
Abstract
There is limited research on the association between the alanine aminotransferase to high-density lipoprotein cholesterol ratio (ALT/HDL-C) ratio and nonalcoholic fatty liver disease (NAFLD). The purpose of the current research was to look into the connection between the ALT/HDL-C ratio and the risk of NAFLD in lean Chinese individuals. Between January 2010 and December 2014, 11,975 non-obese people participated in this prospective cohort research. The relationship between the ALT/HDL-C ratio and the risk of developing NAFLD was assessed using the Cox proportional-hazards regression model, Cox proportional hazards regression with cubic spline functions and smooth curve fitting, sensitivity analysis, and subgroup analyses. The ALT/HDL-C ratio’s potential value as a NAFLD prognostic marker was to be evaluated using the receiver operating characteristic curve analysis. A total of 5419 (45.253%) women comprised the research's participant population, and the research participants’ average age was 43.278 ± 14.941 years. The ALT/HDL-C ratio was 11.607 (7.973–17.422) at the median (interquartile ranges). 2087 (17.428%) patients had NAFLD diagnoses throughout a median follow-up of 24.967 months. The study's findings demonstrated a positive connection between the ALT/AHDL-C ratio and the incident NAFLD (HR = 1.037, 95% CI: 1.031–1.042) when adjusting for relevant factors. The ALT/HDL-C ratio and NAFLD risk had a nonlinear connection, with 12.963 as the ratio's inflection point. Effect sizes (HR) were 1.023 (95% CI: 1.017–1.029) and 1.204 (95% CI: 1.171–1.237), respectively, on the right and left sides of the inflection point. The sensitivity analysis also showed how reliable our findings were. According to subgroup analysis, those with BMI < 24 kg/m2 and DBP < 90 mmHg had a stronger correlation between the ALT/HDL-C ratio and NAFLD risk. The current study shows a positive and non-linear connection between the ALT/HDL-C ratio and NAFLD risk in lean Chinese individuals. When the ALT/HDL-C ratio is less than 12.963, it is significantly linked to NAFLD. Therefore, from a therapy standpoint, it is advised to keep the ALT/HDL-C ratio less than the inflection point.
Similar content being viewed by others


Introduction
The world’s most common chronic liver disease is a non-alcoholic fatty liver disease (NAFLD), characterized by fat buildup inside hepatocytes (hepatic steatosis). Hepatocellular carcinoma incidence strongly correlates with its clinical symptoms, including hepatic steatosis, steatohepatitis, fibrosis, and cirrhosis1,2,3. Although NAFLD has also frequently been seen in obese people4, the percentage of NAFLD in lean or non-obese patients is increasing5,6,7. Within the United States, the prevalence of NAFLD is estimated at 23%8, with up to 7–20% of lean individuals suffering from hepatic steatosis9,10. Hepatic steatosis has been found in 8–19% of lean people in Asian populations11. Additionally, patients who are lean and have NAFLD are more prone to develop metabolic syndrome and other severe conditions, such as type 2 diabetes mellitus (T2DM), severe cardiovascular disease, and liver disease12,13,14,15. Furthermore, numerous investigations have established a link between low-density lipoprotein cholesterol (LDL-C) and NAFLD16,17. Concurrently, recent research indicated that even LDL-C levels considered within the normal range could significantly impact NAFLD's occurrence and widespread nature18. Therefore, it can still be important to identify lean individuals with a normal range of LDL-C who are at risk for NAFLD.
Alanine aminotransferase (ALT), a commonly used marker to assess hepatocyte damage, is a well-established indicator of non-alcoholic fatty liver disease (NAFLD). It has a strong connection to the prevalence of NAFLD19,20. Elevated ALT levels are also linked to NAFLD with a more severe histological spectrum, including fibrosis and non-alcoholic steatohepatitis (NASH), according to research21,22. Conversely, decreased levels of high-density lipoprotein cholesterol (HDL-C) are a risk factor for the development of metabolic syndrome23,24. NAFLD and the components of metabolic syndrome are connected. It has been proposed that NAFLD is sometimes viewed as the metabolic syndrome's hepatic manifestation25. According to several recent research, the risk of T2DM and NAFLD was correlated with HDL-C and ALT levels20,26. Recent cohort research also found a positive correlation between higher alanine aminotransferase to high-density lipoprotein cholesterol (ALT/HDL-C) ratio levels and T2DM27. However, there was no proof that the ALT/HDL-C ratio increased the incident NFLAD. We conducted cohort research to explore this theory and learn how the ALT/HDL-C ratio affects incident NAFLD in lean Chinese individuals with a normal range of LDL-C.
Methods
Data source
From January 2010 to December 2014, participants at Wenzhou Medical Center, Wenzhou People's Hospital, China, were enrolled in this retrospective cohort study28. DATADRYAD database made the initial data provided by Sun et al.28 accessible for free download.
Study participants
In order to minimize selection bias, the individuals were obtained consecutively from Wenzhou People’s Hospital in China. Their identity information was encoded into an untraceable code to maintain the participants’ anonymity. Every procedure involving patients at Wenzhou People's Hospital was approved by the clinical research ethics committee in line with the Helsinki Declaration28. In addition, this study has been approved by the Ethics Committee of the Shenzhen Dapeng New District Nan’ao People’s Hospital (2022082201).
Between January 2010 and December 2014, 33,153 Chinese people without NAFLD in the original research who underwent a health evaluation met the inclusion criteria for the initial investigation28. 21,178 subjects were eliminated, leaving 11,975 subjects for data analysis in the current research. There were some exclusion standards: (1) LDL-C > 3.12 mmol/L; (2) body mass index (BMI) ≥ 25 kg/m2; (3) taking lipid-lowering, anti-diabetic agents or anti-hypertensive; (4) excessive drinking (not less than 140 g per week for men or 70 g per week for women); (5) known chronic liver diseases, such as autoimmune hepatitis, NAFLD, or viral hepatitis; (6) missing data or lost to follow-up. In addition, individuals with missing ALT values (n = 4045) and individuals with abnormal ALT/HDL-C ratio values (three standard deviations above or below the mean) (n = 153) were not included in the current investigation (Fig. 1).

Study population.
ALT/HDL-C ratio
HDL-C and ALT levels were assessed in fasting blood samples using the Abbott AxSYM automatic biochemical analyzer. The Abbott Abbott AxSYM automatic biochemical analyzer used an enzymatic assay to measure ALT levels and a direct selective immunoinhibition assay to measure HDL-C. Then, by dividing ALT by HDL-C, we created a new variable that served as the foundation for our study.
Diagnosis of incident NAFLD
According to the Chinese Liver Disease Association's recommendations29, the existence of NAFLD was determined by ultrasonography based on the following criteria: (1) diffusely boosted near-field echoes and progressively attenuated far-field echoes in the liver region; (2) unclear display of intrahepatic structure; (3) enlarged liver with a round and blunt border; (4) Weakened hepatic blood flow signal; (5) right liver lobe and diaphragm being unclear or incomplete.
Covariates
The factors for this investigation were selected considering prior research and our clinical expertise. Personal information, such as weight, gender, height, and age, was collected based on a standardized spreadsheet. The subjects were seated in a peaceful area, and their diastolic blood pressure (DBP) and systolic pressure (SBP) were measured using an automated blood pressure monitor. BMI was computed as the weight (kg) ratio and the square of height (m2). The following laboratory parameters were measured in venous blood after an overnight fast: triglyceride (TG), creatinine (Cr), γ-glutamyl transpeptidase (GGT), LDL-C, aspartate aminotransferase (AST), uric acid (UA), fasting plasma glucose (FPG), total cholesterol (TC), and alkaline phosphatase (ALP).
Missing data processing
There were 15 (0.125%), 15 (0.125%), and 2 (0.017%) subjects with missing data for SBP, DBP, and GGT, respectively. The missing data were handled by applying multiple imputations. Age, gender, AST, BMI, ALP, SBP, GGT, TC, DBP, UA, TG, Cr, FPG, and LDL-C were all added to the imputation model. Missing-at-random assumptions were employed in missing data analysis processes30,31.
Statistical analysis
Statistical analysis was employed using Empower Stats (version 4.1) and R software version 3.4.3.
Using the quartiles of the ALT/HDL-C, the current research separated the subjects into four groups. The median (interquartile ranges) or mean ± standard deviation (SD) were shown for continuous data, while frequencies and percentages were shown for categorical data. The present research utilized χ2 (categorical data), the Kruskal–Wallis H test (skewed distribution), and the one-way ANOVA test (normal distribution) to examine differences between ALT/HDL-C ratio groups.
The current research utilized univariate and multivariate Cox proportional-hazards regression models to test the correlation between ALT/HDL-C ratio and NAFLD, including Model 1 (no adjustment for covariates), Model 2 (adjusted DBP, gender, age, SBP, and BMI) and Model 3 (adjusted AST, ALP, GGT, UA, Cr, FPG, TG, TC, LDL-C plus the same parameters as model 2). The models generated effect sizes (HR) and 95% confidence intervals (CI), which were adjusted for covariates that resulted in a 10% or greater change in HR32. Moreover, no covariates were excluded from the Cox proportional-hazards regression models according to the screening results for collinearity.
The current research carried out several sensitivity analyses to evaluate the robustness of our findings. In order to scrutinize the findings of the ALT/HDL-C ratio as a continuous variable and investigate the likelihood of non-linearity, the current research ascertained the P-value for the trend by categorizing the ALT/HDL-C ratio into quartiles. TG33 and obesity4 are strongly linked to NAFLD. We thus excluded patients with TG ≥ 1.7 mmol/L and BMI ≥ 24 kg/m2 from further sensitivity analyses looking at the correlation between the ALT/HDL-C ratio and NAFLD risk. Additionally, the current research utilized a generalized additive model (GAM) to further integrate the continuous covariate as a curve in the equation to validate the findings (model 4).
To accommodate the non-linear correlation between the ALT/HDL-C ratio and NAFLD, the current research employed a Cox proportional hazards regression model with cubic spline functions and smooth curve fitting34. The two-piecewise Cox proportional-hazards regression model was utilized to shed light on the inflection point and threshold effect of the ALT/HDL-C ratio and NAFLD.
The current research used a stratified Cox proportional-hazards regression model to analyze multiple subgroups (DBP, gender, age, SBP, and BMI). First, according to the clinical cutpoints, continuous variables for age (< 60, ≥ 60 years), DBP (< 90, ≥ 90 mmHg), BMI (< 24, ≥ 24 kg/m2), and SBP (< 140, ≥ 140 mmHg) were transformed into categorical variables. Second, we adjusted each stratification for all variables (DBP, gender, age, SBP, BMI, TC, AST, UA, GGT, TG, ALP, Cr, FPG, LDL-C) except the stratification factor itself. The likelihood ratio test was utilized in models with and without interaction terms to determine the presence of such terms35.
The Receiver Operating Characteristic (ROC) curve was employed to evaluate the predictive capacity of HDL-C, ALT, and ALT/HDL-C ratio in relation to NAFLD risk. The STROBE criteria were followed while writing up all of the results. Two-tailed test to determine statistical significance at P less than 0.05.
Ethics approval and consent to participate
The study was conducted following the Declaration of Helsinki and was approved by the Clinical Research Ethics Committee in Wenzhou People’s Hospital. Informed consent was obtained from all subjects and/or their legal guardian(s). In addition, the study has also been approved by the Ethics Committee of the Shenzhen Dapeng New District Nan'ao People's Hospital (2022082201).
Results
Characteristics of subjects
In the present study, 11,975 subjects deemed free of NAFLD at baseline were included. The mean age of the current research was 43.278 ± 14.941 years, with 5419 (45.253%) of the subjects being female. The average age was 43.278 ± 14.941 years, and 5419 (45.253%) were female. 2087 (17.428%) patients had NAFLD diagnoses throughout a median follow-up of 24.967 months. Table 1 provides the fundamental indicators, laboratory tests, and other factors of participants included in the study. Using the quartiles of the ALT/HDL-C ratio (Q1 ≤ 7.971; 7.971 < Q2 ≤ 11.602; 11.602 < Q3 ≤ 17.419; Q4 > 17.419). The other three groups had higher ALP, DBP, ALT, FPG, Cr, BMI, GGT, UA, TG, AST, SBP, and lower HDL-C, TC compared to the Q1 group (ALT/HDL-C ratio ≤ 7.971). Additionally, the Q4 group (ALT/HDL-C ratio > 17.419) had a larger percentage of men.
The incidence rate of NAFLD
2087 (17.428%) patients had NAFLD diagnoses throughout a median follow-up of 24.967 months. All persons’ cumulative incidence rate and each ALT/HDL-C ratio group’s cumulative incidence rate were 7.128, 1.659, 3.932, 8.187, and 14.734 per 100 person-years, respectively (Table 2). All persons’ incidence rates and each ALT/HDL-C ratio group’s incidence rate were 17.428% (16.748–18.108%), 4.008% (3.305–4.711%), 9.659% (8.600–10.718%), 20.334% (18.892–21.776%), and 35.705% (33.988–37.422%), respectively (Table 2). In contrast to the group with the lowest ALT/HDL-C ratio, participants with greater ALT/HDL-C ratios showed higher incidence rates of NAFLD (P < 0.001 for trend).
Figure 2 displays the Kaplan–Meier survival curves for NAFLD-free survival probability divided by the ALT/HDL-C ratio group. The groups with different ALT/HDL-C ratios had significantly different chances of NAFLD-free survival (log-rank test, P < 0.001). This current study indicated that the Q4 group (ALT/HDL-C ratio > 17.419) had the highest risk of developing NAFLD, and the chance of NAFLD-free survival g steadily decreased as the ALT/HDL-C ratio increased.

Kaplan–Meier event-free survival curve. Kaplan–Meier event-free survival curve. Kaplan–Meier analysis of incident NAFLD based on the ALT/HDL-C ratio quartiles (log-rank, P < 0.001).
The correlation between ALT/HDL-C ratio and NAFLD
The relevant data were undergoing a univariate analysis, which revealed that DBP, age, SBP, BMI, TC, AST, UA, GGT, TG, ALP, Cr, FPG, LDL-C, and ALT/HDL-C ratio were positively correlated with NAFLD in Table 3.
The ALT/HDL-C ratio and NAFLD risk were shown to be related by employing the multivariate Cox proportional-hazards regression model (Table 4). A 5.2% increase in the risk of NAFLD was connected to a rise of 1 unit in the ALT/HDL-C ratio in Model 1 (HR = 1.052, 95% CI: 1.048–1.055, P < 0.001). When we solely made demographic adjustments (DBP, gender, age, SBP, and BMI) in Model 2, the risk of NAFLD rose by 3.4% for every extra unit of ALT/HDL-C ratio (HR = 1.034, 95% CI: 1.030–1.038, P < 0.001). In Model 3, the incident NAFLD increased by 3.7% for every extra unit of the ALT/HDL-C ratio when adjusting for relevant factors (DBP, gender, age, SBP, BMI, TC, AST, UA, GGT, TG, ALP, Cr, FPG, and LDL-C) (HR = 1.037, 95% CI: 1.031–1.042, P < 0.001). Additionally, the Q4 group (ALT/HDL-C ratio > 17.419) was related to an elevated risk for NAFLD when we used the lowest quartile as a reference (Model 1, Q4: HR = 8.440, 95% CI: 6.987, 10.195, P < 0.001) (Model 2, Q4: HR = 4.469, 95% CI: 3.688–5.416, P < 0.001) (Model 3, Q4: HR = 4.417, 95% CI: 3.575–5.457, P < 0.001) (Table 4).
Sensitive analysis
The continuity covariate was added into the equation as a curve in the current research employing a GAM in Model 4 (HR = 1.028, 95% CI: 1.022–1.034, P < 0.001) (Table 4). The ALT/HDL-C ratio remained strongly linked with NAFLD even after the present investigation excluded patients with BMI ≥ 24 kg/m2 and TG > 1.7 mmol/L for sensitivity analysis in Table 5. The outcomes of each sensitivity analysis demonstrated the robustness of the association between the ALT/HDL-C ratio and the NAFLD.
The nonlinear correlation between the ALT/HDL-C ratio and NAFLD risk
The correlation between the ALT/HDL-C ratio and NAFLD was investigated employing the Cox proportional hazards regression model with cubic spline functions in Fig. 3. After controlling for DBP, gender, age, SBP, BMI, TC, AST, UA, GGT, TG, ALP, Cr, FPG, and LDL-C, a non-linear connection between the ALT/HDL-C ratio and NAFLD was revealed in Table 6 (log-likelihood ratio test P < 0.001). We first used a recursive method to identify the ALT/HDL-C ratio’s inflection point (12.963). Subsequently, a two-piecewise Cox proportional-hazards regression model was utilized to estimate the HR and 95% CI on either side of the inflection point. On the left side of the inflection point, the HR was 1.204 (95% CI: 1.171–1.237). On the right side of the inflection point, the HR was 1.023 (95% CI: 1.017–1.029).

The nonlinear relationship between the ALT/HDL-C ratio and incident NAFLD. A nonlinear relationship was detected after adjusting for DBP, gender, age, SBP, BMI, TC, AST, UA, GGT, TG, ALP, Cr, FPG, and LDL-C.
The results of the subgroup analysis
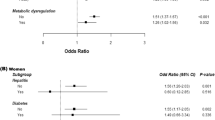
There was no significant interaction between age, gender, and SBP in any predetermined or exploratory subgroups assessed (Table 7). Conversely, valuable interactions in BMI and DBP were found. More specifically, those with DBP < 90 mmHg (HR = 1.040, 95% CI: 1.034–1.045, P < 0.001) and BMI < 24 kg/m2 (HR = 1.057, 95% CI: 1.051–1.064, P < 0.001) had higher correlations between the ALT/HDL-C ratio and NAFLD. In comparison, individuals with DBP ≥ 90 mmHg (HR = 1.026, 95% CI: 1.015–1.037, P < 0.001) and BMI ≥ 24 kg/m2 (HR = 1.030, 95% CI: 1.021–1.039, P < 0.001) had lesser associations.
NAFLD prediction using the ALT/HDL-C ratio
The predictive capacity of HDL-C, ALT, and ALT/HDL-C ratio in relation to NAFLD risk was further evaluated using a ROC curve (Fig. 4). Areas under the curves are listed for each variable in the following table in Fig. 4: HDL-C: 0.671; ALT: 0.712; ALT/HDL-C ratio: 0.744. The best cut-off value was 1.365, 16.500, and 12.385, respectively, based on the Youden index of the ALT/HDL-C ratio, ALT, and HDL-C of 0.375, 0.320, and 0.271 (Table 8). The ALT/HDL-C ratio’s capacity to predict NAFLD risk was better than that of other variables, as evidenced by the fact that its Youden index and AUC were the biggest in Table 8.

The ALT/HDL-C ratio for predicting NAFLD in all participants by ROC analyses.
Discussion
This retrospective investigation found that in lean Chinese individuals, a heightened ALT/HDL-C ratio was found to be associated with an increased risk of NAFLD. The inflection point of the nonlinear association between the ALT/HDL-C ratio and NAFLD was 12.963. Our findings revealed a statistically significant positive correlation between the ALT/HDL-C ratio level and NAFLD when it was 12.963 (HR = 1.204, 95% CI: 1.171–1.237). It was also discovered that BMI and DBP might change the link to the ALT/HDL-C ratio and NAFLD. In the population with DBP < 90 mmHg and BMI < 24 kg/m2, greatly stronger relationships were detected. According to the research mentioned above, the ALT/HDL-C ratio might serve as a benchmark for the main prevention of NAFLD in lean Chinese individuals ith a normal range of LDL-C.
A recent historical Japanese cohort study including 15,342 participants showed a positive correlation between elevated ALT/HDL-C ratio levels and T2DM (HR: 1.01, 95% CI: 1.00–1.02, P = 0.049)27. Based on a comprehensive literature search, it was determined that no current studies have examined the correlation between the ALT/HDL-C ratio and NAFLD risk. However, recent research has indicated a positive correlation between ALT levels and incident NAFLD20,36 and a negative correlation between HDL-C and the occurrence of NAFLD. In addition, a cross-sectional study that included 3311 participants found that ALT levels were an independent risk factor for NAFLD, even within the normal ALT range (OR = 4.98, 95% CI: 3.41–7.27)20. A multivariate Mendelian randomization analysis found that HDL-C was an independent protective factor for NAFLD (OR: 0.776, 95% CI: 0.604–0.998)26. Although there is no data on the association between the ALT/HDL-C ratio and the likelihood of developing NAFLD, an increase in the ratio indicates either an increase in ALT or a reduction in HDL-C. Consequently, our data support the aforementioned findings that ALT/HDL-C ratio levels are substantially correlated with NAFLD. What’s more, the sensitivity analysis showed that this link is still present in people with TG < 1.7 mmol/L or BMI < 24 kg/m2. The above results have demonstrated the consistency of the correlation between the ALT/HDL-C ratio and NALFD risk. This discovery offers a justification for mitigating the likelihood of NAFLD by decreasing the ALT/HDL-C ratio. Furthermore, we assessed the predictive capacity of the ALT/HDL-C ratio, HDL-C, and ALT for NAFLD using a ROC curve. We determined that the ALT/HDL-C ratio exhibited superior predictive ability compared to ALT or HDL-C in isolation. An elevated ALT/HDL-C ratio signifies an elevated risk of developing NAFLD. A higher ALT/HDL-C ratio during the follow-up period indicates an elevated risk of developing NAFLD, alerting individuals to modify their lifestyle choices to reduce the incidence of NAFLD proactively.
Uncertainty surrounds the correlation between an elevated ALT/HDL-C ratio and NAFLD. There are, however, two explanations that could fit this event. First, research has demonstrated that high ALT is linked to metabolic syndrome and insulin resistance37,38. NAFLD is significantly impacted by insulin resistance39,40. As a result, ALT may affect NAFLD development by influencing insulin resistance. Given the significant role of oxidative stress in the onset and advancement of non-alcoholic fatty liver disease41, it is implied that the potential involvement of HDL-C's antioxidant activity may be involved in the pathophysiology of non-alcoholic fatty liver disease42. A high ratio of alanine ALT to HDL-C levels, characterized by reduced HDL-C and elevated ALT, may indicate NAFLD.
The ALT/HDL-C ratio and incident NAFLD were shown to have a non-linear correlation using a two-piecewise Cox proportional hazards regression model in the current investigation. The inflection point for the ALT/HDL-C ratio was 12.963 after adjusting confounding factors. It was discovered that when the ALT/HDL-C ratio was less than 12.963, every additional unit was linked to a 20.4% higher incident NAFLD. However, when the ALT/HDL-C ratio was above 12.963, a 1 unit increase was related to a 2.3% higher incident NAFLD. In Table S1, the current research demonstrated that subjects with an ALT/HDL-C ratio ≤ 12.963 had a low proportion of females and lower BMI, SBP, DBP, AST, ALP, GGT, UA, and LDL-C. However, the abovementioned factors highly correlated with NAFLD19. The impact of the ALT/HDL-C ratio on NAFLD was minimal when it was more than 12.963. Conversely, the risk factors associated with NAFLD were mitigated and exhibited diminished impact when the ALT/HDL-C ratio was below 12.963. At this juncture, the effect of the ALT/HDL-C ratio was significantly amplified. It has important clinical ramifications because ALT/HDL-C and NAFLD have a curvilinear correlation. When we reduced the non-obese subjects' ALT/HDL-C ratio to below 12.963 with treatments, the risk of NAFLD was reduced. Additionally, NAFLD events decreased more quickly when the ALT/HDL-C ratio decreased when it was below 12.963. The current research provides a valuable tool for clinicians to enhance consultation and improve NAFLD preventive decision-making.
The following are some of this study's advantages. (1) The sample size we used was sizable. (2) Notably, this is the first investigation to examine the correlation between ALT/HDL-C and NAFLD. (3) Strict statistical modifications were applied to reduce residual confounding variables. (4) Multiple imputations were employed to address missing data. This approach can increase statistical power while reducing bias that might result from missing covariate data. (5) we conducted several sensitivity analyses and subgroup analyses to assess the robustness of the research’s findings.
The present investigation is subject to certain limitations. First, due to its observational nature, it could not pinpoint the causal association with any degree of precision. Second, the correlation between ALT/HDL-C ratio and NAFLD in subjects with low-density lipoprotein cholesterol over 3.12 mmol/L or BMI over 25 kg/m2 remains unclear. This is not clear about the connection between ALT/HDL-C ratio and NAFLD in subjects with LDL-C over 3.12 mmol/L or BMI over 25 kg/m2. In the future, we may think about planning our trials and enlisting everyone, including patients who are lean and non-lean and who have normal and abnormal LDL-C values. Third, despite the consideration of known potential confounders, unmeasured confounders may still be present, as is typical of observational studies. Fourth, the current investigation solely assessed baseline levels of ALT, HDL-C, and other variables, without accounting for potential fluctuations in the ALT/HDL-C ratio over time. Fifth, due to its limited sensitivity, ultrasonography is not the gold standard for diagnosing NALFD. In the future, we can create our research to identify NAFLD using better techniques, including elastography.
Conclusion
The present investigation shows a positive and non-linear association between the ALT/HDL-C ratio and NAFLD in lean Chinese individuals with a normal range of LDL-C. The relationship between the ALT/HDL-C ratio and NAFLD also has a threshold effect. The risk of developing NAFLD significantly correlates with the ALT/HDL-C ratio when it is less than 12.963. Therefore, the current study advises enhancing clinician consultation and decision-making for NAFLD prevention. Consequently, to reinforce the credibility of employing the ALT/HDL-C ratio as a conventional clinical metric for the early identification and implementation of intervention strategies in NAFLD, particularly regarding its applicability in lean cohorts, we recommend the commencement of prospective studies in real-world settings.
Data availability
The authors confirm that the data supporting the findings of this study are available within the article [and/or its supplementary materials].
Abbreviations
- ALT/HDL-C ratio:
-
Alanine aminotransferase to high-density lipoprotein cholesterol ratio
- BMI:
-
Body mass index
- SBP:
-
Systolic blood pressure
- DBP:
-
Diastolic blood pressure
- ALT:
-
Alanine aminotransferase
- AST:
-
Aspartate aminotransferase
- GGT:
-
Gamma-glutamyl transferase
- ALP:
-
Alkaline phosphatase
- LDL-C:
-
Low-density lipoprotein cholesterol
- HDL-C:
-
High-density lipoprotein cholesterol
- TC:
-
Total cholesterol
- TG:
-
Triglycerides
- FPG:
-
Fasting plasma glucose
- UA:
-
Uric acid
- Cr:
-
Creatinine
- IR:
-
Insulin resistance
- GAM:
-
Generalized additive models
- T2DM:
-
Type 2 diabetes mellitus
- NAFLD:
-
Nonalcoholic fatty liver disease
- HR:
-
Hazard ratio
- SD:
-
Standard deviations
- CI:
-
Confidence interval
References
Hijona, E., Hijona, L., Arenas, J. I. & Bujanda, L. Inflammatory mediators of hepatic steatosis. Mediat. Inflamm. 2010, 837419. https://doi.org/10.1155/2010/837419 (2010).
Kanwal, F. et al. Risk of hepatocellular cancer in patients with non-alcoholic fatty liver disease. Gastroenterology 155(6), 1828-1837.e2. https://doi.org/10.1053/j.gastro.2018.08.024 (2018).
Kodama, K. et al. Clinical features of hepatocellular carcinoma in nonalcoholic fatty liver disease patients without advanced fibrosis. J. Gastroenterol. Hepatol. 34(9), 1626–1632. https://doi.org/10.1111/jgh.14608 (2019).
Fabbrini, E., Sullivan, S. & Klein, S. Obesity and nonalcoholic fatty liver disease: Biochemical, metabolic, and clinical implications. Hepatology 51(2), 679–689. https://doi.org/10.1002/hep.23280 (2010).
Wei, J. L. et al. Prevalence and severity of nonalcoholic fatty liver disease in non-obese patients: A population study using proton-magnetic resonance spectroscopy. Am. J. Gastroenterol. 110(9), 1306–1314. https://doi.org/10.1038/ajg.2015.235 (2015) (quiz 1315).
Liu, C. J. Prevalence and risk factors for non-alcoholic fatty liver disease in Asian people who are not obese. J. Gastroenterol. Hepatol. 27(10), 1555–1560. https://doi.org/10.1111/j.1440-1746.2012.07222.x (2012).
Das, K. et al. Nonobese population in a developing country has a high prevalence of nonalcoholic fatty liver and significant liver disease. Hepatology 51(5), 1593–1602. https://doi.org/10.1002/hep.23567 (2010).
Abenavoli, L. et al. Ultrasound prevalence and clinical features of nonalcoholic fatty liver disease in patients with inflammatory bowel diseases: A real-life cross-sectional study. Medicina (Kaunas) 59(11), 1935. https://doi.org/10.3390/medicina59111935 (2023).
Lazo, M. et al. Prevalence of nonalcoholic fatty liver disease in the United States: The Third National Health and Nutrition Examination Survey, 1988–1994. Am. J. Epidemiol. 178(1), 38–45. https://doi.org/10.1093/aje/kws448 (2013).
Albhaisi, S., Chowdhury, A. & Sanyal, A. J. Non-alcoholic fatty liver disease in lean individuals. JHEP Rep. 1(4), 329–341. https://doi.org/10.1016/j.jhepr.2019.08.002 (2019).
Fan, J. G., Kim, S. U. & Wong, V. W. New trends on obesity and NAFLD in Asia. J. Hepatol. 67(4), 862–873. https://doi.org/10.1016/j.jhep.2017.06.003 (2017).
VanWagner, L. B. & Armstrong, M. J. Lean NAFLD: A not so benign condition?. Hepatol. Commun. 2(1), 5–8. https://doi.org/10.1002/hep4.1143 (2018).
Hagstrom, H. et al. Risk for development of severe liver disease in lean patients with nonalcoholic fatty liver disease: A long-term follow-up study. Hepatol. Commun. 2(1), 48–57. https://doi.org/10.1002/hep4.1124 (2018).
Yoshitaka, H. et al. Nonoverweight nonalcoholic fatty liver disease and incident cardiovascular disease: A post hoc analysis of a cohort study. Medicine (Baltimore) 96(18), e6712. https://doi.org/10.1097/MD.0000000000006712 (2017).
Fukuda, T. et al. The impact of non-alcoholic fatty liver disease on incident type 2 diabetes mellitus in non-overweight individuals. Liver Int. 36(2), 275–283. https://doi.org/10.1111/liv.12912 (2016).
Imajo, K. et al. LDL-migration index (LDL-MI), an indicator of small dense low-density lipoprotein (sdLDL), is higher in non-alcoholic steatohepatitis than in non-alcoholic fatty liver: A multicenter cross-sectional study. PLoS One 9(12), e115403. https://doi.org/10.1371/journal.pone.0115403 (2014).
Norris, A. L. et al. Circulating oxidized LDL and inflammation in extreme pediatric obesity. Obesity (Silver Spring) 19(7), 1415–1419. https://doi.org/10.1038/oby.2011.21 (2011).
Sun, D. Q. et al. Increased levels of low-density lipoprotein cholesterol within the normal range as a risk factor for nonalcoholic fatty liver disease. Oncotarget 7(5), 5728–5737. https://doi.org/10.18632/oncotarget.6799 (2016).
Li, Q., Han, Y., Hu, H. & Zhuge, Y. Gamma-glutamyl transferase to high-density lipoprotein cholesterol ratio has a non-linear association with non-alcoholic fatty liver disease: A secondary prospective cohort study in non-obese Chinese adults. Front. Med. (Lausanne) 9, 995749. https://doi.org/10.3389/fmed.2022.995749 (2022).
Wang, M. et al. A combined association of serum uric acid, alanine aminotransferase and waist circumference with non-alcoholic fatty liver disease: A community-based study. PeerJ 10, e13022. https://doi.org/10.7717/peerj.13022 (2022).
Cruz, M. A. et al. Association of the nonalcoholic hepatic steatosis and its degrees with the values of liver enzymes and homeostasis model assessment-insulin resistance index. Gastroenterol. Res. 8(5), 260–264. https://doi.org/10.14740/gr685w (2015).
Mansour-Ghanaei, R., Mansour-Ghanaei, F., Naghipour, M. & Joukar, F. Biochemical markers and lipid profile in nonalcoholic fatty liver disease patients in the PERSIAN Guilan cohort study (PGCS), Iran. J. Family Med. Prim. Care 8(3), 923–928. https://doi.org/10.4103/jfmpc.jfmpc_243_18 (2019).
Tziomalos, K. High-density lipoprotein: Quantity or quality?. J. Thorac. Dis. 8(11), 2975–2977. https://doi.org/10.21037/jtd.2016.11.67 (2016).
Alberti, K. G. et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 120(16), 1640–1645. https://doi.org/10.1161/CIRCULATIONAHA.109.192644 (2009).
Socha, P. et al. Nonalcoholic fatty liver disease as a feature of the metabolic syndrome. Rocz Panstw Zakl Hig 58(1), 129–137 (2007).
Xie, J. et al. The associations between modifiable risk factors and nonalcoholic fatty liver disease: A comprehensive Mendelian randomization study. Hepatology 77(3), 949–964. https://doi.org/10.1002/hep.32728 (2023).
Cao, C. et al. The nonlinear correlation between alanine aminotransferase to high-density lipoprotein cholesterol ratio and the risk of diabetes: A historical Japanese cohort study. BMC Endocr. Disord. 23(1), 124. https://doi.org/10.1186/s12902-023-01382-7 (2023).
Sun, D. Q. et al. Association of low-density lipoprotein cholesterol within the normal range and NAFLD in the non-obese Chinese population: A cross-sectional and longitudinal study. BMJ Open 6(12), e013781. https://doi.org/10.1136/bmjopen-2016-013781 (2016).
Zeng, M. D. et al. Guidelines for the diagnosis and treatment of nonalcoholic fatty liver diseases. J. Dig. Dis. 9(2), 108–112. https://doi.org/10.1111/j.1751-2980.2008.00331.x (2008).
Groenwold, R. H. et al. Missing covariate data in clinical research: When and when not to use the missing-indicator method for analysis. CMAJ 184(11), 1265–1269. https://doi.org/10.1503/cmaj.110977 (2012).
White, I. R., Royston, P. & Wood, A. M. Multiple imputation using chained equations: Issues and guidance for practice. Stat. Med. 30(4), 377–399. https://doi.org/10.1002/sim.4067 (2011).
Li, J. et al. Effects of childhood body size on breast cancer tumour characteristics. Breast Cancer Res. 12(2), R23. https://doi.org/10.1186/bcr2564 (2010).
Lee, J. H., Lee, H. S., Cho, A. R., Lee, Y. J. & Kwon, Y. J. Non-alcoholic fatty liver disease is an independent risk factor for LDL cholesterol target level. Int. J. Environ. Res. Public Health 18(7), 3442. https://doi.org/10.3390/ijerph18073442 (2021).
Rothenbacher, D. et al. Contribution of cystatin C- and creatinine-based definitions of chronic kidney disease to cardiovascular risk assessment in 20 population-based and 3 disease cohorts: The BiomarCaRE project. BMC Med. 18(1), 300. https://doi.org/10.1186/s12916-020-01776-7 (2020).
Cramer, D. W., Vitonis, A. F., Terry, K. L., Welch, W. R. & Titus, L. J. The association between talc use and ovarian cancer: A retrospective case-control study in two US states. Epidemiology 27(3), 334–346. https://doi.org/10.1097/EDE.0000000000000434 (2016).
Hou, X. H. et al. Non-alcoholic fatty liver disease’s prevalence and impact on alanine aminotransferase associated with metabolic syndrome in the Chinese. J. Gastroenterol. Hepatol. 26(4), 722–730. https://doi.org/10.1111/j.1440-1746.2010.06509.x (2011).
Vozarova, B. et al. High alanine aminotransferase is associated with decreased hepatic insulin sensitivity and predicts the development of type 2 diabetes. Diabetes 51(6), 1889–1895. https://doi.org/10.2337/diabetes.51.6.1889 (2002).
Sookoian, S. & Pirola, C. J. Alanine and aspartate aminotransferase and glutamine-cycling pathway: Their roles in pathogenesis of metabolic syndrome. World J. Gastroenterol. 18(29), 3775–3781. https://doi.org/10.3748/wjg.v18.i29.3775 (2012).
Hwang, K. A., Hwang, Y. J., Kim, G. R. & Choe, J. S. Extracts from Aralia elata (Miq) seem alleviate hepatosteatosis via improving hepatic insulin sensitivity. BMC Complement Altern. Med. 15, 347. https://doi.org/10.1186/s12906-015-0871-5 (2015).
Musso, G., Gambino, R., Cassader, M. & Pagano, G. A meta-analysis of randomized trials for the treatment of nonalcoholic fatty liver disease. Hepatology 52(1), 79–104. https://doi.org/10.1002/hep.23623 (2010).
Sakaida, I. & Okita, K. The role of oxidative stress in NASH and fatty liver model. Hepatol. Res. 33(2), 128–131. https://doi.org/10.1016/j.hepres.2005.09.019 (2005).
Karami, S. et al. Association of anti-oxidative capacity of HDL with subclinical atherosclerosis in subjects with and without non-alcoholic fatty liver disease. Diabetol. Metab. Syndr. 13(1), 121. https://doi.org/10.1186/s13098-021-00741-5 (2021).
Funding
This study was supported by the Natural Science Funding of China (No. 82272598, No. 81901470), and the Natural Science Foundation of Guangdong Province, China (No. 2020A1515011203). This study was also supported by the Science, Technology, and Innovation Commission of Shenzhen (JCYJ20210324135804012, JCYJ20220530150407015).
Author information
Authors and Affiliations
Contributions
Changchun Cao, Zihe Mo, and Yong Han contributed to the study concept and design, researched and interpreted the data, and drafted the manuscript. Jiao Luo, Haofei Hu, and Yongcheng He analyzed the data and reviewed the manuscript. Changchun Cao, Zihe Mo, and Yong Ha oversaw the project’s progress, contributed to the discussion and reviewed the manuscript. Dehua Yang provided great help in responding to the reviewers and made important contributions regarding language quality, grammar, and syntax. Jiao Luo, Haofei Hu, and Yongcheng He are the guarantors of this work and, as such, had full access to all the data in the study and took responsibility for the data’s integrity and the data analysis’s accuracy. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Cao, C., Mo, Z., Han, Y. et al. Association between alanine aminotransferase to high-density lipoprotein cholesterol ratio and nonalcoholic fatty liver disease: a retrospective cohort study in lean Chinese individuals. Sci Rep 14, 6056 (2024). https://doi.org/10.1038/s41598-024-56555-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-024-56555-8
Keywords
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
