; for example, Mx was more likely to be M0 rather than M1. This means that had the data been complete, we would probably see a larger proportion of lower categories. Consequently, we might then have seen a larger protective effect of aspirin, as the incompletion was higher among users of aspirin.
The strength of the study is that it is a large population-based study of the whole Swedish population. Hence, it captures the real effects of aspirin when used widely in an open population, with no issue of preselection or inclusion/exclusion criteria imposed as in clinical trial samples. Alas, as a common weakness of observational studies, we cannot rule out confounders beyond those we have adjusted for. We observed a clear value of adjusting for age, gender and education with respect to the following two effects: (i) for both prostate and breast cancers, before adjustment, tumour extent was unexpectedly worse for aspirin users but not after adjustment; (ii) for lung tumour extent, the association was not significant before adjustment but significant in the expected direction after adjustment.
Another strength of the study was that we analysed four common cancers and three characteristics together so that the results can immediately be compared with each other. As an example, if one argues that the result for tumour extent was due to some potential confounding factor, then one must also explain why such confounding did not affect nodal involvement. Similarly, if the results for colorectal and lung cancers were due to some potential confounding, then such confounding should not affect prostate and breast cancers in the same way. One potential confounding was a differential surveillance between aspirin users and non-users. In Sweden, we have opportunistic screening of prostate cancer with PSA testing and a nationwide mammographic screening program for breast cancer but no comparable screening for colorectal and lung cancers. It was conceivable that, because of screening, both aspirin users and non-users get equal surveillance for prostate and breast cancers, whereas for colorectal and lung cancers, aspirin users received more medical attention, thus higher surveillance. This is a difficult issue, but there are several arguments against surveillance bias being the explanation of our results. First, the annual uptake of PSA screening among Swedish men aged 55–69 years peaked at 12% in 2004 and declined to 7% in 2007 (Jonsson et al, 2011), so screening cannot fully equalise the surveillance level between users and non-users of aspirin. Second, from the analyses of randomised studies, for which there was no surveillance bias, there was a significant association between aspirin use and distant metastasis for colorectal cancer (Rothwell et al, 2012), so we have observed a consistent result. Third, as commented above, we can ask that if the result of lower tumour extent in colorectal and lung cancers was due to higher surveillance in the aspirin group, then why did we not get a similarly lower rate of nodal involvement.
In summary, we found evidence that the use of low-dose aspirin in the year prior to diagnosis was associated with better tumour extent for colorectal and lung cancers, but not for prostate and breast cancers, and was associated with lower metastatic disease for colorectal, lung and breast cancers. This result partially explains the mortality benefit of aspirin use observed particularly in colorectal and lung cancers; it may also suggest early and late protective effects and, consequently, a potential use of aspirin for chemoprevention and cancer therapy.
Change history
01 October 2013
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Barlow L, Westergren K, Holmberg L, Talback M (2009) The completeness of the Swedish Cancer Register: a sample survey for year 1998. Acta Oncol 48: 27–33.
Bastiaannet E, Sampieri K, Dekkers OM, de Craen AJ, van Herk-Sukel MP, Lemmens V, van den Broek CB, Coebergh JW, Herings RM, van de Velde CJ, Fodde R, Liefers GJ (2012) Use of aspirin postdiagnosis improves survival for colon cancer patients. Br J Cancer 106: 1564–1570.
Bosetti C, Rosato V, Gallus S, Cuzick J, La Vecchia C (2012) Aspirin and cancer risk: a quantitative review to 2011. Ann Oncol 23: 1403–1415.
Chan AT, Ogino S, Fuchs CS (2009) Aspirin use and survival after diagnosis of colorectal cancer. JAMA 302: 649–659.
Cook NR, Lee IM, Gaziano JM, Gordon D, Ridker PM, Manson JE, Hennekens CH, Buring JE (2005) Low-dose aspirin in the prevention of cancer: the Women’s Health Study: a randomized controlled trial. JAMA 294: 47–55.
Egan KM, Stampfer MJ, Giovannucci E, Rosner BA, Colditz GA (1996) Prospective study of regular aspirin use and the risk of breast cancer. J Natl Cancer Inst 88: 988–993.
Holmes MD, Chen WY, Li L, Hertzmark E, Spiegelman D, Hankinson SE (2010) Aspirin intake and survival after breast cancer. J Clin Oncol 28: 1467–1472.
Jonsson H, Holmström B, Duffy SW, Stattin P (2011) Uptake of prostate-specific antigen testing for early prostate cancer detection in Sweden. Int J Cancer 129: 1881–1888.
Jurasz P, Alonso-Escolano D, Radomski MW (2004) Platelet–cancer interactions: mechanisms and pharmacology of tumour cell-induced platelet aggregation. Br J Pharmacol 143: 819–826.
Rothwell PM, Fowkes FG, Belch JF, Ogawa H, Warlow CP, Meade TW (2011) Effect of daily aspirin on long-term risk of death due to cancer: analysis of individual patient data from randomized trials. Lancet 377: 31–41.
Rothwell PM, Wilson M, Elwin CE, Norrving B, Algra A, Warlow CP, Meade TW (2010) Long-term effect of aspirin on colorectal cancer incidence and mortality: 20-year follow up of five randomized trials. Lancet 376: 1741–1750.
Rothwell PM, Wilson M, Price JF, Belch JF, Meade TW, Mehta Z (2012) Effect of daily aspirin on risk of cancer metastasis: a study of incident cancers during randomized trials. Lancet 379: 1591–1601.
Seshasai SRK, Wijesuriya S, Sivakumaran R, Nethercott S, Erqou S, Sattar N, Ray KK (2012) Effect of aspirin on vascular and nonvascular outcomes. Arch Intern Med 172: 209–216.
Thun MJ, Jacobs EJ, Patrono C (2012) The role of aspirin in cancer prevention. Nat Rev Clin Oncol 9: 259–267.
Wettermark B, Hammar N, Fored M, Leimanis A, Otterblad Olausson P, Bergman U, Persson I, Sundström A, Westerholm B, Rosén M (2007) The new Swedish Prescribed Drug Register – opportunities for pharmacoepidemiological research and experience from the first six months. Pharmacoepidemiol Drug Saf 16: 726–735.
Acknowledgements
We would like to acknowledge the Swedish Initiative for research on Microdata in the Social and Medical Sciences (SIMSAM), grant number 80748301. The use of the medical registers for this study was approved by Karolinska Institutet’s Ethical Review Committee, according to Dnr. 2012/658-31/2.
Author information
Authors and Affiliations
Corresponding author
Additional information
This work is published under the standard license to publish agreement. After 12 months the work will become freely available and the license terms will switch to a Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License.
Supplementary Information accompanies this paper on the British Journal of Cancer website
Supplementary information
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Jonsson, F., Yin, L., Lundholm, C. et al. Low-dose aspirin use and cancer characteristics: a population-based cohort study. Br J Cancer 109, 1921–1925 (2013). https://doi.org/10.1038/bjc.2013.411
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bjc.2013.411
Keywords
This article is cited by
-
Low-dose aspirin use and risk of ovarian cancer: a combined analysis from two nationwide studies in Denmark and Sweden
British Journal of Cancer (2024)
-
Target trial emulation of aspirin after diagnosis of colorectal polyps
European Journal of Epidemiology (2023)
-
Effect of aspirin on incidence, recurrence, and mortality in prostate cancer patients: integrating evidence from randomized controlled trials and real-world studies
European Journal of Clinical Pharmacology (2023)
-
Different associations of tumor PIK3CA mutations and clinical outcomes according to aspirin use among women with metastatic hormone receptor positive breast cancer
BMC Cancer (2020)
-
NSAIDs Use and Reduced Metastasis in Cancer Patients: results from a meta-analysis
Scientific Reports (2017)
