
Abstract
We have previously reported that 12p gain may predict the presence of malignant components and poor prognosis for CNS germ cell tumor (GCT). Recently, 3p25.3 gain was identified as an independent predictor of poor prognosis for testicular GCT. Eighty-one CNS GCTs were analyzed. Copy number was calculated using methylation arrays. Five cases (6.2%) showed 3p25.3 gain, but only among the 40 non-germinomatous GCTs (NGGCTs) (5/40, 12.5%; p = 0.03). Among NGGCTs, those with a yolk sac tumor component showed a significantly higher frequency of 3p25.3 gain (18.2%) than those without (1.5%; p = 0.048). NGGCTs with gain showed significantly shorter progression-free survival (PFS) than those without (p = 0.047). The 3p25.3 gain and 12p gain were independent from each other. The combination of 3p25.3 gain and/or 12p gain was more frequent among NGGCTs with malignant components (69%) than among those without (29%; p = 0.02). Germinomas containing a higher number of copy number alterations showed shorter PFS than those with fewer (p = 0.03). Taken together, a finding of 3p25.3 gain may be a copy number alteration specific to NGGCTs and in combination with 12p gain could serve as a marker of negative prognosis or treatment resistance. Germinoma with frequent chromosomal instability may constitute an unfavorable subgroup.
Similar content being viewed by others

Introduction
Germ cell tumors (GCTs) occur in various organs in the body, mainly in the gonads (testis and ovary), but also in midline structures such as brain, mediastinum and sacrococcygeal regions1. Extragonadal GCT is hypothesized to develop from a mis-migrated primordial germ cell (PGC), which is pluri- or toti-potent2. Central nervous system (CNS) GCTs are mostly categorized as type II when classified according to the seven types of developmental potential. Type II GCTs comprise CNS GCTs and testicular and ovarian GCTs1. The transcriptome and methylation studies comparing CNS and testicular GCTs (TGCTs) have revealed close similarities between germinoma and seminoma, as well as non-germinomatous GCTs (NGGCTs) and non-seminomatous GCTs (NSGCTs), with some diversity between NGGCT and NSGCT in the expression profiles3. Copy number alterations appear more pronounced in TGCTs than in CNS GCTs, although the overall profiles show much in common. Thus, these molecular findings corroborate the concept that gonadal and extra-gonadal GCTs are biologically akin to each other. However, the impact of biological findings on clinical phenotypes leaves much to be clarified.
CNS GCTs are treated with platinum-based chemotherapy and radiation therapy, with surgical resection reserved for mature teratoma, unresponsive or remnant tissue after chemotherapy and/or radiation therapy, or biopsy for diagnostic purposes4,5,6,7,8,9. With the exception of some modifications in chemotherapy intensity, radiation dose and coverage in view of the tumor response to initial treatment, treatment regimens are basically homogeneous without stratification into each germinoma and NGGCT subgroup10,11,12,13,14. We have previously reported that 12p gain may predict the presence of malignant components and poor prognosis in CNS GCTs15. High tumor cell content and atypical location in germinoma cases, and 12p gain in NGGCT cases have been demonstrated as candidate factors for poor prognosis. The identification of age < 6 years old and exceptionally high tumor marker level (AFP > 1000 ng/ml) as poor prognostic factors was an important advance4. High tumor cell content and atypical location have also been demonstrated as poor prognostic factors in germinoma cases8,15,16,17. However, treatment is still generally homogeneous except for distinguishing germinoma or NGGCTs, so further investigations are necessary to identify biomarkers for risk stratification.
A recent study demonstrated that 3p25.3 copy number gain had histological and clinical significance for testicular and mediastinal GCTs in male patients18. In that study, 3p25.3 copy number gain calculated based on methylation array was associated with cisplatin resistance in GCT cell lines, non-seminomatous histology (particularly yolk sac tumor), and significantly poorer progression-free survival (PFS) and overall survival (OS). The authors suggested that 3p25.3 copy number status could be incorporated into risk classifications18.
In light of these findings, we revisited copy number alterations in CNS GCTs and explored their impact on histological malignancy and prognosis. Here, using a cohort of 81 CNS GCT cases with various histological subtypes, we investigated the histological and clinical significance of 3p25.3 copy number profile with the aim of validating this potential risk predictor. We further extended the study to investigate the importance of total numbers of gains and losses genome-wide to assess the prognostic impact on CNS GCTs.
Materials and methods
Patients and histopathological diagnoses
A total of 82 CNS GCTs from 11 institutions underwent central histopathological review by an expert neuropathologist (YN) and were diagnosed as primary (not metastatic) CNS GCTs. Among these, tissues from 16 cases were obtained at recurrence. The cohort was identical to that in a previously published study15. Clinical information such as age, sex, tumor location, treatment and follow-up data were as previously published15. Histopathological breakdown was as follows: 42 germinomas; 22 mixed GCTs; 7 mature teratomas (MTs); 4 immature teratomas (ImTs); 5 yolk sac tumors (YSTs); one embryonal carcinoma (EC); and one choriocarcinoma (CC). With some variability between institutions, treatment regimens were generally based on histopathological diagnoses classifying patients into three risk groups: germinoma group; intermediate prognosis group; and poor prognosis group7. Except for MT cases, all cases received platinum-based chemotherapy and radiation therapy at different intensities, according to the above three risk groups. The intermediate prognosis group included ImTs, teratomas with somatic malignancy, and mixed tumors composed mainly of germinoma or teratoma. The poor prognosis group included so-called malignant GCTs (namely CC, YST and EC) and mixed tumors mainly composed of these histological components. Chemotherapy and radiation dose and coverage have been described previously8.
This study was approved by the ethics committee at Juntendo University, Tokyo, Japan (Approval No. M20-0295, informed consent was waived from study participants) and the respective local institutional review boards. All experiments were performed in accordance with relevant guidelines and regulations.
Molecular data
DNA methylation data obtained using Illumina Infinium Human Methylation450 BeadChips (450 K, Illumina, San Diego, CA, USA) for all 82 cases19, as well as somatic mutation data obtained by whole-exome or target sequencing for 81 of the 82 cases were used in the current analyses20. One case (GCT83, germinoma) was omitted from further analyses, because the quality of the sample was deemed low, considering that the average detection p value of all the probes across chromosomes calculated using the package minfi (version 1.44.0) was greater than 0.001. Copy number calculation was carried out using the conumee package run in the R statistical environment (version 4.0.2), as described previously15, with modifications in the steps of raw data preprocessing and combining probes into bins to align with the preceding study in the testicular GCTs18. Methylation array probes in the region of 3p25.3 (chr3:8,700,001–11,800,000, HG19) were aggregated into 25 bins (specified as such with at least 25 probes, otherwise settings were default). Regarding the definition of copy number gain, cases with any segment that showed a log2ratio higher than 0.1 within this region (3p25.3; chr3:8,700,001–11,800,000, HG19) were counted as positive for gain, according to the aforementioned publication18. The data regarding 12p status were as published15. The data regarding mutational status were as published20.
The number of segments in which the average value of log2ratio CN was higher than 0.1 (gain) or lower than − 0.1 (loss) was counted in each case.
Statistical analysis
Non-parametric values were compared using Wilcoxon’s test. Categorical data were compared between subgroups using Fisher’s exact test. Survival data were analyzed using the log-rank test and the results are shown as Kaplan–Meier curves. Cox proportional hazard models were used for multivariate survival analysis. All statistical analyses were carried out using JMP® 16 (SAS Institute Inc., Cary, NC, USA). Values of p < 0.05 were considered statistically significant.
Ethics statement
This study was approved by the ethics committee at Juntendo University, Tokyo, Japan (Approval No. M20-0295) and the respective local institutional review boards.
Informed consent
Patient consent was waived due to this study being minimal-risk retrospective review.
Results
Copy number status and histological classification
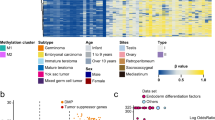
A copy number gain for chromosome 3p25.3 was identified in 5 of the 81 cases (6.2%) (Fig. 1A,B). With the exception of one case (GCT65: YST), the other 4 cases showed 3p whole-chromosomal arm gain, as shown in Fig. 1. Histopathological diagnoses for these five cases were: one YST; one mixed GCT (germinoma + MT + YST + EC); two high-grade GCTs; and one ImT. Gain was observed exclusively in NGGCTs (12.5%), not in germinomas (0%; p = 0.03) (Fig. 1C). Correlating with histopathological components, the presence of a YST component was positively associated with the presence of gain (2/11 cases with YST component vs 1/69 cases without YST component; p = 0.049). The remaining two cases were high-grade GCTs without further histological specifications. No correlation was observed for any other histopathological component. While the gain was more prevalent among recurrent GCTs in testicular cases, no such correlation was found in CNS NGGCTs (4/30 primary tumors vs. 1/10 recurrent tumors) (Fig. 1D).

(A) Copy number plots for 5 cases with 3p25.3 gain. The 4 cases other than GCT65 showed 3p chromosomal arm gains. (B) Heatmap of copy number status within the region of 3p25.3 for the 5 cases acknowledged as harboring a gain. (C) Distribution of 3p25.3 gain by histopathological classification. A significantly higher prevalence of 3p25.3 gain was observed in NGGCT cases compared with germinoma cases (p = 0.03). (D) Distribution of 3p25.3 gain according to primary or recurrent status of the tissues. No difference was observed between groups.
Correlation with mutation profile and 12p gain
The relationship between the presence of mutation in either of the MAPK or PI3K pathways and the presence of copy number gain was investigated in 39 NGGCT cases (mutation information was not available for one case). Mutation in the above two pathways was found in 11 and 4 of the 39 cases, respectively. The 3p25.3 gain was almost evenly distributed, regardless of mutation status (1/11 vs. 4/28, p = 1.0 in the MAPK pathway; 1/4 vs. 4/35, p = 0.44 in the PI3K pathway). Of note, 3p25.3 gain was mutually exclusive with KIT mutation, with 3p25.3 gain observed only in KIT-wildtype cases (5/35 cases) and not in any KIT-mutant cases (0/4 cases), although the frequency of the two genetic events was not significantly correlated, mainly due to the sample size.
In our previous study, 12p gain was identified as a marker for NGGCT histology15. No association was seen between 3p25.3 gain and 12p gain among NGGCT cases (3p25.3 gain: 2/20 12p-neutral cases vs 3/20 12p-gain cases; p = 1.0). Combining 12p gain and 3p25.3 gain, the prevalence of these abnormalities among NGGCT cases was 55% (22/40), and the association with NGGCT was more robust (p < 0.0001) than that for 12p gain alone (p = 0.0002). These abnormalities were found at higher frequency among NGGCT cases with malignant components (18/26, 69%) than among those without (4/14, 29%; p = 0.02) (Supplementary Fig. 1).
Prognostic significance of 3p25.3 gain
Survival analyses were performed for 30 primary NGGCT cases. PFS was significantly shorter in cases with 3p25.3 gain (p = 0.047) (Fig. 2A). Cases with 3p25.3 gain tended to have a shorter OS compared with cases without 3p25.3 gain, but the difference was not significant (p = 0.14) (Fig. 2B).

(A) Progression-free survival (PFS) among 30 cases of primary (not recurrent) non-germinomatous GCTs was compared between cases with and without 3p25.3 gain. Those with 3p25.3 gain showed significantly shorter PFS than those without (p = 0.047). (B) Comparison of overall survival (OS) among 30 cases of primary (not recurrent) non-germinomatous GCTs between cases with and without 3p25.3 gain. No significant difference was found, although a trend was seen toward shorter OS in cases with 3p25.3 gain.
Genome-wide chromosomal aberrations
Next, we interrogated genome-wide copy number changes and investigated whether copy number profile was linked with histopathology and prognosis from a broader perspective. Based on the copy number profiles calculated using the R conumee package under the settings described above, the number of segments across autosomal chromosomes with gains and losses was counted in all 81 cases. The number of altered segments tended to be slightly higher in NGGCT cases compared with germinoma cases, although the difference was not significant (9.5 vs. 13.0 on average, p = 0.09) (Fig. 3A). Among primary germinoma cases (n = 33), most cases displayed fewer copy number alterations (number of altered segments < 10, “stable chromosome”, n = 22), while a minority of cases harbored a higher number of alteration (> 10, “unstable chromosome”, n = 11) (Fig. 3B). Germinoma cases with stable chromosomes showed longer PFS than cases with unstable chromosomes (p = 0.03) (Fig. 3C). As only one death was recorded among germinoma cases, the association with OS could not be investigated. In addition, no significant correlation was found for prognosis in relation to chromosomal instability in NGGCTs, although similar trends in both PFS and OS were observed (Supplementary Fig. 2A,B).

(A) Number of altered (gain and loss) segments in copy number analyses of 81 germinoma and non-germinomatous GCT (NGGCT) cases. The number of altered copy number segments tended to be slightly higher in NGGCT cases than in germinoma cases, but the difference was not significant. (B) The number of altered copy number segments in germinoma displayed in a histogram. The distribution shows that most cases had a small number of altered segments (< 10, n = 22, stable), although a subgroup showed a high number of alterations (> 10, n = 11, unstable). (C) Germinoma cases with a more than 10 altered copy number segments showed shorter progression-free survival (PFS) than other cases.
As germinoma is known to have a variable degree of tumor cell content in their tissue, wherein a subgroup of cases were enriched with a high amount of lymphocytes, a lower log2CN threshold at 0.05 was attempted, and the prognosis was evaluated. As the median number of altered segments using this threshold was 15, germinoma cases were divided into two cohorts, like above. The analysis demonstrated a slightly worse PFS in cases with a higher number of altered segments than those with fewer. However, there was no statistical significance (p = 0.13, Supplementary Fig. 3A,B). The fraction of the genome altered (FGA) was computed across the genome21; the sum of the coverage of a bin (bases) above or below a log2CN threshold (0.1 or 0.05) was divided by the entire genome. When the threshold of 0.1 was used, the median FGA was 20.2%, and germinoma cases with a higher FGA demonstrated a slightly worse PFS than otherwise, and the difference was not significant (p = 0.20, Supplementary Fig. 3C,D). When the 0.05 threshold was used, the median FGA was 48.9%, and again, the PFS was not statistically different (p = 0.29, Supplementary Fig. 3E,F).
Tumor cell content was proportional to FGA. The R-squared values in a linear regression model were 0.39 when log2 CN ratio of 0.1 and 0.05 was applied. As a tumor cell content of ≥ 50% was proven to be a poor prognostic indicator in germinoma cases17, PFS was assessed using tumor cell content (≥ 50% or < 50%) and the number of altered segments (≥ 10 or < 10) as variables in the Cox regression analysis. This showed that neither of the two factors demonstrated statistical significance, with p values 0.21 and 0.09, respectively.
Discussion
This study aimed to investigate the impact of copy number alterations on histopathology, platinum-resistance and prognosis in CNS GCTs. We found that 3p25.3 gain correlated with the histopathological diagnosis of NGGCT, presence of a YST histological component among NGGCTs, and shorter PFS. However, the finding that 3p25.3 gain was related to chemotherapy-resistance, which would have been represented by the presence of 3p25 gain in recurrent tumor tissues following platinum-based chemotherapy, was not evident in the current CNS GCT cohort.
The hypothesis about the cell of origin for GCTs stands for PGC, and extragonadal GCTs (including CNS and mediastinal GCTs) are hypothesized to originate from mis-migrated PGCs2,19,20,22,23,24,25. In addition to the morphological similarities between gonadal and extra-gonadal GCTs from histopathological observations, these tumors are reported to be at least partly akin in terms of molecular findings, such as mutational profiles, copy number alterations, methylation status and transcriptomes26,27,28,29,30,31. Under these circumstances, gonadal and extra-gonadal GCTs would fall into the same category of type I or II GCT1. In contrast, a previous transcriptome study revealed that CNS and testicular GCTs were clustered differently in a dimensionality reduction method, implying the presence of unique characteristics according to the site of occurrence3. Furthermore, the same study comparing CNS and testicular GCTs also showed that copy number alterations were more enhanced in testicular GCTs than CNS GCTs3. This study revealed that the 3p25.3 gain may have clinical and histopathological significance in CNS GCTs as in mediastinal and testicular GCTs in part, which may corroborate the existence of shared biological properties between CNS and gonadal GCTs. Nonetheless, the almost equal presence of 3p25.3 gains in primary and recurrent CNS GCTs contrasted with findings in mediastinal and testicular GCTs, where the gain was significantly more prevalent for recurrent tumors. Our results suggest the possibility of site-dependent features of GCTs. Furthermore, the close association between the presence of a YST component as histopathology and 3p25.3 gain suggests that this gain may be a characteristic of Type I GCT, which occurs in neonates and children less than 6 years of age and is histopathologically YST and immature teratoma. The five cases with 3p25.3 gain in the current cohort demonstrated an age range of 2, 16, 16, 19, and 20 years. Although the two cases were diagnosed as high-grade GCTs in the central histopathology review, all the cases had either YST or immature teratoma components in the original histopathology diagnoses in local institutions. The five cases did not match the typical Type I GCT profile, and further investigation is warranted.
In our cohort, 4 of 5 cases with 3p25.3 gain also harbored entire 3p gain. The preceding study of testicular GCTs also showed that many of the samples with 3p25.3 gain appeared to have concomitant 3p gain (11 of 15 per figure)18. The study demonstrated the presence of cisplatin resistance in cell lines with 3p25.3; however, further functional study is warranted to prove the significance of the specific region of 3p25.3 gain in tumor biology.
We have previously reported finding 12p gain at a higher frequency in NGGCTs compared with germinoma, particularly in those with a malignant component15. Accordingly, the relationship between copy number gain of 3p25.3 and 12p gain was investigated. Among the 20 NGGCT cases with 12p gain, 3 cases showed concomitant 3p25.3 gain. This association was not significant (p = 1.0). These two copy number gains thus appear to have independent biological significance. By combining 12p gain and 3p25.3 gains, copy number gains were more closely associated with NGGCT cases, particularly those with malignant components, than each single gain alone.
The present findings also suggested that germinoma cases with a higher number of chromosomal aberrations may manifest shorter PFS (Fig. 3C). One marker-positive case was identified in each of the chromosome-stable and chromosome-unstable groups (GCT91: CSF HCG 58 IU/l and GCT19: serum HCG 61.7 IU/l, respectively), and did not appear to have contributed to prognostic differences. Gain in 12p was more frequent in chromosome-unstable germinoma cases (28.6% vs. 3.7%, p = 0.04). No association was found with mutation frequency in the MAPK or PI3K pathways. Germinoma was previously shown to be subdivided into two clusters based on the copy number profile; cases with abundant aberrations across chromosomes, and other cases with few aberrations31. Genome-wide hypomethylation including retrotransposons, typically found in germinomas, as well as high expression of embryonic microRNAs, both of which may contribute to genomic instability1,19,32. Chromosomal instability, represented as aneuploidy, has been shown to be associated with metastasis, immune evasion and therapeutic resistance, leading to poor prognosis in many cancer types33,34. Collectively, germinoma cases with chromosomal instability might constitute a subgroup with poor prognosis warranting more intensive treatment compared to most other cases that are sensitive to standard chemotherapy and radiation therapy. However, using a different log2CN threshold or fraction of the genome altered to divide the cohort, the difference in prognosis was not significant. Furthermore, chromosomal instability appeared to be related to tumor cell content. The small number of recurrences (n = 4) out of the cohort (n = 33) may be one of the limitations of the study; further evaluation using a larger cohort would lead to a more solid analysis.
Some CNS GCTs, mostly NGGCTs and a subset of germinomas, show resistance to standard radiation and chemotherapy1,18. These predominantly develop in pediatric and young adult patients, leading to long-term side effects caused by radiation therapy and chemotherapy such as secondary malignancy, intellectual decline, and vascular damage35,36,37,38,39,40. Treatment stratification based on biomarkers is therefore needed. So far, atypical sites of occurrence outside of midline structures (including the neurohypophysis, pineal gland and ventricles), higher tumor cell content in pathological specimens in germinoma, and 12p gain in NGGCTs have been identified as negative prognostic factors15. Based on the present results, chromosomal instability in germinoma and 3p25.3 gain in NGGCTs may also be considered as potential markers of poor prognosis. Further in-depth analysis of the combinations of 3p25.3 gain with other chromosomal aberrations in the entire genome would be worthwhile to interrogate potential prognostic markers. Our study was limited by the small size of the cohort, so the findings need to be validated in a larger cohort as a valid biomarker for future treatment stratification. Furthermore, calculation of copy number can be affected by multiple factors, including parameters used in the R package (minfi, conumee) and the samples used as controls. For instance, the previous study analyzing the identical cohort used different parameters, which resulted in slightly different results for cases having 3p25.3 gain (GCT32 and 65). However, the current study aimed to examine the results obtained in testicular GCTs, so the study used the same parameters as those in the testicular GCT study. A more robust method of copy number calculation is warranted for this gain to be valuable in clinical practice in the future.
In conclusion, we propose 3p25.3 gain as a novel marker to predict malignant components and poor prognosis of CNS GCTs. Chromosomal instability in germinoma may identify cases with poor prognosis. In combination with previously reported 12p gain, this may facilitate patient stratification for treatment and prognostication of CNS GCTs. Validation studies in a larger number of patients are underway.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Oosterhuis, J. W. & Looijenga, L. H. Human germ cell tumours from a developmental perspective. Nat. Rev. Cancer 19, 522–537 (2019).
Oosterhuis, J. W., Stoop, H., Honecker, F. & Looijenga, L. H. Why human extragonadal germ cell tumours occur in the midline of the body: Old concepts, new perspectives. Int. J. Androl. 30, 256–263. https://doi.org/10.1111/j.1365-2605.2007.00793.x (2007).
Takami, H. et al. Transcriptome and methylome analysis of CNS germ cell tumor finds its cell-of-origin in embryogenesis and reveals shared similarities with testicular counterparts. Neuro-oncology 24, 1246–1258 (2022).
Calaminus, G. et al. Outcome of patients with intracranial non-germinomatous germ cell tumors: Lessons from the SIOP-CNS-GCT-96 trial. Neuro-oncology 19, 1661–1672 (2017).
Calaminus, G. et al. SIOP CNS GCT 96: Final report of outcome of a prospective, multinational nonrandomized trial for children and adults with intracranial germinoma, comparing craniospinal irradiation alone with chemotherapy followed by focal primary site irradiation for patients with localized disease. Neuro-oncology 15, 788–796. https://doi.org/10.1093/neuonc/not019 (2013).
Goldman, S. et al. Phase II trial assessing the ability of neoadjuvant chemotherapy with or without second-look surgery to eliminate measurable disease for nongerminomatous germ cell tumors: A Children’s Oncology Group Study. J. Clin. Oncol. 33, 2464–2471. https://doi.org/10.1200/JCO.2014.59.5132 (2015).
Matsutani, M. et al. Primary intracranial germ cell tumors: A clinical analysis of 153 histologically verified cases. J. Neurosurg. 86, 446–455. https://doi.org/10.3171/jns.1997.86.3.0446 (1997).
Takami, H. et al. Integrated clinical, histopathological, and molecular data analysis of 190 central nervous system germ cell tumors from the iGCT Consortium. Neuro-oncology 21, 1565–1577 (2019).
Fangusaro, J. et al. Phase II trial of response-based radiation therapy for patients with localized CNS nongerminomatous germ cell tumors: A Children’s Oncology Group Study. J. Clin. Oncol. 37, 3283–3290 (2019).
Murray, M. J. et al. Consensus on the management of intracranial germ-cell tumours. Lancet Oncol. 16, e470–e477. https://doi.org/10.1016/S1470-2045(15)00244-2 (2015).
Frappaz, D. et al. EANO, SNO and Euracan consensus review on the current management and future development of intracranial germ cell tumors in adolescents and young adults. Neuro-oncology 24, 516–527 (2022).
Takami, H., Nakamura, H., Ichimura, K. & Nishikawa, R. Still divergent but on the way to convergence: Clinical practice of CNS germ cell tumors in Europe and North America from the perspectives of the East. Neuro-Oncol. Adv. https://doi.org/10.1093/noajnl/vdac061 (2022).
Nakamura, H. et al. The Japan society for neuro-oncology guideline on the diagnosis and treatment of central nervous system germ cell tumors. Neuro-oncology 24, 503–515 (2022).
Takami, H. Advances in molecular profiling and developing clinical trials of CNS germ cell tumors: Present and future directions. Curr. Oncol. Rep. 24, 105–112 (2022).
Satomi, K. et al. 12p gain is predominantly observed in non-germinomatous germ cell tumors and identifies an unfavorable subgroup of central nervous system germ cell tumors. Neuro-oncology 24, 834–846 (2022).
Takami, H. et al. Intratumoural immune cell landscape in germinoma reveals multipotent lineages and exhibits prognostic significance. Neuropathol. Appl. Neurobiol. 46, 111–124 (2020).
Takami, H. et al. Low tumor cell content predicts favorable prognosis in germinoma patients. Neuro-oncol. Adv. 3, vdab110 (2021).
Timmerman, D. M. et al. Chromosome 3p25.3 gain is associated with cisplatin resistance and is an independent predictor of poor outcome in male malignant germ cell tumors. J. Clin. Oncol. 40, 3077 (2022).
Fukushima, S. et al. Genome-wide methylation profiles in primary intracranial germ cell tumors indicate a primordial germ cell origin for germinomas. Acta Neuropathol. 133, 445–462. https://doi.org/10.1007/s00401-017-1673-2 (2017).
Ichimura, K. et al. Recurrent neomorphic mutations of MTOR in central nervous system and testicular germ cell tumors may be targeted for therapy. Acta Neuropathol. 131, 889–901. https://doi.org/10.1007/s00401-016-1557-x (2016).
Zhou, J. et al. Analysis of tumor genomic pathway alterations using broad-panel next-generation sequencing in surgically resected lung adenocarcinoma. Clin. Cancer Res. 25, 7475–7484. https://doi.org/10.1158/1078-0432.CCR-19-1651 (2019).
Teilum, G. Classification of endodermal sinus tumour (mesoblatoma vitellinum) and so-called “embryonal carcinoma” of the ovary. Acta Pathol. Microbiol. Scand. 64, 407–429 (1965).
Stevens, L. C. Jr. & Little, C. C. Spontaneous testicular teratomas in an inbred strain of mice. Proc. Natl. Acad. Sci. U. S. A. 40, 1080 (1954).
Hoei-Hansen, C. E. et al. New evidence for the origin of intracranial germ cell tumours from primordial germ cells: Expression of pluripotency and cell differentiation markers. J. Pathol. 209, 25–33. https://doi.org/10.1002/path.1948 (2006).
Wang, L. et al. Novel somatic and germline mutations in intracranial germ cell tumours. Nature 511, 241–245. https://doi.org/10.1038/nature13296 (2014).
Schulte, S. L. et al. CNS germinomas are characterized by global demethylation, chromosomal instability and mutational activation of the Kit-, Ras/Raf/Erk-and Akt-pathways. Oncotarget 7, 55026 (2016).
Hsieh, T.-H. et al. Global DNA methylation analysis reveals miR-214-3p contributes to cisplatin resistance in pediatric intracranial nongerminomatous malignant germ cell tumors. Neuro-oncology 20, 519–530 (2018).
Williams, L. A. et al. Differences in DNA methylation profiles by histologic subtype of paediatric germ cell tumours: A report from the Children’s Oncology Group. Br. J. Cancer 119, 864–872 (2018).
Rijlaarsdam, M. A. et al. Genome wide DNA methylation profiles provide clues to the origin and pathogenesis of germ cell tumors. PLoS ONE 10, e0122146. https://doi.org/10.1371/journal.pone.0122146 (2015).
Wang, H. W. et al. Pediatric primary central nervous system germ cell tumors of different prognosis groups show characteristic miRNome traits and chromosome copy number variations. BMC Genom. 11, 132. https://doi.org/10.1186/1471-2164-11-132 (2010).
Fukushima, S. et al. Mutually exclusive mutations of KIT and RAS are associated with KIT mRNA expression and chromosomal instability in primary intracranial pure germinomas. Acta Neuropathol. 127, 911–925. https://doi.org/10.1007/s00401-014-1247-5 (2014).
Murray, M. J. et al. Clinical utility of circulating miR-371a-3p for the management of patients with intracranial malignant germ cell tumors. Neuro-oncol. Adv. 2, vdaa048 (2020).
Bakhoum, S. F. & Cantley, L. C. The multifaceted role of chromosomal instability in cancer and its microenvironment. Cell 174, 1347–1360 (2018).
Taylor, A. M. et al. Genomic and functional approaches to understanding cancer aneuploidy. Cancer Cell 33, 676–689 (2018).
Takami, H., Perry, A., Graffeo, C. S., Giannini, C. & Daniels, D. J. Novel diagnostic methods and posttreatment clinical phenotypes among intracranial germ cell tumors. Neurosurgery 87, 563–572 (2020).
Acharya, S., DeWees, T., Shinohara, E. T. & Perkins, S. M. Long-term outcomes and late effects for childhood and young adulthood intracranial germinomas. Neuro-oncology 17, 741–746. https://doi.org/10.1093/neuonc/nou311 (2015).
Twitchell, S., Karsy, M., Guan, J., Couldwell, W. T. & Taussky, P. Sequelae and management of radiation vasculopathy in neurosurgical patients. J. Neurosurg. 130, 1889–1897 (2018).
Choudhary, A., Pradhan, S., Huda, M. F., Mohanty, S. & Kumar, M. Radiation induced meningioma with a short latent period following high dose cranial irradiation: Case report and literature review. J. Neurooncol. 77, 73–77. https://doi.org/10.1007/s11060-005-9009-9 (2006).
Pettorini, B. L. et al. Radiation-induced brain tumours after central nervous system irradiation in childhood: A review. Childs Nerv. Syst. 24, 793–805. https://doi.org/10.1007/s00381-008-0631-7 (2008).
Vinchon, M. et al. Radiation-induced tumors in children irradiated for brain tumor: A longitudinal study. Childs Nerv. Syst. 27, 445–453. https://doi.org/10.1007/s00381-011-1390-4 (2011).
Funding
HT received a research grant from Astellas Foundation for Research on Metabolic Disorders, which is no relationship to this work. KI is an endowed chair at Department of Brain Disease Translational Research, Juntendo University Faculty of Medicine supported by Idorsia Pharmaceuticals Japan Ltd. The sponsor has no role whatsoever in this work. KI received research grants unrelated to this work from the following entities: Daiichi Sankyo Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., Riken Genesis CO., LTD., EPS Corporation, Leica Microsystems, Therabiopharma., and SRL Inc., JSPS. The other authors declare no conflicts of interest related to this work. This study was supported by JSPS KAKENHI Grant Number 22K16650, Astellas Foundation for Research on Metabolic Disorders, and by AMED under Grant Number 21ck0106692s0701.
Author information
Authors and Affiliations
Contributions
Conceptualization: H.T., M.N., R.N., K.I. Manuscript Writing: H.T., K.I. Final editing and approval of the manuscript: H.T., K.S., K.F., T.N., S.T., A.M., N.S., T.S., T.Y., K.S., M.K., T.K., T.T., K.T., T.M., M.N., A.A., K.Y., H.T., T.I., K.K., K.Y., K.S., Y.N., M.M., M.N., R.N., K.I.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Takami, H., Satomi, K., Fukuoka, K. et al. Distinct patterns of copy number alterations may predict poor outcome in central nervous system germ cell tumors. Sci Rep 13, 15760 (2023). https://doi.org/10.1038/s41598-023-42842-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-023-42842-3
This article is cited by
-
Advances in genetic abnormalities, epigenetic reprogramming, and immune landscape of intracranial germ cell tumors
Acta Neuropathologica Communications (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
