

Key Points
- Esophageal motility is best evaluated using a combination of endoscopy and barium x-ray study.
- In achalasia, endoscopy helps to rule out gastroesophageal junction malignancy.
- In scleroderma, endoscopic findings relate to a hypotensive lower esophageal sphincter.
- In the spastic disorders of the esophagus, endoscopy is often normal.
- Esophageal diverticula are seen by endoscopy but best diagnosed by barium swallow.
- Eosinophilic esophagitis is diagnosed by biopsy at the time of endoscopy. Patients with eosinophilic esophagitis and other ringed esophagi are at risk for tears or perforation during endoscopic dilation.
Introduction
The evaluation of esophageal motility disorders often begins with endoscopy. Many diagnoses can be made with endoscopy alone, although some require manometry or barium x-ray study for confirmation. This review discusses the endoscopic findings of achalasia, scleroderma, nutcracker esophagus, diffuse esophageal spasm, diverticula, eosinophilic esophagitis, and ringed esophagus.
Achalasia
Achalasia is an uncommon disorder that involves loss of neurons or ganglion cells in the myenteric plexus of the lower esophageal sphincter (LES) and the body of the esophagus. These neurons allow relaxation of the LES through inhibition of the normally contracted LES smooth muscle, and their loss can lead to the failure of the LES to relax with swallowing. A full description of the pathophysiologic basis of achalasia can be found in other sections of this publication.
Symptoms of achalasia include dysphagia to both solids and liquids, regurgitation chest pain, and weight loss.1, 2
Diagnosis of achalasia lies in findings on manometry, barium esophagram, and endoscopy. Many of these findings are similar whether the disease is primary or secondary, for instance due to Chagas disease or malignancy at the gastroesophageal junction (GEJ). Manometry is the most important diagnostic test. It typically shows absent or incomplete relaxation of the LES with wet swallows and aperistalsis (no smooth muscle contractions or simultaneous contractions of the body of the esophagus after wet swallows). A higher LES resting pressure is also often seen.
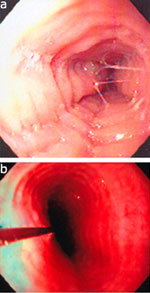
Barium swallow typically shows a dilated esophagus with a "bird's beak" narrowing distally due to the contracted LES. Late in the disorder, the esophagus is severely dilated and takes on the contortions of a "sigmoid" shape (Figure 1a). This results from longstanding aperistalsis and the lack of LES relaxation.
Figure 1: a: Barium esophagram showing a dilated, tortuous esophagus and a "bird's beak" appearance of the lower esophageal sphincter (LES).
![Figure 1 : a: Barium esophagram showing a dilated, tortuous esophagus and a |[ldquo]|bird's beak|[rdquo]| appearance of the lower esophageal sphincter (LES). Unfortunately we are unable to provide accessible alternative text for this. If you require assistance to access this image, or to obtain a text description, please contact npg@nature.com](/gimo/contents/pt1/thumbs/gimo29-f1.jpg)
b: Endoscopy in this same patient with late-stage achalasia showing a dilated, "sigmoid" shaped esophagus. (Source: Courtesy of Drew Schembre, M.D.)
In patients with suspected achalasia, endoscopy is performed to exclude pseudoachalasia, that is, GEJ tumors that can mimic primary achalasia. In patients not known to have achalasia, for instance in a patient undergoing esophagogastroduodenoscopy (EGD) to evaluate regurgitation or chest pain, the diagnosis can be suggested by a constellation of findings, including a feeling of resistance at the LES that suddenly gives way, with the endoscope "popping" into the stomach, due to the contracted LES smooth muscle.
The spectrum of endoscopic findings worsens as the disease progresses, from a normal-appearing esophagus1, 2 to a dilated and tortuous "sigmoid" esophagus (Figure 1b). There is often retained fluid or food and a longer period of fasting prior to endoscopy may be needed (Figure 2). The mucosa of the esophagus often appears normal, but stasis of fluid, food, or pills may cause friability, erosions, or Candida esophagitis (Figure 3).
Figure 2: Dilated, fluid-filled esophagus in a patient with achalasia.
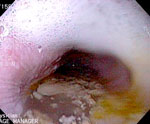
(Source: Courtesy of Drew Schembre, M.D.)
Cameron et al.3 used videoendoscopy to evaluate achalasia. A standard endoscope was passed to 25 cm, and then to just proximal to the LES. The patients were videotaped during swallowing. Lumen-occluding peristaltic contractions were seen in only 1 of 20 patients with achalasia. This absence of peristalsis was also seen in patients with scleroderma.
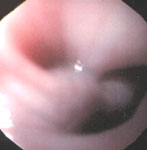
The LES can appear puckered and may not open with air insufflation (Figure 4).3 However, with gentle pressure, the endoscope should pass easily. If more pressure is needed to cross the GEJ, pseudoachalasia due to a malignancy should be suspected.4
Endoscopy plays a crucial role in ruling out mechanical stricture and malignancy. However, despite a careful evaluation of the distal esophagus and cardia, a tumor can be missed in more than one third of patients because of submucosal growth.4, 5 Biopsies, although important, can also be negative because of the infiltrative nature of some of these tumors. If a malignancy is suspected, patients should undergo testing with computed tomography scan or endoscopic ultrasound (EUS). Even with additional testing, some tumors remain elusive.4, 6
Endoscopic ultrasound may be helpful in evaluating for malignancy by showing esophageal wall thickness and disruption of the normal wall architecture. However, a thickened wall can be seen near the GEJ in patients with primary achalasia.7, 8, 9 Some of this may be due to a tangential imaging artifact in patients with a tortuous esophagus.10, 11
Scleroderma
Scleroderma causes abnormalities of the autonomic nervous system, microvasculature, and immune system, and causes smooth muscle atrophy and fibrosis. Though patients with scleroderma often present with skin changes, calcinosis, and Raynaud's phenomenon, 90% have gastrointestinal involvement. Half are symptomatic. Esophageal abnormalities are the most common gastrointestinal abnormality, with manometry showing low amplitude or absent peristalsis in the middle and distal esophagus and a low LES pressure. The proximal one third of the esophagus, with its striated muscle, is spared.
Symptoms include heartburn, dysphagia due to stricture or esophageal dysmotility, and pain due to diffuse spasm.
Endoscopic findings include a patulous GEJ (Figure 5), esophagitis, and even Barrett's esophagus due to the hypotensive LES, stricture due to reflux, a hypotonic esophagus, or Candida esophagitis due to stasis. Although Ling and Johnston12 found that endoscopy was not a sensitive means to evaluate the esophagus in connective tissue disease patients, especially when compared with manometry, at videoendoscopy, Cameron et al.3 noted that the LES remained widely open in 12 of 13 patients with scleroderma. Ten of 13 scleroderma patients showed a typical motility abnormality consisting of a normal contraction in the upper esophagus and no contraction in the middle and distal esophagus.3
Figure 5: Retroflexed view showing a patulous gastroesophageal junction in a patient with scleroderma.

(Source: Courtesy of Drew Schembre, M.D.)
Spastic Disorders of the Esophagus
Diffuse esophageal spasm (DES) or "corkscrew" esophagus and nutcracker esophagus are diagnosed by manometry, with DES showing abnormal simultaneous contractions in the esophageal body and nutcracker esophagus characterized by extremely high-amplitude distal esophageal contractions (mean greater than 180 mmHg). Both cause intermittent dysphagia to liquids and solids, and chest pain, which can radiate to the arms or back. The pain can be precipitated with eating, but can also occur at other times.12, 13, 14 Diffuse esophageal spasm can sometimes be seen at the time of endoscopy as a "corkscrew" appearance in the distal esophagus.14 Nutcracker esophagus often appears normal at endoscopy (Figure 6). A careful look for signs of reflux such as erosions, ulcerations, or strictures is required as gastroesophageal reflux disease may be an underlying cause of these two spastic abnormalities.15

Esophageal Diverticula
Esophageal diverticula are caused by pulsion or traction, much like diverticula elsewhere in the gastrointestinal tract. Esophageal stricture or dysmotility abnormalities such as achalasia or a hypertensive upper or lower esophageal sphincter cause increased intraluminal pressure and diverticula due to pulsion. Inflammatory processes like tuberculosis or malignancy can cause adhesions and diverticula due to traction.
A discussion of esophageal diverticula is included in this chapter because they can result from dysmotility, and because the primary symptom of esophageal diverticula is dysphagia.
Diverticula can occur in any part of the esophagus. Zenker's diverticula form above the upper esophageal sphincter in the midline posteriorly at the pharyngoesophageal junction, through a weak spot between the muscles known as Killian's triangle or hiatus. Diverticula can also occur in the mid-esophagus (pulsion or traction) and distal esophagus (pulsion), called epiphrenic diverticula and located just above the LES (Figure 7).16, 17, 18, 19

Zenker's diverticula typically occur in older patients and cause progressive symptoms of regurgitation of food, dysphagia, pulmonary aspiration, halitosis, gurgling in the throat, or even a neck mass.16, 17, 18, 19
Mid-esophageal and epiphrenic diverticula may be asymptomatic or may cause regurgitation, cough, aspiration, chest pain, dysphagia or even cardiac arrhythmias due to pressure on the left atrium.17, 18, 20, 21 Some of these symptoms may be due to the underlying motility disorder that led to the diverticulum formation.
Zenker's diverticula are seen proximal to the cricopharyngeal muscle, and this muscle can be seen endoscopically to form a "bridge" between the esophagus and the diverticulum (Figure 8). This bridge is particularly well seen after careful passage of a nasogastric tube, a technique utilized during endoscopic intraluminal treatment of Zenker's diverticula.22
Figure 8: Zenker's diverticulum.
The diverticulum is on the right and the true esophageal lumen is on the left. They are separated by a "bridge" of tissue.
Pulsion diverticula consist of mucosa and submucosa only, and endoscopically appear round with a wide neck. Traction diverticula, which often occur in the mid-esophagus, contain all layers of the esophageal wall and have a tented shape, that is, small diverticula with a large neck.16, 17 However, endoscopy is not very sensitive. Esophageal diverticula are well seen on barium x-ray examination (Figure 9), and this is the best choice for diagnosis. Manometry may reveal an underlying motility disorder, but does not aid diagnosis of the diverticula themselves.

Esophageal diverticula may lead to nasogastric tube curling and improper placement or even iatrogenic perforation. Perforation can also occur with endoscopy. When performing endoscopy on a patient with a known Zenker's diverticulum, the endoscope should be placed carefully under direct visualization.16, 23 Very little pressure should be used, and if the diverticulum is entered, the endoscope tip should be slowly withdrawn out of the diverticulum, and then gently torqued clockwise to find the esophageal lumen.23
Eosinophilic Esophagitis
Eosinophilic esophagitis is a disease seen in both the pediatric population and adults. Though not a motility disorder per se, because of its common symptom of dysphagia, it is discussed in this chapter.
Esophageal abnormalities and symptoms are partly due to chronic inflammation. There is a male predominance.24, 25, 26, 27 Though most patients are younger, there is a report of a patient as old as 85 years.28
Most patients have a history of atopy (hay fever, asthma, peanut allergy),24, 29 and with the increase in allergic disease in the general population, the incidence of eosinophilic esophagitis may rise as well.30 Symptoms include dysphagia and food impaction, and patients may or may not respond to treatment for gastroesophageal reflux disease (GERD) such as H2 blockers and proton pump inhibitors, or to dilation.24, 29, 30
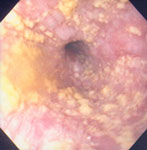
Diagnosis is made by biopsy at the time of endoscopy. Multiple biopsies should be taken from both the upper and lower esophagus, as the disease is patchy. Biopsies show greater than 15 to 20 eosinophils per high-power field , considerably more than is seen with GERD.24, 29, 30, 31, 32 Endoscopic findings are variable. The esophagus may appear normal24, 28 or show a subtle loss of vascularity.29, 32 The most common abnormality is a white exudate, varying from fine reticular lines or tiny nodules to scales and patches or even nodularity or plaques.29, 32, 33 These white lesions can be mistaken for Candida esophagitis but are actually clumps of eosinophils.32, 33
Focal proximal strictures28 or linear folds and furrows can be seen, or even a small caliber esophagus due to a long-segment esophageal stricture.25, 32, 34
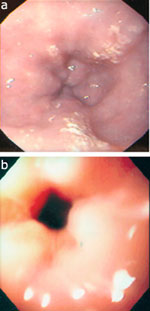
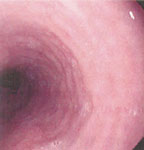
Esophageal rings, both in the proximal and distal esophagus, are also common. The rings are 1 to 2 cm apart and are fixed, that is, they do not disappear with air insufflation (Figure 10).31, 35, 36 The esophagus is variously called corrugated ringed esophagus,25, 32, 37 trachealized esophagus,37 multiple esophageal rings,26, 27, 31, 36 ringed esophagus,35 or feline esophagus.24, 38
Figure 10: Multiple esophageal rings.
a: In a man with asthma. b: In a 24-year-old man with exercise induced asthma and allergic rhinitis.
The latter term is particularly confusing, as many authors18, 25, 31, 39 use the term felinization to describe a normal endoscopic variant, defining it as transient, fine, circumferential esophageal folds, 1 to 2 mm in thickness and symmetric, predominately in the distal two thirds of the esophagus (Figure 11).39 The folds disappear with air overinsufflation. When it is defined in this way, Kundrotas et al.39 found esophageal felinization in 24% of 280 unselected endoscopies. There were no associated symptoms and no correlation to age, sex, or other endoscopic findings.
Eosinophilic esophagitis is extremely important to recognize, through the history, symptoms, and endoscopic findings, as patients are at a higher risk of perforation with dilation or even with simple endoscopy.24, 25, 26, 27, 34, 37 Mucosal shearing or rents can be seen as the endoscope is withdrawn after diagnostic endoscopy.24, 34, 38 Endoscopy should be performed cautiously in these patients, and dilations, if done, should begin with small-caliber dilators.25, 27, 36
Other Ringed Esophagus
Multiple fixed esophageal rings can also be seen in patients who do not have eosinophilic esophagitis, and may be due to gastroesophageal reflux disease or other causes.35, 40 Again, multiple terms are used, including multiple esophageal rings,40 corrugated esophagus, feline esophagus, etc. With these patients, also, extreme care must be taken with dilation.40
Conclusion
Though not the sole diagnostic tool, endoscopy is used in conjunction with esophageal manometry and barium x-rays to evaluate patients with esophageal motility disorders. Endoscopic findings are less helpful in scleroderma and the spastic disorders of nutcracker esophagus and diffuse esophageal spasm, as the findings are often normal with these entities. Endoscopy is helpful in diagnosing diverticula and ringed esophagus. It is mandatory in achalasia to aid exclusion of malignancy. The diagnosis of eosinophilic esophagitis is made by endoscopy and biopsy.
