

Key Points
- Nonerosive reflux disease (NERD) is the most common phenotypic presentation of gastroesophageal reflux disease (GERD).
- Although definition of NERD remains an area of controversy, many studies continue to define these patients as having classic symptoms of GERD in the absence of esophageal mucosal injury.
- As compared with patients with erosive esophagitis, NERD patients tend to be younger, female, and lack hiatal hernia.
Introduction
Symptoms of gastroesophageal reflux disease (GERD) are very common, affecting up to 20% of the population in North America, 9% to 17% of Europe, 12% to 15% of Australia, and 2% to 5% of Asia once a week.1 Nonerosive reflux disease (NERD) is the most common presentation of GERD. Traditionally, it has been assumed that patients with GERD symptoms who lack esophageal mucosal injury represent a mild form of the disease. Consequently, a much more conservative therapeutic approach has been suggested to be adequate for these patients. However, there are very little data to support such a strategy, because most of the well-designed therapeutic trials in GERD during the last two decades have focused primarily on mucosal healing and symptom improvement in patients with erosive esophagitis.
In recent years, at least three important developments have emerged in the field of GERD that have shifted our attention back to those patients with normal esophagus and typical symptoms of GERD. First, it has been observed that most of the community-based GERD patients appear to have no evidence of esophageal mucosal injury. Second, recent therapeutic trials have demonstrated that NERD patients have a lower symptom response rate to proton pump inhibitors (PPIs) taken once daily as compared with patients with erosive esophagitis. Third, there have been recent profound changes in the management of GERD in gastrointestinal (GI) practice. Currently, gastroenterologists have to cope with a growing number of GERD patients, who are referred because of continuation of GERD-related symptoms, despite treatment with a PPI (PPI failure). Most of these patients originate from the NERD group.
Definition
Patients with classic symptoms of GERD and normal esophageal mucosa have been classified as having endoscopy-negative reflux disease (ENRD), symptomatic GERD, or NERD.2 Consequently, a group of experts at the Genval Workshop on Reflux Management3 offered the following definition of patients with NERD: "These are individuals who satisfy the definition of GERD but do not have either Barrett's esophagus or definite endoscopic esophageal breaks." A similar definition, proposed by Waring,4 is "burning retrosternal discomfort for at least three months, but with normal esophageal mucosa on upper endoscopy." Both definitions assume that all patients who present with heartburn have GERD, regardless of whether there is esophageal mucosal injury. However, as data accumulate regarding mechanisms leading to heartburn, it appears that the latter assumption is unfounded. In fact, recent studies have demonstrated that acid is not the only intraesophageal stimulus that leads to heartburn symptoms. Non-acid-related stimuli (volume, esophageal motor event, nonacidic reflux, etc.) may trigger classic symptoms of GERD as well. Thus, the axiom "no acid, no heartburn" should be considered obsolete. Heartburn appears to be a cortical perception of a variety of intraesophageal events, of which acid reflux is only one.5
Subjects with heartburn and normal esophageal mucosa probably represent a heterogeneous group of patients of whom most, but not all, have gastroesophageal reflux (GER)-related disorder. Only those with symptoms owing to GER should be considered as having NERD. Thus, the proposed definition for NERD by Fass et al.6 is the presence of typical symptoms of GERD owing to intraesophageal reflux in the absence of visible esophageal mucosal injury on endoscopy. Clearly, the main limitation in determining the presence of GERD is the lack of a "gold standard" for diagnosing it. Until better diagnostic modalities are available for GERD, the full spectrum of NERD will remain unknown.
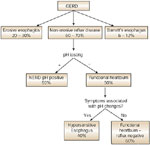
Nonerosive reflux disease affects a heterogeneous group of patients. One of the subgroups includes those patients who have been termed as having functional heartburn. The Rome II committee for functional esophageal disorders defined functional heartburn as an episodic retrosternal burning in the absence of pathologic GERD, pathology-based motility disorders, or structural explanations.7 This definition is vague and clearly does not provide any clues to the different underlying mechanisms that may lead to heartburn in these patients. However, studies have demonstrated that functional heartburn also affects a heterogeneous group of patients. When using pH testing and a therapeutic trial with a PPI, two main subgroups emerge. The first subgroup demonstrates either a close relationship between symptoms and acid reflux events or minute changes in pH (pH changes that do not reach pH 4) and thus are termed the hypersensitive esophagus. The second and larger subgroup (up to 60%) includes patients with classic heartburn but with no evidence that acid reflux or any pH changes are the underlying cause. These patients are likely to have heartburn owing to non-acid-related stimuli. Consequently, the future definition of NERD may include the hypersensitive esophagus subgroup and exclude those with heartburn symptoms unrelated to esophageal pH changes as in the functional heartburn group. Figure 1 depicts the subclassification of GERD and NERD.
History of the Disease
Most of the studies that assessed the natural history of NERD provide very limited information owing to various shortcomings. For example, it is not unusual in these studies to allow patients to continue to consume various antireflux compounds. The baseline status of the GERD patients is retrospectively assessed, regular follow-up is unusual, and prospective design is uncommon.
Kuster et al.8 followed 107 patients with GERD, of whom 33 had endoscopically documented erosive esophagitis. The authors used a step-up approach in which patients initially received antacids and prokinetics, and if symptoms continued, an H2-blocker was prescribed. Patients who did not respond to an H2-blocker were referred for antireflux surgery. At 3 years of follow-up, 107 patients were available for evaluation, and of those, 52% required only antacids plus prokinetics to control their symptoms. At 6-year follow-up, 89 patients were available for evaluation and, of those, 55% required only antacids plus prokinetics to control their symptoms. Regardless of therapy, only 2.7% of the NERD patients developed erosive esophagitis after 3 years and 3% after 6 years of follow-up. This study provided a relatively longer duration of follow-up and, despite its limitations, very few NERD patients progressed to develop esophageal mucosal injury. Isolauri et al.9 conducted a longer duration follow-up (17 to 22 years, mean 19.5 years) of 60 patients with documented GERD. Patients received medical (n = 50) or surgical (n = 10) antireflux therapy as needed (no standardization). Of the 50 subjects who received only medical therapy, 30 had NERD and 20 erosive esophagitis at baseline. At follow-up, only 5 (17%) of the NERD patients progressed to develop erosive esophagitis (all to grade 1 Savary-Miller).
A recent retrospective study from the Hines Veterans Administration Medical Center reported 2306 GERD patients having at least two separate upper endoscopies during a mean follow-up of 7 years.10 The authors reported that the endoscopic findings of 69% of the patients remained unchanged, 21% improved, and 11% worsened. Additionally, endoscopic findings among untreated patients were similar between baseline and follow-up. Most importantly, discontinuing medical therapy resulted in return to the pretreatment esophageal mucosal status.
McDougall et al.11 conducted a 10-year follow-up of 152 patients with typical GERD symptoms and grade 1 to 3 erosive esophagitis (modified Savary-Miller) documented during an upper endoscopy. Over 70% of the patients still had heartburn daily or at least weekly at follow-up. Patients reporting dysphagia underwent repeat endoscopy, revealing two new benign peptic strictures and one Barrett's esophagus. However, because this was a survey study and patients were allowed to be on and off treatment ad libitum, it is difficult to interpret the findings. Furthermore, the presence of so-called new Barrett's esophagus may well be an unrecognized Barrett's mucosa that was obscured by esophageal inflammation. In another study, McDougall et al.12 performed a prospective follow-up of 101 GERD patients for a period of at least 32 months after initial assessment with pH testing and an upper endoscopy. During follow-up more than half of the patients were on a PPI or H2-blocker. Of the 17 subjects with NERD and abnormal pH testing, 4 (24%) developed erosive esophagitis while on a histamine-2 receptor antagonist. This study is commonly used by proponents of the spectrum-continuum concept to demonstrate that a significant number of NERD patients progress over time to develop esophageal inflammation. However, the study included a small number of subjects who were followed long term. Again, the authors' claim in this study that three patients with erosive esophagitis developed Barrett's esophagus may also represent an unrecognized Barrett's mucosa that was obscured by the esophageal inflammation.
Manabe et al.13 followed 105 patients with mild erosive esophagitis (Los Angeles classification A and B) for a mean duration of 5.5 years. Only 10.5% of the patients progressed to higher grading (mostly Los Angeles grade C) and none has progressed to Barrett's esophagus. This study suggests that even within the different gradings of erosive esophagitis there is very little progression over time.
In a publication by Pace et al.,14 which was a long-term follow-up of a previously published short-term follow-up study, the authors claimed that 94% of NERD patients progressed to develop erosive esophagitis after 5 years of follow-up. The authors concluded that the natural history of NERD is that the majority of the patients progress, albeit relatively rapidly, to develop erosive esophagitis. These unusual results fly in the face of the current literature as well as the common GI practice experience, which further substantiates the impression that the study by Pace et al.15 included from the start a large number of patients with healed erosive esophagitis, who were erroneously considered as having NERD. In their original article the authors stated that the study consisted of a retrospective analysis of 33 outpatients. The original article lacks any information on how the diagnosis of NERD was made, what grading system was used to describe esophageal mucosal involvement, and, in particular, if patients were receiving any antireflux treatment prior to first endoscopy. These shortcomings, in addition to the evaluation of a patient population from a tertiary-care referral center, may have led to the authors' conclusion that NERD is just a temporary anatomic finding in GERD patients who will rapidly progress along the spectrum.
Lastly, thus far we are lacking prospective reports demonstrating progression of NERD patients to Barrett's esophagus or adenocarcinoma of the esophagus. Figure 2 depicts the natural course of NERD as we currently understand it.

Epidemiology
Early studies reported that approximately 50% of patients with heartburn were found to exhibit normal esophageal mucosa during endoscopy.16, 17 However, several community-based European studies of NERD found a much higher prevalence of 70%.18 Galmiche et al.19 assessed the efficacy of on-demand H2-receptor antagonist therapy in patients with GERD symptoms who were recruited from general practice clinics. A total of 423 patients were included in the intent-to-treat analysis of this study; 71% met the criteria for NERD. Carlsson et al.20 compared different treatment strategies for GERD at 36 primary care centers in Europe and Australia and noted that 49% of the 538 enrolled patients lacked esophageal mucosal breaks. In the United States, Robinson et al.21 evaluated only subjects who used antacids for symptomatic relief of heartburn. Of 165 patients enrolled in this study, 53% had normal esophageal mucosa on upper endoscopy. Overall, the results of studies investigating NERD have suggested that its prevalence is between 50% and 70% of the GERD population. In Asia, NERD affects up to 65% of the Indians, 72% of the Malay, and 60% to 90% of the Chinese in studies from Malaysia, Singapore, China, and Hong Kong22 (Figure 3).

Among patients with NERD, between 30% and 50% have normal 24-hour esophageal pH monitoring, defined by duration of acid exposure (pH <4) over a period of 24 hours, and thus meet the diagnostic criteria set for functional heartburn.5, 18, 23, 24 In a recent study, Martinez et al.25 evaluated 71 NERD patients and demonstrated that in 50% who underwent pH testing, normal distal esophageal acid exposure was present. Of those with functional heartburn, approximately 40% have the hypersensitive esophagus.
However, we also should consider that most patients with GERD symptoms never seek medical attention. It is still unknown what percentage of these nonpresenters has NERD or functional heartburn. Additionally, there are very few studies that can shed light on the clinical characteristics of NERD, particularly compared with erosive esophagitis. A large study involving 25 centers in Denmark and Sweden reported on 424 patients with troublesome heartburn associated with NERD. The mean age of the population was 50 years, 58% were female, only 21% were smokers, 45% were active alcohol users, 52% had more than a 5-year history of heartburn, and in only 37% a hiatal hernia was documented during upper endoscopy.26 Carlsson et al.20 compared the clinical characteristics of patients with NERD and those with erosive esophagitis. In the NERD group, 62% were female, the mean age was 48 years, the mean weight was 79 kg for males and 69 kg for females, 24% were smokers, 58% were alcohol consumers, 75% had symptom duration longer than 12 months, 56% had a hiatal hernia, and 26% were positive for Helicobacter pylori. Although not demonstrated in the studies above, pooled data from two other studies suggest that patients with erosive esophagitis are significantly older than those with NERD.27
Pathophysiology
Physiologic studies in NERD patients demonstrated minimal abnormalities when compared to normal subjects (Table 1). Nonerosive reflux disease patients have a slightly higher rate of failed peristaltic contractions, defined as nontransmitted contractions or contraction waves that do not traverse the entire esophagus. Additionally, NERD patients demonstrate mildly reduced mean lower esophageal sphincter (LES) resting pressure and distal amplitude contractions as compared with normal subjects.28 Hiatal hernia is a relatively uncommon anatomic finding in NERD patients as compared with patients with erosive esophagitis or Barrett's esophagus. Cameron29 reported that the hiatal hernia prevalence among NERD patients is only 29% as compared to 71% of the erosive esophagitis and up to 96% of the long-segment Barrett's esophagus patients. The rarity of hiatal hernia suggests that transient lower esophageal sphincter relaxation (TLESR) is the predominant underlying mechanism for GER in patients with NERD.

Patients with NERD demonstrate the lowest esophageal acid exposure profile as compared with patients with erosive esophagitis or those with Barrett's esophagus. They have the lowest total, supine, and erect time with pH <4 as well as total number of acid reflux events. Only 45% of the NERD patients demonstrate abnormal values during pH testing as compared with 75% of the patients with erosive esophagitis and 92% of those with Barrett's esophagus.25 However, a recent study revealed that the percent overlap in esophageal acid exposure between patients with NERD and abnormal pH test and those with Barrett's esophagus was 31.6% for total time, 37.5% for upright time, and 20.8% for supine time.30 Furthermore, the percent overlap between NERD patients with abnormal pH and those with erosive esophagitis was 47.7% for total time, 64.7% for upright time, and 81.8% for supine time (Table 2).
Cicala et al.31 assessed the intraesophageal distribution and perception of acid reflux in patients with NERD, erosive esophagitis, and healthy controls. Independent of the duration of acid exposure in the distal esophagus, NERD patients were found to have a significantly higher proximal spread of acid reflux and a higher sensitivity to short-duration reflux episodes when compared with erosive esophagitis patients (odds ratio = 11). The highest proximal acid exposure and consequently symptom perception was noted in functional heartburn patients (normal endoscopy and normal pH testing) and to a lesser extent in NERD patients with abnormal pH testing. Weusten et al.32 demonstrated in NERD patients with an abnormal pH testing and a positive correlation between GERD symptoms and acid reflux events that both duration of esophageal acid exposure and the proximal migration of the refluxate were essential determinants in the perception of acid reflux.
By using the results of 24-hour esophageal pH monitoring, NERD patients can be subdivided into two main subgroups: patients with a pathologic and patients with a normal esophageal acid exposure. In the former group, studies with magnification endoscopy have demonstrated minimal very distal esophageal breaks in about 40% of the patients.33 The meaning of these minute esophageal breaks, which tend to improve after antireflux treatment, remains unclear, but the findings were used by some authorities to suggest that the distinction between erosive esophagitis and NERD may not be well defined. The group of NERD patients with normal pH testing, termed functional heartburn, is further subdivided into two additional subgroups according to symptom index (SI), a clinical tool commonly used to determine the relationship between symptoms and acid reflux events. The first subgroup includes functional heartburn patients with a positive SI, and the second subgroup includes functional heartburn patients with a negative SI. The former NERD subgroup displays hypersensitivity to physiologic amounts of acid and thus was termed the sensitive (or hypersensitive) esophagus.34, 35, 36, 37 These patients have also demonstrated an abnormal perception threshold for pain during esophageal balloon distention in comparison with normal controls, suggesting that the underlying mechanism for symptoms is visceral hypersensitivity.35 Martinez et al.38 demonstrated that 55% of 71 NERD patients had a negative pH test and of those 32% had positive SI. Patients with the hypersensitive esophagus demonstrate a very limited response to standard-dose PPI treatment but with some improvement when higher doses are used.39 Patients with functional heartburn and negative SI are rarely responsive to any antireflux intervention. Mechanisms for heartburn in this group of patients are mostly speculative and may include nonacidic reflux, bile, esophageal motor abnormality, or hypersensitivity to mechanical stimuli.
Overall, interpretation of a positive SI in the setting of a negative pH test remains an area of controversy. Some experts suggest that a positive SI is indicative of a false-negative pH test, whereas others consider it as indicative of visceral hypersensitivity. In general, patients with erosive esophagitis are more likely (65%) to have a positive SI than patients with normal endoscopy and positive (32.5%) or negative (21%) pH testing.40
Repeated studies in patients with functional heartburn, using either esophageal balloon distention or electrical stimulation, have consistently demonstrated a lower perception threshold for pain as compared to patients with other presentations of GERD.41 Furthermore, objective neurophysiologic measures of esophageal evoked potentials latency revealed that functional heartburn patients achieve equivalent latency and amplitude responses with reduced afferent input, suggesting heightened esophageal sensitivity.41 By contrast, stimulus response functions to acid in patients with functional heartburn gave mixed results. Rodriguez-Stanley et al.42 reported that 90% of functional heartburn patients experienced abnormal responses to esophageal balloon distention, intraesophageal acid perfusion (Bernstein test), or both. In contrast, Fass et al.43 demonstrated a higher mean value for time to heartburn symptoms, and lower mean values for intensity and acid perfusion sensitivity score than in patients with NERD and abnormal pH testing. Additionally, a quarter of functional heartburn patients had a negative acid perfusion test. The latter study further supports the hypothesis that functional heartburn is composed of a heterogeneous group of patients. A significant subset of these patients is unlikely to have GER as the underlying stimulus for their heartburn.
Mechanoreceptor sensitivity to balloon distention seems to be a general phenomenon in functional heartburn, and in a group of patients chemoreceptor sensitivity to acid can also be shown. Regardless, it seems that visceral hyperalgesia is the main underlying mechanism in functional heartburn. Central neural mechanisms such as psychological comorbidity (anxiety, stress, depression) can modulate esophageal perception and cause patients to perceive low intensity esophageal stimuli as being pain (infra vide).35, 44 However, it is still unclear what role these central factors play in symptom generation in patients with functional heartburn.
Frazzoni et al.45 recently evaluated patients with different phenotypic presentations of GERD and compared them with functional heartburn patients and normal controls. Patients with functional heartburn did not differ from normal controls in their distal esophageal acid exposure profile, prevalence of hiatal hernia, distal esophageal amplitude contractions, and LES basal pressure. This study further shows that mechanisms other than reflux are likely to have an important role in symptom generation of those with functional heartburn. Martinez et al.38 demonstrated that patients with NERD and an abnormal pH test were more likely to have an SI >75% compared with functional heartburn patients (6l.9% vs. 10.5%, p = .0001). In the functional heartburn group, those patients with a negative SI reported having heartburn at pH <4 only 12.7% of the time as compared with 70.7% of the time in those with a positive SI, despite a similar mean number of heartburn episodes.25 Consequently, the authors proposed that most (63%) of the patients with functional heartburn appear to have heartburn symptoms unrelated to acid reflux.
The authors also suggested, however, that there was a subgroup of patients that fell under the category of functional heartburn, and demonstrated a close relationship between their heartburn symptoms and acid reflux events. Further support for the existence of this subgroup derives from a therapeutic study in patients with functional heartburn using PPI twice daily.46 In this study, the authors demonstrated that the partial response to PPI therapy seen in patients with functional heartburn is probably owing to the subgroup of patients who have a close correlation between their symptoms and acid reflux events.
The role of bile reflux in symptom generation of NERD patients remains to be elucidated. Nonerosive reflux disease patients and healthy controls appear to have similar level of gastric bile content. Furthermore, in erosive esophagitis and Barrett's esophagus patients, most GER events are a combination of acid and duodenogastroesophageal reflux (79% and 95%, respectively). In contrast, only in half of the NERD patients a combination of acid and duodenogastroesophageal reflux has occurred.47
The main underlying mechanism for heartburn is sensitization of esophageal chemoreceptors either directly by GER or indirectly by inflammatory mediators.32 It has been proposed that this physiologic event is possible owing to the presence of marked dilation of inter-epithelial spaces in the esophageal mucosa of NERD patients, as documented by electron microscopy. A recent study even suggested the presence of dilated inter-epithelial spaces in patients with functional heartburn.48 The presence of dilated inter-epithelial spaces results in an increase in paracellular permeability, allowing acid and other reflux components to reach nerve endings that are located within the esophageal mucosa, leading to a heartburn sensation.49 However, it still remains to be elucidated why most acid reflux events (95%) that occur during a 24-hour pH test are not associated with symptoms. By now, it has been substantiated that acid is not the only stimulus responsible for heartburn sensation, but rather one of a host of different intraesophageal stimuli (nonacidic reflux, a motor event, etc.).
Although we consider any drop of pH below 4 during a pH test to be a reflux event, presently it is unclear that the intraesophageal pH must drop below 4 for symptoms such as heartburn to occur. There is some evidence to suggest that pH changes per se are sufficient to trigger classic heartburn symptoms in a subset of patients.6 This suggests that some patients with normal 24-hour esophageal pH monitoring, who lack any correlation between their symptoms and acid reflux events, may still have symptoms related to reflux that causes pH changes that never reach pH 4.
Perception of GER events appears to be influenced by central and peripheral factors.50 However, it is yet to be determined what factors lead to perception of an intraesophageal event. Meyer et al.51 reported that intraduodenal fat significantly shortened latency to onset of heartburn and intensified the perception of acid-induced heartburn among patients with GERD who underwent intraesophageal acid perfusion.
Psychological comorbidity such as anxiety and depression can modulate esophageal perception and cause patients to perceive low-intensity esophageal stimuli as being painful.35 Stress, through brain–gut interaction, is another important central factor that appears to enhance the perception of intraesophageal acid reflux by reducing perception thresholds for pain as well as alteration in GI secretory and motor responses. Bradley et al.52 suggested that chronically anxious patients when exposed to prolonged stress might perceive low-intensity esophageal stimuli as painful. Baker et al.53 performed psychological assessment of GERD patients and controls. Patients with GERD differed from controls on scales of depression, somatization, anxiety, and intensity of reporting symptom distress. Stress and psychological comorbidity seem to have an important role in symptom generation in GERD patients, particularly in those with NERD. Thus, factors that can modulate brain–gut interaction may alter the perception of intraesophageal pathologic and possibly physiologic events in patients with GERD.6 Potentially, other factors, such as sleep quality, may also alter the perception of intraesophageal stimuli. Further research is needed to better define the brain–gut relationship as it is related to symptom generation in GERD.
Altered pain perception demonstrated by increased chemoreceptor sensitivity to acid has been shown in NERD patients.34, 54 This hypersensitivity to acid can be demonstrated in both the proximal and distal esophagus.55 In contrast, assessment of mechanoreceptor sensitivity using intraesophageal balloon distention has yielded contradictory results. Trimble et al.35 found that patients with heartburn and a normal 24-hour esophageal pH monitoring demonstrated lower perception thresholds for pain as compared with patients with heartburn and excess acid reflux. This study suggests that patients with heartburn who lack any evidence of excess acid are highly sensitive to mechanical stimuli. In another study using esophageal balloon distention delivered by an electronic barostat, patients with NERD or erosive esophagitis (a chronic acid exposure model) did not demonstrate an increase in mechanosensitivity, when compared to normal controls.34 This study suggested that chronic esophageal acid exposure results in chemoreceptor sensitivity but not mechanoreceptor sensitivity.6
Clinical Features
Currently there are no clinical features that can distinguish patients with NERD from those with erosive esophagitis or even those with Barrett's esophagus. Additionally, there are no clinical predictors for patients with functional heartburn, and thus these patients cannot be identified on a clinical basis only. Severity, frequency, or intensity of symptoms has been shown consistently to be similar among the different GERD phenotypes.20, 56 Furthermore, patients with different degrees of esophageal acid exposure have similar symptom presentation. Consequently, the cardinal symptoms of NERD patients are heartburn and acid regurgitation. The word heartburn is commonly used to denote a burning sensation behind the breastbone rising up toward the throat or the neck. Not uncommonly, patients use the word heartburn to describe closely related symptoms (such as dyspepsia or chest pain) and vice versa as well as symptoms that are completely unrelated to GERD. As a result, clarification of the meaning of heartburn is almost always needed, especially when new patients present with this symptom. Heartburn is exacerbated by certain food products, bending over, when assuming the supine position, and during sleep, and it is temporarily relieved by antacids.57
There have been some suggestions in the literature that NERD patients are more commonly reporting associated dyspeptic symptoms than other GERD phenotypes.58 However, symptoms such as bloating, early satiety, nausea, and vomiting are commonly reported by all GERD phenotypes and presently do not appear to afflict any specific group more than the other. In contrast, functional heartburn patients report chest pain significantly more common than their counterparts within the NERD group.59 This may suggest an overlap with other functional esophageal disorders, such as noncardiac chest pain. Other traits of functional bowel disorder have been recently demonstrated in patients with functional heartburn. They include increased reports of somatization and alteration of autonomic activity. Studies have demonstrated that NERD patients experience less nighttime reflux than patients with erosive esophagitis.60 Additionally, patients with erosive esophagitis reported significantly more awakenings during the night owing to heartburn than patients with NERD.61 Heartburn during sleep has been shown to affect patients' perception of their quality of sleep and may be associated with a variety of sleep disturbances.62
Regurgitation may also affect patients with NERD and can present as bitter or sour taste in the mouth. Regurgitation is less common than heartburn and more difficult to control with antireflux treatment. It is exacerbated when bending over or assuming the supine position.
Most patients with atypical manifestations of GERD have NERD. However, when compared to patients with erosive esophagitis, the prevalence of atypical manifestations of GERD are more common in the latter group than in those with NERD.63
As with the other phenotypic presentations of GERD, NERD is a chronic, relapsing disease with periods of exacerbation and remission.20 If treatment is discontinued, 75% of the patients relapse within 6 months.20 As a result most of the patients with NERD require long-term treatment with antireflux medications.
Thus far, we lack any clinical evidence that patients with NERD are at risk of developing any of the typical complications of GERD, Barrett's esophagus, or adenocarcinoma of the esophagus over time. The main impact of the disease is on patients' perception of their quality of life.
Nonerosive reflux disease should be suspected in every patient who presents with typical or extraesophageal manifestations of GERD (Table 1). Specific questions that address different potential manifestations of NERD should be asked. Reports of typical GERD symptoms are indicative of NERD, but these are not always present in patients with atypical manifestations of GERD. Patients reporting heartburn, acid regurgitation, sour or bitter taste in mouth, and water brash (sudden filling of the mouth with salivary secretions in response to acid reflux) should be considered as possibly having NERD. Additionally, NERD may present with cough, wheezing, sore throat, chest pain, and other extraesophageal manifestations. Furthermore, insomnia, dyspeptic symptoms, and other functional bowel symptoms may also be reported by patients with NERD.
A careful physical examination should be performed at the first clinical visit and on subsequent visits as needed. However, most patients with NERD do not demonstrate any specific disease-related physical findings. Additionally, signs that could be found in any GERD patient may be present, such as increased body mass index, obesity, submandibular adenopathy (GERD-related pharyngeal involvement), caries and poor oral hygiene (GERD-related oral involvement), hoarse voice (laryngeal involvement), and wheezing (pulmonary involvement). However, most of these signs are rarely found in patients with NERD.
Diagnosis
Currently, there are no clinical predictive factors that can help us determine if patients harbor erosive esophagitis or Barrett's esophagus or lack esophageal mucosal injury. Regardless, patients presenting with symptoms of GERD (heartburn and acid regurgitation), unless alarm symptoms are present, are likely to be treated empirically with an antireflux medication.64 Reported alarm symptoms such as dysphagia, odynophagia, anorexia, weight loss, GI bleed, and others, require an immediate investigation with an upper endoscopy.
Empirical therapy with a PPI once daily is a reasonable approach for patients with typical GERD symptoms, regardless of whether erosive esophagitis is present or not. Most patients responding to treatment require long-term maintenance therapy.
Upper Endoscopy
In addition to alarm symptoms (dysphagia, odynophagia, anorexia, weight loss, GI bleeding, etc.), upper endoscopy is indicated in patients with long-term GERD symptoms to exclude the presence of Barrett's esophagus.65 However, there is currently no consensus regarding the time threshold for performing this test.
In patients who undergo upper endoscopy off or on antireflux medication, the role of mucosal biopsy to detect histopathologic changes consistent with GERD remains an area of intense controversy. Commonly done in clinical practice, esophageal mucosal biopsy can demonstrate inflammatory cells (neutrophils and eosinophils), epithelial hyperplasia (basal cell hyperplasia and elongated papillae), and dilated vessels in the papillae.65 Funch-Jensen et al.66 found that GERD-related histologic findings are more frequent in NERD patients (47.8%) than normal subjects (21.6%). In contrast, Schindlbeck et al.67 demonstrated that the histologic findings were no different in NERD patients than in controls. Specifically, histologic changes consistent with GERD were found in 46% of NERD patients with abnormal pH testing as compared to only 9% of NERD patients with normal pH test and 29% of healthy controls. The latter study questions the yield of esophageal mucosal biopsies as a diagnostic tool in NERD patients.
A concern has been raised about overdiagnosing NERD during endoscopy, because of the common use of antireflux medications, in many cases over-the-counter products.68 However, one should not make the diagnosis of NERD in patients with normal endoscopy who are actively consuming or recently consumed (within 3 to 4 weeks) histamine-2 receptor antagonists (H2RAs) or PPIs. A subset of patients with healed erosive esophagitis may remain symptomatic and thus should not be considered as having NERD.
Twenty-Four-Hour Esophageal pH Monitoring
The pH test is invasive, inconvenient to patients, and not readily available. It is currently indicated in NERD patients who are candidates for antireflux surgery.69 Studies have demonstrated that NERD patients with abnormal pH test are more likely to respond to antireflux treatment. There is a close correlation between the extent of esophageal acid exposure and response to PPI.26 The greater the acid exposure, the higher the proportion of patients who achieve complete symptom resolution after 4 weeks of treatment with PPI once daily.18 However, mere abnormal esophageal acid exposure is an insufficient clinical predictive factor for response to therapy. Many NERD patients with mildly abnormal pH test (4.2% <% total time <7%) demonstrate a limited response to PPI once daily, almost similar to what has been observed in patients with functional heartburn (normal pH test).
The pH test has also demonstrated some clinical value in distinguishing patients with the hypersensitive esophagus (normal pH test but positive SI) from those with symptoms that are likely to be caused by non–acid-reflux–related stimuli. The former patients appear to respond favorably, albeit in a limited way, to double-dose PPI.70 Some may argue that the symptom association probability (SAP) is more sensitive to determine the association between symptoms and acid reflux events than is the SI. However, most studies in NERD use the latter rather than the former parameter.
Performing 24-hour esophageal pH monitoring for the purpose of subcategorizing NERD patients is not practical in clinical practice. However, given the fact that the PPI empirical trial is as sensitive as the pH test in identifying GERD patients, the former is commonly practiced by primary care physicians and gastroenterologists alike.71 Lack of response of a NERD patient to PPI twice daily is suggestive of non–acid-reflux–related stimuli that are unlikely to improve with escalating PPI doses.
Proton Pump Inhibitor Test
The PPI therapeutic trial (or PPI test), which entails using a high-dose PPI over a short period of time, has shown it to be an accurate and cost-effective diagnostic strategy in patients with GERD.23, 72 Patients with NERD demonstrated marked improvement in symptom response rate, from 27.2% to 83.3%, when the omeprazole test dose (given over 7 days) was increased from 40 mg once daily to 40 mg twice daily.73 Schenk et al.23 evaluated 85 NERD patients with the PPI test (omeprazole 40 mg daily) administered over a period of 14 days and demonstrated a 66% sensitivity in this group of patients. The PPI test consistently had a low specificity in GERD patients, specifically in NERD patients. The potential explanation for this phenomenon is the partial response to therapy of patients with functional heartburn, particularly those with a "sensitive esophagus."
Treatment
The goals of treatment in NERD should include acute and long-term relief of symptoms, prevention of symptom relapse, and improvement in quality of life. In general, therapeutic requirements for patients with NERD are similar to those for patients with erosive esophagitis. Proton pump inhibitors are the most efficacious therapeutic modality in NERD patients.
Overall, complete symptom control is achievable in only 37.6% (PPI symptomatic response pooled rate) of NERD patients as compared with 55% (PPI symptomatic response pooled rate) of those with erosive esophagitis after 4 weeks of treatment with a standard dose PPI74 (Figure 4). The lower response rate to PPI therapy as observed in NERD patients is attributed to the heterogeneity of this group. Specifically, the functional heartburn patients demonstrate the lowest response rate to PPI once daily of all NERD patients.
Figure 4: The effectiveness of proton pump inhibitor therapy in NERD as compared to erosive esophagitis (EE).
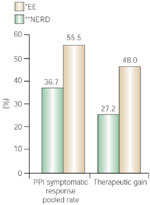
(Source: Adapted from Dean et al.74)
Unfortunately, NERD patients are still considered as having just a mild form of GERD, a position still widely held by institutions and third-party payers. Consequently, prescribing a PPI is commonly discouraged, and many of the patients are treated with long-term H2-blockers. However, therapeutic studies with H2-blockers in NERD patients showed very limited response rate, not greater from what was expected from placebo.56 Generally H2-blockers are ineffective in inhibiting meal-induced acid secretion and are associated with development of rapid tolerance.75 Increased doses in nonresponders are associated with very modest therapeutic gain. The role of prokinetics in NERD was assessed in a large European study. Remission of symptoms was achieved in few than half of the patients who were receiving cisapride.76 As with H2-blockers, the therapeutic efficacy of prokinetics in NERD patients appears to be very limited. This is compounded by the fact that cisapride is available only through a compassionate usage program.
In a 4-week duration study, omeprazole 20 mg once daily resulted in complete symptom relief in 61% of NERD patients.56 In a placebo-controlled trial, resolution of heartburn at 4 weeks was achieved in 61% of the patients receiving omeprazole 20 mg once daily versus 24% of those receiving placebo.18 In this study, the proportion of patients reporting complete symptom resolution was correlated with the prerandomization distal esophageal acid exposure as determined by pH testing (the greater the acid exposure, the higher the number of patients responding to PPI once daily). The NERD patients with normal pH test (functional heartburn) demonstrated the lowest response rate to PPI once a day. Therapeutic studies in NERD patients that compared the efficacy of PPIs versus H2-blockers and cisapride clearly demonstrated the superiority of PPIs. Patients who received standard-dose PPI once daily achieved 60% remission rate and more than 50% were maintained symptom free as compared to 40% and less than 30%, respectively, of those who received ranitidine 150 mg twice daily.19, 77, 78
The role of antireflux surgery in patients with NERD has scarcely been evaluated. Nissen fundoplication has been shown to reduce the frequency of TLESR, the main underlying mechanism for GER in NERD. However, patients with NERD and abnormal pH test had a lower symptom improvement rate, a higher level of dissatisfaction, as well as more reports of postoperative dysphagia than erosive esophagitis patients.79 A positive predictive factor for favorable outcome was a positive preoperative response to PPI therapy. In another study, results of Nissen fundoplication in NERD patients with normal preoperative pH test were compared with NERD patients and abnormal pH test.80 The authors demonstrated that those with normal pH test have significantly worse subjective outcomes after Nissen fundoplication compared with patients having abnormal preoperative pH test results.
Because most natural history studies suggest that the vast majority of NERD patients never progress to develop erosive esophagitis or Barrett's esophagus,81 therapeutic approaches such as on-demand or intermittent therapy are an attractive option for these patients. These therapeutic strategies are further supported by the notion that many patients commonly use PPIs only when symptoms relapse and not on a regular basis.82 Randomized controlled trials that assessed the clinical value of intermittent and on-demand therapies in NERD patients have demonstrated that these therapeutic strategies are adequate for long-term control of GERD symptoms and improvement of quality of life. Furthermore, on-demand and intermittent therapy were also found to be safe and the most cost-effective therapeutic strategy for GERD.26, 83, 84, 85 Over time (6 months), about 20% of NERD patients no longer respond to intermittent or on-demand therapy, primarily owing to symptoms relapse or worsening in symptoms severity.
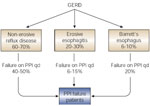
In recent years, PPI failure (continuation of GERD symptoms while on standard-dose PPI) has become a major clinical dilemma in GI practice. Based on their overall low symptoms response rate, it is highly likely that most of the patients who failed PPI used once daily originate from the NERD group. Furthermore, the main contributors to the PPI failure group are patients with functional heartburn, who demonstrate the lowest symptom response rate to PPI used once a day among NERD patients (Figure 5).
Adding a pain modulator in PPI-failure NERD patients is an attractive therapeutic strategy, because of the notion that many patients who fail PPI are likely to have functional heartburn. Pain modulators, such as tricyclics and selective serotonin reuptake inhibitors (SSRIs), have been shown to be highly efficacious in patients with noncardiac chest pain of presumed esophageal origin.86, 87, 88 These visceral analgesics are used in non–mood-altering low doses, to relieve esophageal pain. Currently, there are no studies to demonstrate their value in PPI failure patients, but they may provide a therapeutic alternative until more novel and GI-specific pain modulators are available. Adding a pain modulator to a PPI or just providing a pain modulator alone to those without any improvement on a PPI is a therapeutic strategy that can be entertained in NERD patients who failed PPI.
Future Developments
Future developments in the field will focus on determining the underlying mechanisms for symptom generation in patients with NERD. Identification of the pain receptors and the mapping of their distribution along the esophagus will be a primary investigative target. The role of weakly acidic reflux in generating symptoms in NERD patients will be evaluated by tools such as the multichannel impedance with a pH sensor. The genetic makeup of patients with NERD will provide clues to the natural history of the disease. Additional attempts to detect minimal mucosal changes in patients with NERD, using improved endoscopic techniques, will be carried out, but unlikely to be clinically helpful owing to low inter- and intraobserver variability.
More studies will be carried out to characterize the functional heartburn patients in the hope of identifying them clinically. Because NERD is perceived as an area with unmet needs, it will become a major target for new therapeutic approaches and novel antireflux medications. However, medications that can alter esophageal pain are likely to revolutionize the current treatment for NERD.
Conclusion
Nonerosive reflux disease is the most common presentation of GERD in community-based patients. Many patients with NERD have moderate-to-severe symptoms and significant impairment in quality of life. Therapy with a PPI results in improvement or complete resolution of symptoms in most NERD patients and restores quality of life. However, the symptom response rate of NERD patients to standard-dose PPI is significantly lower than what has been reported for patients with erosive esophagitis. The role of antireflux surgery in NERD patients needs to be further defined. Alternative therapeutic strategies with a PPI, such as on-demand or intermittent, are adequate for treating most NERD patients owing to the low risk of progression over time to erosive esophagitis or Barrett's esophagus.
