
Abstract
Background:
Several environmental factors have been associated with increased risks for cervical cancer. We examined whether reproductive history, contraceptive use, or sexual behaviour increase the risk for cervical intraepithelial neoplasia grade 3 or worse (CIN3+) among women with persistent human papillomavirus (HPV) infection.
Methods:
A population-based cohort of women participated in a personal interview and underwent a gynaecological examination at which cervical specimens were obtained for HPV DNA testing. Follow-up information (∼13 years) on cervical lesions was obtained from the Danish Pathology Data Bank. Women who had a high-risk HPV infection comprised the overall study population (n=1353). A subgroup of women with persistent high-risk HPV infection (n=312) was identified. Hazard ratios (HRs) for a diagnosis of CIN3+ and the corresponding 95% confidence intervals (CIs) were calculated.
Results:
Women with persistent HPV infection who had given birth had a significantly increased risk for CIN3+ (HR=1.78; 95% CI: 1.07–2.94). No association was found with pregnancy, use of intrauterine devices, or sexual behaviour. Based on small numbers, women with persistent HPV infection had a decreased risk for CIN3+ with any use of oral contraceptives (HR=0.54; 95% CI: 0.29–1.00).
Conclusion:
Childbirth increases the risk for subsequent CIN3+ among women with persistent HPV infection.
Similar content being viewed by others


Main
The common sexually transmitted high-risk human papillomavirus (HPV) is found to be a necessary factor for cervical cancer (Bosch et al, 2002). Most newly acquired HPV infections are transient, but a small fraction of infections persist, and it is these persistent infections that are involved in the development of cervical cancer and its immediate precursor lesions (Kjaer et al, 2010; Schiffman et al, 2011). Cervical cancer and the less severe but commoner precursor lesions results in high costs for treatment and surveillance, and cause anxiety (Kjaer, 2007). Identification of HPV cofactors, which in addition to HPV infection increase the risk for precursor lesions of cervical cancer, will lead to better understanding of the natural history of HPV and cervical carcinogenesis (Castellsague et al, 2002).
A variety of environmental factors, such as reproductive history (Castle et al, 2002, 2005; Munoz et al, 2002; Appleby et al, 2006; Gargano et al, 2012; Liao et al, 2012), contraceptive use (Castle et al, 2002, 2005; Moreno et al, 2002; Appleby et al, 2007; Castellsague et al, 2011), and sexual behavioural factors (Appleby et al, 2009; Louie et al, 2009), have been suggested as HPV cofactors. Only a few of the known studies concerning these cofactors were prospective cohort studies (Castle et al, 2002, 2005; Gargano et al, 2012; Liao et al, 2012) and some did not differentiate between high- and low-risk HPV types (Moreno et al, 2002; Munoz et al, 2002; Louie et al, 2009; Castellsague et al, 2011) at baseline. In addition, in previous studies, a single measurement of baseline HPV infection (comprising newly acquired as well as persistent infections) was used, although women truly at risk for cervical progression have persistent high-risk HPV infection (Kjaer et al, 2010; Schiffman et al, 2011). Thus, it is still not clear whether any associations observed between these suggested HPV cofactors and high-grade cervical disease were due to an increase in the risk for persistence of the prevalent HPV infection or also to an increase in the risk for progression given persistent HPV infection. We have previously identified heavy smoking to increase the subsequent risk for high-grade cervical lesions given persistent HPV infection (Jensen et al, 2012). In this study, we examined the possible contribution of reproductive history, contraceptive use, and sexual behaviour to the subsequent risk for precursor lesions of cervical cancer in a prospective cohort study of high-risk HPV+ women and in a subgroup of women with persistent infection.
Materials and methods
The study population consisted of women who participated in a Danish population-based cohort study of the natural history of HPV (Kjaer et al, 2006). All participants provided written informed consent before entering the study. The study was approved by the National Scientific Ethical Committee and the National Data Protection Board. Residents of Denmark are assigned a unique personal identification number, which includes their sex and date of birth and is registered in the Central Population Register. Individual information on all residents is kept under this personal identification number in all public registries in Denmark, which ensures correct linkages between registries. The cohort consisted of a random sample of women aged 20–29 years living in the Copenhagen area (n=17 949) identified by the Central Population Register. All the women received a postal invitation to participate in the study. Women who had moved out of the uptake area when contacted were ineligible (n=1604). At the study site, the participants underwent a structured interview covering sociodemographic factors, lifestyle habits, reproductive factors, contraceptive use, sexual behaviour, and history of sexually transmitted infections. The participants also underwent a gynaecological examination, where a Pap smear was taken and cervical cells were obtained for later HPV DNA testing. At the first examination (May 1991–January 1993), 11 088 women participated. Approximately 2 years later (October 1993–January 1995), the same women were invited for a second examination. The women were invited in the same order as participating in the first examination, they underwent the same procedures, and a total of 8656 women participated.
Follow-up
The date of the second individual examination was chosen as the baseline. The women were followed from baseline to 6 March 2007. We obtained information about cervical lesions during follow-up by linking the participants’ personal identification numbers to the Danish Pathology Data Bank, a nationwide pathology register that contains the results of cervical cytology and histology in Denmark. Cervical diagnoses are mainly reported as atypia, mild dysplasia, moderate dysplasia, severe dysplasia, carcinoma in situ, or cancer. For our study, we translated the histological diagnoses into the cervical intraepithelial neoplasia (CIN) nomenclature, where CIN grade 3 (CIN3) or worse covers the diagnoses severe dysplasia, carcinoma in situ, and cancer. Regarding the cytological diagnoses, severe dysplasia, carcinoma in situ, and cancer were categorised as high-grade squamous intraepithelial lesions or worse.
HPV DNA testing
As described previously, Hybrid Capture 2 (Qiagen, Hilden, Germany) was used to test for HPV DNA in cervical samples (Kjaer et al, 2006). The high-risk probe that detects at least 13 high-risk types (HPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68) was used, and the cutoff of 1.0 pg ml−1 recommended by the United States Food and Drug Administration was adopted (Iftner and Villa, 2003). The samples that contained high-risk HPV DNA were later HPV genotyped by a polymerase chain reaction-based line probe assay (LiPAv2; Innogenetics Inc., Ghent, Belgium) (Klug et al, 2008), which allows detection of 24 HPV genotypes; we were interested in the 13 high-risk types. The cervical samples were tested for HPV infection years after the samples were obtained and the HPV results did not influence subsequent surveillance or treatment of the women.
Definition of the study population
The overall study population for our study consisted of women who provided biological material for HPV DNA testing at both examinations and who had a high-risk HPV infection (based on the Hybrid Capture 2) at baseline (n=1435). Women who had an inadequate baseline smear and women who did not undergo a cervical examination during follow-up were excluded (n=56), as were women with prevalent disease (moderate dysplasia or worse) at baseline or within 1 year before (n=26). The remaining 1353 women, who were high-risk HPV+ based on the single HPV measurement at baseline, constituted our overall study population. From this population, we identified a subgroup on the basis of the LiPAv2 HPV test results from both cervical examinations: woman who had the same HPV genotype at the baseline examination and at the examination 2 years before baseline were categorised as having persistent HPV infection (n=312).
We retrieved information about the covariates from the structured interview at the baseline examination. We used two measures of reproductive history, namely number of pregnancies (including induced abortions, miscarriages, and ectopic pregnancies) and number of births. We also evaluated the contributions of ever/never oral contraceptives (OCs) and intrauterine devices (IUDs). Among ever OC users, we studied the duration of OC use in three categories (⩽4, 5–9, and ⩾10 years), and among ever IUD users, we studied the duration in two categories (⩽4 and ⩾5 years). As a measure of sexual behaviour, age at first intercourse was divided into three categories (⩽15, 16–17, and ⩾18 years) and lifetime number of sexual partners was divided into four categories (⩽4, 5–9, 10–14, and ⩾15 partners). The outcome measure was immediate precursors of cervical cancer, defined as a histological diagnosis of CIN3 or worse or a cytological diagnosis of high-grade squamous intraepithelial lesions or worse. In the overall study population, we identified 241 women with high-grade cervical lesions of whom the majority (n=187) had a diagnosis of CIN3 or worse and 54 women had a diagnosis of high-grade squamous intraepithelial lesions or worse without histological confirmation. In the following, we use the term ‘CIN3+’ to refer to this combined outcome measure.
Statistical analyses
To determine whether reproductive history, contraceptive use, or sexual behaviour could predict CIN3+, an accelerated failure time model was used, which allowed the use of an interval censored response variable, as the exact date of development of a cervical lesion was unknown. A Weibull distribution was used for failure time, as the Weibull distribution fitted data significantly better than the more parsimonious exponential model (P<0.001) and as well as the more complex generalised gamma model (P=0.34). Hazard ratios (HRs) and their corresponding 95% confidence intervals (CIs) were estimated for CIN3+ in relation to reproductive history, contraceptive use, and sexual behaviour for both the overall study population and the subgroup of women who had persistent high-risk HPV infection at baseline. When we analysed the risk in relation to only histological diagnoses of CIN3 or worse, the results were virtually identical but with wider CIs as for the combined diagnoses. Thus, we used the combined outcome measure ‘CIN3+’.
We have found that smoking (Jensen et al, 2012) and length of schooling (data not shown), as a proxy for socioeconomic status (Bobák et al, 2000), are associated with a diagnosis of CIN3+. Furthermore, HPV type is known to be predictive for progression (Kjaer et al, 2010). Therefore, we present unadjusted estimates, estimates adjusted for smoking status (never, former, current) and length of schooling (long, medium, short), and estimates additionally adjusted for baseline HPV16 positivity (yes/no). The estimates for contraceptive methods and sexual behaviour were additionally adjusted for ever given birth (yes/no). We also initially adjusted for age, sexual behaviours, and OC use; however, it did not affect the overall results and these factors were not included as potential confounders in the final analysis. Finally, we also adjusted for length of time between the two examinations, but as this did not affect the estimate of the other variables, it was not included in the final statistical model.
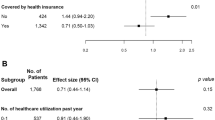
In a separate analysis, we studied whether some groups of women were more likely to undergo cervical cytology screening during follow-up and were therefore more likely to have cervical lesions detected and treated. A Poisson regression model was used to determine whether the number of cervical cytology examinations between baseline and the end of study varied with any of the potential cofactors. This was studied among women in the overall study population who had no abnormal cervical diagnoses during follow-up (n=954), taking the person time in the cohort into account.
Results
Table 1 shows the distribution of the two study groups in relation to reproductive history, contraceptive methods, and sexual behaviour, and the percentage of women who had a diagnosis of CIN3+ during follow-up. Overall, 17.8% of the high-risk HPV+ women had a diagnosis of CIN3+ and 30.8% of the women with persistent HPV infection had CIN3+ diagnosed during follow-up (Table 1). A small number of women had given birth twice or more and a high proportion of these women had a diagnosis of CIN3+: 27.5% of women who were high-risk HPV+ at one measure and as high as 83.3% of women with persistent HPV infection. In relation to OC use among women with a persistent HPV infection, a small number (n=28) of women reported never having used OC and 42.9% of these women had a diagnosis of CIN3+. The number of cervical cytological examinations during follow-up did not vary significantly with any of the potential cofactors (pregnancy, P=0.9; childbirth, P=0.6; OC use, P=0.7; IUD use, P=0.5; young age at first intercourse, P=0.3; or number of sexual partners, P=0.6) (data not shown).
The HRs for a subsequent diagnosis of CIN3+ in relation to reproductive history, contraceptive use, and sexual behaviour in the overall study population of women testing positive for high-risk HPV at baseline are shown in Table 2. We found no statistically significant association between pregnancy and CIN3+. In contrast, we found a statistically significantly increased risk for CIN3+ with ever giving birth (HR=1.39; 95% CI: 1.02–1.91) in the adjusted model and an almost two-fold increased risk in the unadjusted model for two or more deliveries compared with no deliveries (HR=1.90; 95% CI: 1.11–3.28). In the model where adjustment was made for smoking status, length of schooling, and HPV16 positivity, the HR did not reach statistical significance but was still markedly increased (HR=1.58; 95% CI: 0.91–2.74). In relation to contraceptive use, no association was seen with ever OC use, ever IUD use, or duration of use of these contraceptives. In addition, no statistically significant associations were observed with age at first intercourse or lifetime number of sexual partners.
In the subgroup of women with persistent high-risk HPV infection (Table 3), the women who had given birth were significantly more likely to have a subsequent diagnosis of CIN3+ (HR=1.78; 95% CI: 1.07–2.94) than those who had never given birth, and the estimate for two or more births was also markedly increased in the fully adjusted model (HR=2.59; 95% CI: 1.00–6.74). The likelihood of CIN3+ during follow-up was lower among women who ever had used OC (HR=0.54; 95% CI: 0.29–1.00) than among those who had never used them, and a statistically significantly decreased risk was observed for women who had used OC for 4 or less years (HR=0.47; 95% CI: 0.23–0.96). In contrast, neither pregnancy, IUD use, nor any of the sexual habit variables (age at first intercourse, number of sexual partners) showed any relation with the development of CIN3+ among women with a persistent high-risk HPV infection.
Discussion
In this study of high-risk HPV+ women, childbirth but not pregnancy was predictive of CIN3+ during up to 13 years of follow-up. The effect of parity was particularly evident when the study population was restricted to women with persistent high-risk HPV infection, which implies that the effect of childbirth on CIN3+ cannot solely be explained by an increased risk for HPV persistence. This has not been shown previously. Previous studies, which were based on a single HPV measurement, had conflicting results: in studies of pooled data, mainly from case–control studies, a strong association was found between cervical cancer and an increasing number of full-term pregnancies (Munoz et al, 2002; Appleby et al, 2006). Other studies also observed an increased risk with pregnancy or parity (Hildesheim et al, 2001; Castellsague et al, 2006; Wang et al, 2009; Almonte et al, 2011; Gargano et al, 2012; Liao et al, 2012), although some did not (Deacon et al, 2000; Ferrera et al, 2000; Castle et al, 2002, 2005). Castle et al (2005), who did not observe an association between parity and CIN3 or worse, suggested that their null finding could be explained by low parity and choice of outcome. In our study, however, parity was even lower and we also focused on immediate precursor lesions to cervical cancer. Based on our study design, where we observed a high risk of subsequent CIN3+ among women with a persistent HPV infection (30.8%), childbirth was able to increase the risk for CIN3+ on top of the strong effect of HPV persistence.
Several mechanisms have been suggested to explain the increased risk for precursor lesions or cervical cancer in relation to pregnancy and childbirth, for example, increased hormone levels and impaired immune response (Appleby et al, 2006). Furthermore, it has been shown that the transformation zone remains on the ectocervix for longer in multiparous women and thereby facilitates direct exposure to HPV and potential cofactors (Autier et al, 1996). The increased risk found in our study in relation to childbirth and not to number of pregnancies could indicate that the biological explanation is delivery-related and not pregnancy per se. Furthermore, women who had never given birth according to pregnancy (never/ever), but had had one or more abortions/ectopic pregnancies, had no increased risk of CIN3+ when compared with never pregnant women (high-risk HPV+ women: HRadj=0.93; 95% CI: 0.67–1.29) (data not shown). Local tissue damage during vaginal delivery or cellular oxidative stress with increased likelihood of DNA damage and HPV integration may be possible mechanisms (Castle, 2004; Williams et al, 2011). A role of vaginal delivery is supported by findings from a multicentre study in which an increased risk for cervical cancer was observed among HPV+ women with vaginal deliveries but not with number of abortions or among HPV+ women with caesarean sections only (Munoz et al, 2002). However, the number in the last group was small, and this aspect should be explored further. In contrast, Hildesheim et al (2001) reported no increased risk with stillbirths, refuting the hypothesis of a delivery-related mechanism. If no true difference in risk is found in relation to mode of delivery, our finding of an increased risk with giving birth but not with pregnancy might be explained by the length of pregnancy or some common biological circumstances during late pregnancy.
High levels of sex hormones appear to be involved in cervical carcinogenesis: oestrogen has been suggested to stimulate HPV gene expression, influence the cervical immune response, and stimulate cell proliferation in the transformation zone (Delvenne et al, 2007; Gariglio et al, 2009). Exposure to sex hormones is related to both parity and OC use. Pregnancy and childbirth is characterised by short-term intense exposure, whereas OC use is low-intensity and can often be a more long-term exposure. We, however, found no increased risk for CIN3+ in relation to OC use or duration of use. This is in line with previous prospective studies (Castle et al, 2002, 2005) and some case–control studies (Deacon et al, 2000; Wang et al, 2009), but in contrast to findings from studies based mainly on pooled data, in which increased risks were found with long duration of OC use (Hildesheim et al, 2001; Moreno et al, 2002; Smith et al, 2003; Castellsague et al, 2006; Appleby et al, 2007). In our study, the subgroup of women with persistent HPV infection, ever use as opposed to never use of OC, was related to a decreased risk for CIN3+ of borderline significance and a statistically significantly decreased risk was found with 4 or less years of OC use. The group of never OC users with a persistent HPV infection comprised only 28 women. We cannot explain these findings; the associations could be spurious and should be examined further before any firm conclusions are drawn. The conflicting results regarding the role of OC use in cervical carcinogenesis might be explained by different hormone levels, as the hormone levels in OCs have declined gradually since the first launch. The inherent advantages of a prospective study design as opposed to cross-sectional designs might also explain the discrepancy with previous findings. Intensive cervical cancer screening, for example, among women who use OC, may imply a higher detection and treatment of precursor lesions. However, the extent of cervical cytology testing did not differ significantly according to the covariates in our study.
We found no association between IUD use and a subsequent diagnosis of CIN3+. In a large study of pooled data from mainly case–control studies, IUD use was no longer associated with a statistically significantly decreased risk for cervical cancer when the analysis was restricted to HPV+ women (Castellsague et al, 2011). A decreased risk for adenocarcinomas was found in a smaller study of HPV+ women (Castellsague et al, 2006). It has been hypothesised that women who use IUD often are well screened, and precursor lesions are therefore more likely to be eliminated than in non-IUD users. Furthermore, IUD-induced chronic, low-grade, sterile inflammation of the local mucosa might modify HPV carcinogenesis (Castellsague et al, 2011). We also found no association with sexual behaviour, in accordance with previous case–control studies (Deacon et al, 2000; Ferrera et al, 2000; Hildesheim et al, 2001; Wang et al, 2009; Almonte et al, 2011) and a large study of pooled data (Appleby et al, 2009), but in contrast to the results of two multicentre case–control studies, which showed an increased risk for cervical cancer with decreasing age at first intercourse (Castellsague et al, 2006; Louie et al, 2009).
This is the first study presenting reproductive cofactors for developing CIN3+ among women with persistent HPV infection. However, the study had some potential limitations: the group of women with persistent infection was relatively small, and this might explain some nonsignificant findings. We also had limited statistical power to study the mode of delivery (vaginal delivery/caesarean section) or pregnancy outcome (abortion/ectopic pregnancy) separately. A larger cohort of women with persistent infections is needed to draw firm conclusions about the importance of mode of delivery or pregnancy outcome. We defined HPV persistence as being HPV+ for the same HPV genotype at the two examinations, which means that at baseline the infections had lasted for approximately 2 years. Owing to left-censoring, we did not have any further information about length of persistence, which is a potential limitation of the study. Furthermore, using our definition of HPV persistence we cannot exclude that some of the women with persistent infections had re-infections with the same HPV genotype rather than true persistent infections. A further limitation of our study is that the exposure status was captured only at baseline, and exposure status might have changed between baseline and end of follow-up; however, this potential change has most likely led to conservative estimations of the HRs.
Our study also had some strengths: it is a major strength that we are able to investigate HPV cofactors in a population of high-risk HPV DNA+ women as well as in a subgroup of women with persistent HPV infection. This implies that our results on the risk for CIN3+ cannot solely be explained by an association between the covariate and HPV acquisition or HPV persistence. Additional strengths were use of a population-based study with no prevalent disease at baseline and a long follow-up (∼13 years). This design ensured that both HPV infection and the potential cofactors were present before development of CIN3+, although it did not allow us to determine whether progression was conditional on inter-relational timing between HPV infection and the covariate. To examine this aspect of the natural history of HPV, prospective studies with many consecutive measurements of HPV and covariates are needed. Finally, we obtained follow-up information by using the unique personal identification number and the nationwide Pathology Data Bank, which is known to be almost complete and of high quality. This enabled us to conduct a prospective study with virtually no loss to follow-up.
In summary, childbirth increased the subsequent risk for immediate precursor lesions to cervical cancer, particularly among women with persistent high-risk HPV infection. No increased risk was observed with pregnancy, contraceptive use, or sexual behaviour. These findings add to the understanding of cervical carcinogenesis and this study is the first to show that childbirth contributes to the risk of cervical carcinogenesis in addition to the risk associated with persistent HPV infection.
Change history
15 January 2013
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Almonte M, Ferreccio C, Gonzales M, Delgado JM, Buckley CH, Luciani S, Robles SC, Winkler JL, Tsu VD, Jeronimo J, Cuzick J, Sasieni P (2011) Risk factors for high-risk human papillomavirus infection and cofactors for high-grade cervical disease in Peru. Int J Gynecol Cancer 21: 1654–1663
Appleby P, Beral V, Berrington de Gonzáles A, Colin D, Franceschi S, Green J, la Vecchia C, Peto J, Plummer M, Randi G, Sweetland S (2006) Cervical carcinoma and reproductive factors: collaborative reanalysis of individual data on 16,563 women with cervical carcinoma and 33,542 women without cervical carcinoma from 25 epidemiological studies. Int J Cancer 119: 1108–1124
Appleby P, Beral V, Berrington de Gonzáles A, Colin D, Franceschi S, Goodhill A, Green J, Peto J, Plummer M, Sweetland S (2007) Cervical cancer and hormonal contraceptives: collaborative reanalysis of individual data for 16,573 women with cervical cancer and 35,509 women without cervical cancer from 24 epidemiological studies. Lancet 370: 1609–1621
Appleby P, Beral V, Berrington de Gonzáles A, Colin D, Franceschi S, Green J, la Vecchia C, Peto J, Plummer M, Sweetland S (2009) Cervical carcinoma and sexual behavior: collaborative reanalysis of individual data on 15,461 women with cervical carcinoma and 29,164 women without cervical carcinoma from 21 epidemiological studies. Cancer Epidemiol Biomarkers Prev 18: 1060–1069
Autier P, Coibion M, Huet F, Grivegnee AR (1996) Transformation zone location and intraepithelial neoplasia of the cervix uteri. Br J Cancer 74: 488–490
Bobák M, Hertzman C, Škodová Z, Marmot M (2000) Own education, current conditions, parental material circumstances, and risk of myocardial infarction in a former communist country. J Epidemiol Community Health 54: 91–96
Bosch FX, Lorincz A, Munoz N, Meijer CJ, Shah KV (2002) The causal relation between human papillomavirus and cervical cancer. J Clin Pathol 55: 244–265
Castellsague X, Bosch FX, Munoz N (2002) Environmental co-factors in HPV carcinogenesis. Virus Res 89: 191–199
Castellsague X, Diaz M, de Sanjose S, Munoz N, Herrero R, Franceschi S, Peeling RW, Ashley R, Smith JS, Snijders PJ, Meijer CJ, Bosch FX (2006) Worldwide human papillomavirus etiology of cervical adenocarcinoma and its cofactors: implications for screening and prevention. J Natl Cancer Inst 98: 303–315
Castellsague X, Diaz M, Vaccarella S, de Sanjose S, Munoz N, Herrero R, Franceschi S, Meijer CJ, Bosch FX (2011) Intrauterine device use, cervical infection with human papillomavirus, and risk of cervical cancer: a pooled analysis of 26 epidemiological studies. Lancet Oncol 12: 1023–1031
Castle PE (2004) Beyond human papillomavirus: the cervix, exogenous secondary factors, and the development of cervical precancer and cancer. J Low Genit Tract Dis 8: 224–230
Castle PE, Wacholder S, Lorincz AT, Scott DR, Sherman ME, Glass AG, Rush BB, Schussler JE, Schiffman M (2002) A prospective study of high-grade cervical neoplasia risk among human papillomavirus-infected women. J Natl Cancer Inst 94: 1406–1414
Castle PE, Walker JL, Schiffman M, Wheeler CM (2005) Hormonal contraceptive use, pregnancy and parity, and the risk of cervical intraepithelial neoplasia 3 among oncogenic HPV DNA-positive women with equivocal or mildly abnormal cytology. Int J Cancer 117: 1007–1012
Deacon JM, Evans CD, Yule R, Desai M, Binns W, Taylor C, Peto J (2000) Sexual behaviour and smoking as determinants of cervical HPV infection and of CIN3 among those infected: a case–control study nested within the Manchester cohort. Br J Cancer 83: 1565–1572
Delvenne P, Herman L, Kholod N, Caberg JH, Herfs M, Boniver J, Jacobs N, Hubert P (2007) Role of hormone cofactors in the human papillomavirus-induced carcinogenesis of the uterine cervix. Mol Cell Endocrinol 264: 1–5
Ferrera A, Velema JP, Figueroa M, Bulnes R, Toro LA, Claros JM, de BO, Melchers WJ (2000) Co-factors related to the causal relationship between human papillomavirus and invasive cervical cancer in Honduras. Int J Epidemiol 29: 817–825
Gargano JW, Nisenbaum R, Lee DR, Ruffin MT, Steinau M, Horowitz IR, Flowers LC, Tadros TS, Birdsong G, Unger ER (2012) Age-group differences in human papillomavirus types and cofactors for cervical intraepithelial neoplasia 3 among women referred to colposcopy. Cancer Epidemiol Biomarkers Prev 21: 111–121
Gariglio P, Gutierrez J, Cortes E, Vazquez J (2009) The role of retinoid deficiency and estrogens as cofactors in cervical cancer. Arch Med Res 40: 449–465
Hildesheim A, Herrero R, Castle PE, Wacholder S, Bratti MC, Sherman ME, Lorincz AT, Burk RD, Morales J, Rodriguez AC, Helgesen K, Alfaro M, Hutchinson M, Balmaceda I, Greenberg M, Schiffman M (2001) HPV co-factors related to the development of cervical cancer: results from a population-based study in Costa Rica. Br J Cancer 84: 1219–1226
Iftner T, Villa LL (2003) Chapter 12: human papillomavirus technologies. J Natl Cancer Inst Monogr 80–88
Jensen KE, Schmiedel S, Frederiksen K, Norrild B, Iftner T, Kjaer SK (2012) Risk for cervical intraepithelial neoplasia grade 3 or worse in relation to smoking among women with persistent human papillomavirus infection. Cancer Epidemiol Biomarkers Prev 21: 1959–1965
Kjaer S, Høgdall E, Frederiksen K, Munk C, van den BA, Svare E, Meijer C, Lorincz A, Iftner T (2006) The absolute risk of cervical abnormalities in high-risk human papillomavirus-positive, cytologically normal women over a 10-year period. Cancer Res 66: 10630–10636
Kjaer SK (2007) Human papillomavirus (HPV) infection, cervical cancer and vaccination against HPV: a Nordic perspective. Acta Obstet Gynecol Scand 86: 1286–1289
Kjaer SK, Frederiksen K, Munk C, Iftner T (2010) Long-term absolute risk of cervical intraepithelial neoplasia grade 3 or worse following human papillomavirus infection: role of persistence. J Natl Cancer Inst 102: 1478–1488
Klug SJ, Molijn A, Schopp B, Holz B, Iftner A, Quint W, Snijders JF, Petry KU, Kruger KS, Munk C, Iftner T (2008) Comparison of the performance of different HPV genotyping methods for detecting genital HPV types. J Med Virol 80: 1264–1274
Liao SF, Lee WC, Chen HC, Chuang LC, Pan MH, Chen CJ (2012) Baseline human papillomavirus infection, high vaginal parity, and their interaction on cervical cancer risks after a follow-up of more than 10 years. Cancer Causes Control 23: 703–708
Louie KS, de Sanjose S, Diaz M, Castellsague X, Herrero R, Meijer CJ, Shah K, Franceschi S, Munoz N, Bosch FX (2009) Early age at first sexual intercourse and early pregnancy are risk factors for cervical cancer in developing countries. Br J Cancer 100: 1191–1197
Moreno V, Bosch FX, Munoz N, Meijer CJ, Shah KV, Walboomers JM, Herrero R, Franceschi S (2002) Effect of oral contraceptives on risk of cervical cancer in women with human papillomavirus infection: the IARC multicentric case-control study. Lancet 359: 1085–1092
Munoz N, Franceschi S, Bosetti C, Moreno V, Herrero R, Smith JS, Shah KV, Meijer CJ, Bosch FX (2002) Role of parity and human papillomavirus in cervical cancer: the IARC multicentric case–control study. Lancet 359: 1093–1101
Schiffman M, Wentzensen N, Wacholder S, Kinney W, Gage JC, Castle PE (2011) Human papillomavirus testing in the prevention of cervical cancer. J Natl Cancer Inst 103: 368–383
Smith JS, Green J, Berrington de GA, Appleby P, Peto J, Plummer M, Franceschi S, Beral V (2003) Cervical cancer and use of hormonal contraceptives: a systematic review. Lancet 361: 1159–1167
Wang SS, Zuna RE, Wentzensen N, Dunn ST, Sherman ME, Gold MA, Schiffman M, Wacholder S, Allen RA, Block I, Downing K, Jeronimo J, Carreon JD, Safaeian M, Brown D, Walker JL (2009) Human papillomavirus cofactors by disease progression and human papillomavirus types in the study to understand cervical cancer early endpoints and determinants. Cancer Epidemiol Biomarkers Prev 18: 113–120
Williams VM, Filippova M, Soto U, Duerksen-Hughes PJ (2011) HPV-DNA integration and carcinogenesis: putative roles for inflammation and oxidative stress. Fut Virol 6: 45–57
Acknowledgements
This work was supported by the National Institutes of Health (Grant RO1 CA47812), the Mermaid project (MERMAID-2), Savværksejer Jeppe Juhl og Hustru Ovita Juhls Mindelegat, and the Danish Cancer Society. Innogenetics Inc. (Gent, Belgium) provided INNO-LiPAv2 HPV prototype assay kits for HPV testing free of charge.
Author information
Authors and Affiliations
Corresponding author
Additional information
This work is published under the standard license to publish agreement. After 12 months the work will become freely available and the license terms will switch to a Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License.
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Jensen, K., Schmiedel, S., Norrild, B. et al. Parity as a cofactor for high-grade cervical disease among women with persistent human papillomavirus infection: a 13-year follow-up. Br J Cancer 108, 234–239 (2013). https://doi.org/10.1038/bjc.2012.513
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bjc.2012.513
Keywords
This article is cited by
-
Establishment of multifactor predictive models for the occurrence and progression of cervical intraepithelial neoplasia
BMC Cancer (2020)
-
High frequency of HPV genotypes 59, 66, 52, 51, 39 and 56 in women from Western Mexico
BMC Infectious Diseases (2020)
-
Comparison of cure rates in women treated with cold-coagulation versus LLETZ cervical treatment for CIN2-3 on pretreatment cervical punch biopsies: a retrospective cohort study
Archives of Gynecology and Obstetrics (2017)
-
Conisation as a marker of persistent human papilloma virus infection and risk of breast cancer
British Journal of Cancer (2016)
-
Socio-demographic and reproductive determinants of cervical neoplasia in seven sub-Sahara African countries
Cancer Causes & Control (2016)
