
Abstract
Study Design:
Case series.
Objective:
To compare transcranial magnetic stimulation (TMS) and magnetic resonance imaging (MRI) findings between patients who underwent surgery for cervical spondylotic myelopathy and those with spondylosis who were not operated upon, and to correlate these findings with clinical functionality at follow-up.
Setting:
Private practice.
Methods:
Of 16 consecutive patients with cervical spondylosis 8 underwent surgery (group I) and 8 were treated conservatively (group II). We compared TMS and MRI findings between these groups and we correlated central motor conduction times (CMCTs) and MRI-measured sagittal and parasagittal diameters of the spinal canal at baseline evaluation, with clinical functionality at 2-year follow-up.
Results:
Group I CMCTs at the lower limbs correlated significantly with modified-JoA 2 years post surgery (r=−0.71, P<0.05), but MRI-measured diameters did not. In group II baseline TMS was unrevealing, contrary to significant spinal stenosis disclosed by MRI. The condition of none of these patients deteriorated at 2 years.
Conclusions:
CMCTs at the lower limbs, but not cervical spinal canal diameters, correlate with long-term functional outcome following surgical or conservative treatment.
Similar content being viewed by others


Introduction
Whether magnetic resonance imaging (MRI) and transcranial magnetic stimulation (TMS) can predict long-term clinical outcomes in patients with cervical spondylosis is an issue of debate.1, 2, 3 We compared TMS and MRI findings between a group of patients who underwent surgery for cervical spondylotic myelopathy and a second group with spondylosis, who were not operated upon, and we correlated these abnormalities with longitudinal clinical follow-up.
Materials and methods
We evaluated by TMS and MRI, in the context of our routine assessment protocol, 16 consecutive patients who presented with symptoms of (a) cervical myelopathy, (b) upper-limb radicular lesions or (c) pain localized at the cervix. TMS evaluation comprised determination of the central motor conduction times (CMCTs) at the upper and lower limbs, according to the f-wave method.4 Motor Evoked Potentials were recorded from the abductors digiti minimi (ADM) and extensors digitorum brevis (EDB).
MRI evaluation comprised determination of the transverse diameter of the spinal canal at the midline (dmri_midline) and at 50% of the distance between the midline and the left (dmri_left) and right (dmri_right) borders of the spinal canal, at all intervertebral levels. We also looked for T2 signal hyperintensities and we screened patients by EMG for radicular lesions.
Surgery was recommended to patients who had (1) clinical and/or TMS signs of myelopathy and (2) weakness or intolerable pain of radicular origin, or signs of acute denervation in the EMG. Patients with pain but without weakness or denervation in the EMG and with unrevealing TMS were treated conservatively. All patients were followed up for at least 2 years. Clinical functionality was expressed in terms of the modified Japanese Orthopedic Association (modified-JoA) scale, at baseline evaluation and at 2 years.
We correlated CMCTs at the upper and lower limbs with MRI-based measures and with the modified-JoA scale at baseline and at 2 years of follow-up. For each patient, we included one upper-limb and one lower-limb CMCT value (right or left) in the analysis, recorded from the most severely affected side, denoted as CMCTmostaffected_adm and CMCTmostaffected_edb.
On the MRI we analyzed dmri_midline, dmri_left and dmri_right measured at the level shown to suffer the most severe stenosis. We denote the smallest of dmri_left, dmri_right as dmri_smallest_parasagittal and the parasagittal diameter ipsilateral to CMCTmostaffected_adm or CMCTmostaffected_edb as dmri_ipsilateral_adm and dmri_ipsilateral_edb, respectively. We included in the statistical analysis the following MRI-based measures: (1) we correlated CMCTs on the most affected side (CMCTmostaffected_adm and CMCTmostaffected_edb) with the ipsilateral parasagittal diameter (dmri_ipsilateral_adm and dmri_ipsilateral_edb) and with the midline diameter of the spinal canal (dmri_midline); (2) we also correlated the smallest parasagittal diameter (dmri_smallest_parasagittal) with CMCTmostaffected_adm and CMCTmostaffected_edb. Our aim was to determine whether any of the spinal canal diameters shows a significant correlation with CMCTs. Finally (3) we correlated spinal canal diameters (dmri_smallest_parasagittal and dmri_midline) with the modified-JoA scale at baseline and at 2 years of follow-up.
We also compared our neurophysiology and imaging findings between patients who underwent surgical decompression and those who were treated by conservative measures. With regard to TMS, we compared between the groups CMCTmostaffected_adm and CMCTmostaffected_edb, whereas for MRI we compared dmri_smallest_parasagittal and dmri_midline. Here we wanted to test whether the two groups were significantly different in terms of their most severe findings on the MRI and TMS evaluations.
For correlation, we used Pearson’s (r). We tested for differences between groups using the two-sided Student’s t-test. All calculations were performed in Microsoft Excel 2008.
Results
Of the 16 patients, 8 underwent surgical decompression (group I), whereas 8 were treated by conservative measures (group II). Table 1 outlines patient demographic characteristics and clinical presentation.
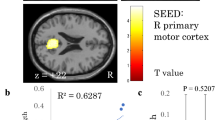
In group I, baseline CMCTmostaffected_edb correlated significantly with modified-JoA 2 years after surgery (r=−0.71, P<0.05). None of the remaining correlations were statistically significant (Table 2). Table 3 compares the mean values of TMS and MRI parameters between group I and group II.
In group II, myelopathic symptoms were absent; thus, modified-JoA was not used. However, clinical functionality had not deteriorated in any of these patients at 2-year follow-up. In this group baseline TMS was unrevealing, contrary to the MRI, which in many cases disclosed signficant stenosis (dmri_midline<10 mm).
Finally, there were no signal hyperintensities or EMG signs of denervation in any of the patients. All group I patients underwent anterior cervical discectomy and fusion.
Discussion
Whether TMS can determine prognosis after surgical decompression in patients with cervical spondylotic myelopathy is an issue of debate.3 We found that pre-surgical CMCT at the lower limbs can predict functional recovery. Thus, our work further supports this view5 and refutes studies with opposite findings.6, 7
In conservatively treated patients, normal CMCTs at baseline were in agreement with their sustained clinical functionality at 2-year follow-up, despite the significant stenosis seen in many of the MRIs. The average midline diameter of the spinal canal in this group was 9.2 mm—that is, below 10 mm, the widely accepted limit for surgical intervention.8
Although none of the MRI measures correlated with postsurgical outcome, the smallest parasagittal diameter of the spinal canal, dmri_smallest_parasagittal, was significantly smaller in surgically treated patients compared with conservatively treated ones, whereas the midline diameter was not significantly different. This finding speaks against the use of the midline diameter alone when making a decision for surgery; as many disc hernias project more laterally than centrally, evaluation of the parasagittal diameters is also important.
Our findings suggest that, in addition to the clinical picture, TMS can be an important tool when making the decision to treat cervical spondylosis surgically and has the potential to predict the long-term postoperative outcome. Although the number of patients included in this series is small, our work supports the reappraisal of the value of TMS in this context in further studies with a larger sample size.
References
Karpova A, Arun R, Cadotte DW, Davis AM, Kulkarni AV, O’Higgins M et al. Assessment of spinal cord compression by magnetic resonance imaging—can it predict surgical outcomes in degenerative compressive myelopathy? A systematic review. Spine 2013; 38: 1409–1421.
Wilson JR, Barry S, Fischer DJ, Skelly AC, Arnold PM, Riew KD et al. Frequency, timing, and predictors of neurological dysfunction in the nonmyelopathic patient with cervical spinal cord compression, canal stenosis, and/or ossification of the posterior longitudinal ligament. Spine 2013; 38: S37–S54.
Holly LT, Matz PG, Anderson PA, Groff MW, Heary RF, Kaiser MG et al. Clinical prognostic indicators of surgical outcome in cervical spondylotic myelopathy. J Neurosurg Spine 2009; 11: 112–118.
Hallett M, Chokroverty S. (eds) Magnetic Stimulation in Clinical Neurophysiology, 2nd edn. Butterworth-Heinemann: Philadelphia, PA, USA. 2005, pp 106–120.
Takahashi J, Hirabayashi H, Hashidate H, Ogihara N, Yamazaki I, Kamimura M et al. Assessment of cervical myelopathy using transcranial magnetic stimulation and prediction of prognosis after laminoplasty. Spine 2008; 33: E15–E20.
Jaskolski DJ, Laing RJ, Jarratt JA, Jukubowski J . Pre- and postoperative motor conduction times, measured using magnetic stimulation, in patients with cervical spondylosis. Br J Neurosurg 1990; 4: 187–192.
De Mattei M, Paschero B, Cocito D, Cassano D, Campanella A, Rizzo L et al. Motor evoked potentials in the post-surgical follow-up of cervical spondylotic myelopathy. Ital J Neurol Sci 1995; 16: 239–248.
Bess S . Tandem stenosis: fix the cervical or lumbar spine first? In: The Cervical Spine, 5th edn. Lippincott Williams & Wilkins: Phladelphia, PA, USA. 2012, pp 1498–1506.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Deftereos, S., Kechagias, E., Ioakeimidou, C. et al. Transcranial magnetic stimulation but not MRI predicts long-term clinical status in cervical spondylosis: a case series. Spinal Cord 53 (Suppl 1), S16–S18 (2015). https://doi.org/10.1038/sc.2014.220
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sc.2014.220
This article is cited by
-
Abnormal central motor conduction at the upper but not lower limbs correlates with severe cervical spondylosis: discussion of an unexpected observation
Spinal Cord Series and Cases (2017)
-
The contribution of neurophysiology in the diagnosis and management of cervical spondylotic myelopathy: a review
Spinal Cord (2016)
